
Research Article | DOI: https://doi.org/10.31579/2578-8868/230
1 Tingandogo University Hospital, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
2 Yalgado Ouédraogo University Hospital of Ouagadougou, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
3 Sourô Sanou University Hospital of Bobo-Dioulasso, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
4 Health Sciences Research Institute of Ouagadougou, Department of Medical Biology and Public Health, Ouagadougou, Burkina Faso.
*Corresponding Author: Djingri Labodi Lompo, Tingandogo University Hospital, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
Citation: Djingri L. Lompo., Kadari Cissé., Adja M. Ouédraogo., Nagaonlé E. Somé., Ousséni Diallo. et all (2022). Short-Term Prognosis of Patients Hospitalized for Status Epilepticus in Ouagadougou, Burkina Faso. J. Neuroscience and Neurological Surgery. 11(5); DOI:10.31579/2578-8868/230
Copyright: © 2022 Djingri Labodi Lompo, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 07 January 2022 | Accepted: 18 April 2022 | Published: 25 April 2022
Keywords: status epilepticus ; intra hospital mortality ; disability ; altered consciousness
Introduction: Status epilepticus is one of the most common neurological emergency, with high morbidity and mortality and an often poor functional prognosis in survivors. We carried out the present study, to describe the intra-hospital clinical course and to identify the risk factors for intra-hospital death of patients hospitalized for status epilepticus in Ouagadougou, Burkina Faso.
Patients and methods: it was a prospective, cross-sectional, multi-center hospital, descriptive and analytical study, which took place from January 1, 2015 to December 31, 2019, involving patients consecutively hospitalized in the university hospitals of Ouagadougou, for status epilepticus. Sociodemographic characteristics, clinical data on admission, biological assessment on admission, EEG characteristics, brain scan and / or brain MRI results ; etiological diagnosis of status epilepticus and intra hospital evolutionary data of the patients, have been analyzed. Univariate analysis between the general characteristics of patients and the intra-hospital mortality, was performed in order to identify the risk factors for the intrahospital mortality.
Results: The mean age of the patients was 36.6 years with an M / F sex ratio of 1.4 ; 66 patients (72.5%) had no clinical history of epilepsy, while 25 patients (27.5%) were already known to have epilepsy. The generalized tonic-clonic SE immediately (50.5%) and the focal secondarily generalized convulsive status epilepticus (29.7%) were the most common seizure types. The average duration of an SE episode was 18 hours. status epilepticus were subdivided into status epilepticus symptomatic of acute brain conditions with 61 cases (67%), dominated by central nervous system infections and acute strokes, and status epilepticus of non-acute or sequelae etiologies with 30 cases (33%), dominated by the sequelae of head trauma. Intra-hospital complications were dominated by prolonged post-critical mental confusion, 45 cases (49.4%) and aspiration pneumonia, 30 cases (33%). In-hospital mortality was 12.1% (11 patients). At the end of hospitalization, 49 patients (53.9%) still had moderate to severe disabilities. In univariate analysis, comatose non convulsive status epilepticus (p = 0.003), and altered consciousness on admission (p = 0.026), were the risk factors for in-hospital mortality.
Conclusion: Prognosis of status epilepticus in Burkina Faso remains unfavorable with early mortality in more than one in 10 patients and poor functional outcome in more than half of the patients. Altered consciousness on admission and non-convulsive comatose status epilepticus were risk factors for early mortality. The fight against infectious diseases, the prevention of vascular risk factors, the promotion of helmet wearing in cyclists and motorcyclists, early admission of patients sufferinf of status epilepticus, and adequate and standardized management of status epilepticus, will help reduce the frequency and severity of this disease in our African regions.
Status epilepticus (SE) is the second most common neurological emergency after stroke, with high morbidity and mortality and an often poor functional prognosis in survivors [1, 2, 3].
The short-term mortality reported in the literature is very variable from one study to another, in the order of 3% to 39% [1], due to the heterogeneity of the methods used and the populations studied, in particular the inclusion or not of pediatric cases [4], strongly influenced by the underlying aetiology, the age of the patients, the clinical form of the seizures, the delays in patient admission [5].
In Sub-Saharan Africa (SSA), early mortality appears to be higher, particularly in adult patients, in the order of 21.3% to 44.3% in most cases [6, 7], but a lower in the order of 13.3 to 16.9% is reported in some more recent African studies including pediatric cases [8, 9], probably due to the implementation of standardized treatment protocols, better availability of anti-epileptic drugs (AEDs) and adequate emergency and intensive care services.
Advanced age, initial alteration of consciousness prior to administration of treatment, non-convulsive comatose SEs and acute potentially lethal etiologies, and duration of SE> 1 hour, have been identified as the strongest predictors of short-term mortality [10, 11, 12]. Their prevention or adequate management if possible, could contribute to a significant reduction in SE mortality, in particular in a context of under-equipment of health services.
Burkina Faso, like other SSA countries with limited resources, has a high prevalence and incidence of epilepsy, seizures and etiological factors of epileptic seizures, contrasting with a double diagnosis and treatment gap, exposing them to a high risk of SEs and their morbidity and mortality [7, 9, 13]. It is strong of this observation that we carried out the present hospital, multicenter, cross-sectional, descriptive and analytical study. The objectives were to describe the intra-hospital clinical course and to identify the risk factors for intra-hospital death of patients hospitalized for SE in Ouagadougou, Burkina Faso. This study will help improve the management and the prognosis of patients hospitalized for SE.
This was a prospective, cross-sectional, multi-center hospital, descriptive and analytical study, which took place from January 1, 2015 to December 31, 2019, involving all patients consecutively hospitalized in the university hospitals (UH) of the city of Ouagadougou (Tingandogo, Yalgado Ouédraogo, Bogodogo, Charles De Gaulle Pediatric), for SE during the study period.
Were included in our study, patients of all ages consecutively hospitalized in the different hospitalization units of said HUs (emergency reception, neurology, pediatrics, or intensive care units, or any other services), for diagnosed SE clinically and / or confirmed by an electroencephalogram (EEG), during the study period. Note that consent to participate in the study was obtained in all patients who were aware, consistent and cooperative. For those who had altered consciousness and / or were aphasic and / or inconsistent and / or uncooperative, or for any other medical reasons, we obtained the consent of their respective families. Patients who presented with a seizure that did not meet diagnostic criteria for SE and those who did not give informed consent to participate in the study were not included in our study. The data was collected directly from patients or their families during hospitalization and recorded in their medical files, then transcribed on a data collection sheet.
Confirmation of the positive diagnosis of SE and the etiology of SE was made by a neurologist. The management of SEs at the different sites of our study was based on the recommendations of the 2009 Société de Réanimation de Langue Française (SRLF) consensus conference [14]
Data on the history of the disease, history and physical examination were systematically recorded. Complementary biological and neuroradiological examinations were performed according to the context. In an unknown patient with epilepsy: plasma biological assessment (blood count, C Reactive Protein (CRP), blood ionogram, occasional glycemia, azotemia, serum creatinine, hepatic transaminases) and brain CT scan, were made. In any febrile patient regardless of the context, a brain CT scan and a lumbar puncture with cytological, biochemical and bacteriological study of the cerebral spinal fluid (CSF) were performed. In a known epileptic patient under treatment: search for factors of imbalance in the antiepileptic treatment (discontinuation of treatment, suboptimal dosage, intercurrent events such as diarrhea / vomiting, feverish state, etc.). The test for toxic subtances in the blood or urine has not been carried out in our context due to its expensive cost. Depending on the clinical course of the SE, in the emergency department, the patient was either transferred to the neurology unit (discontinuation of the SE) or to intensive care (refractory SE and/or comatose SE). Patients who were in refractory SE and / or in larvae or subtle SE and / or in comatose SE on admission to the emergency room, were directly hospitalized in the intensive care unit. The patient benefited from clinical and / or biological monitoring depending on the context. EEG was not essential for the diagnosis of SE except in non-convulsive SE cases. The outcome at discharge from hospital was assessed using the Glasgow Outcome Scale (GOS).
The following variables were taken into account in our study: sociodemographic characteristics of the patients; clinical data (history of epilepsy, time to hospital, duration of SE, number of SE episodes, semiology of SE, clinical examination upon admission); biological assessment on admission; characteristics at the critical and / or inter-critical EEG; Brain scan and / or brain MRI results ; etiological diagnosis of SE (acute epileptogenic cerebral diseases / attacks, non-acute or sequelae epileptogenic cerebral lesions, undetermined etiologies) and evolving data of the patients: duration of hospitalization, intra-hospital complications, vital and functional prognosis according to the GOS at the end of hospitalization.
The data collected were analyzed using Epi-info 7.2.1.0 software in its French version. The analysis focused on calculations of numbers, frequencies, averages, and percentages of the data collected. We carried out an univariate analysis using the Chi-square test and Fisher's test, between the general characteristics of the patients (independent variables) and the intra-hospital mortality (dependent variable), in order to identify the risk factors for the intrahospital mortality. The variables whose significance threshold was p was less than 0.05 were retained.
SE has been defined, in a general sense, by continuous epileptic seizures or by the short succession of at least two epileptic seizures without recovery of consciousness intercritically, over a period of at least 30 minutes. The generalized convulsive SE, because of its severity, was defined by continuous seizures beyond 5 minutes or by the succession of at least two epileptic seizures without complete recovery of consciousness in intercritical over a period of at least less than 5 minutes [15, 16].
The classification of SEs in the present study was adapted from that proposed by the consensus conference of the French Language Society of Resuscitation [15]. Alertness on admission was assessed using the Glasgow Coma Scale.
During the study period, we consecutively collected 91 patients hospitalized for SE. The mean age of the patients was 36.6 years +/- 24.5 years (2 days and 86 years). Patients aged 15-45 and 0-14 were the most represented with 34 cases (37.4%) and 29 cases (31.9%), respectively. There was a male predominance, with 67 men (73.6%) and 24 women (26.4%); the sex ratio M / F was 1.4. The majority of patients, or 43 patients (47%) were married. Unemployed patients with 27 cases (29.7%) and retirees with 14 cases (15.4%) were the most frequent socio-professional categories. Patients residing in urban areas with 63 cases (69.2%) were the most represented (Table I)

Among our patients, 66 patients (72.5%) had no clinical history of epilepsy, while 25 patients (27.5%) were known to have epilepsy. Among non-epileptic patients, in 55 patients (83.3%), SE occurred early between 1 and 14 days after the onset of an acute brain disease compared to 11 patients (17.5%) in whom SE occurred later (beyond 14 days). For patients with known epilepsy, the mean duration of epilepsy was 39.7 months +/- 54.1 (2 - 252 months); the average seizure frequency was 2.1 seizures +/- 3.2 (1-7 monthly seizures).
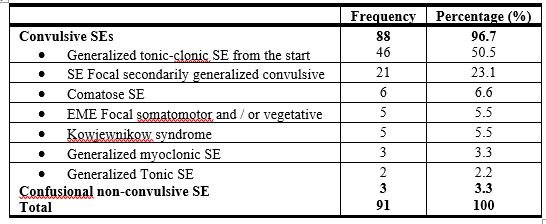
Of all the patients, 88 patients (96.7%) presented with convulsive SE versus three (3) patients (3.3%) who presented with confusional non-convulsive SE. Generalized tonic-clonic SE from the start and focal secondarily generalized convulsive SE were the most represented types of seizures with respectively 46 cases (50.5%) and 27 cases (29, 7%) (Table II).
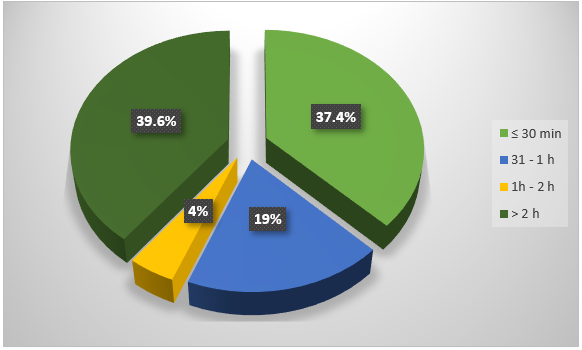
The average duration of an SE episode was 18 hours +/- 31 (5 minutes - 6 days).
SEs lasting> 2 hours and SEs lasting ≤ 30 minutes were the most represented with 36 cases (39.6%) and 34 cases (37.4%) respectively (Figure 1).
The mean number of SE episodes during hospitalization was 3.5 +/- 3.1 (1-20 episodes). EEG was performed only in 22 patients (24.2%), after monitoring of vital functions, in 9 patients (9.9%) percritical and 13 patients (14.3%) postcritical. The tracing was normal in 3 patients (13.6%) post-critical; he found epileptic paroxysms mainly focal or multifocal in 19 patients (86.4%).
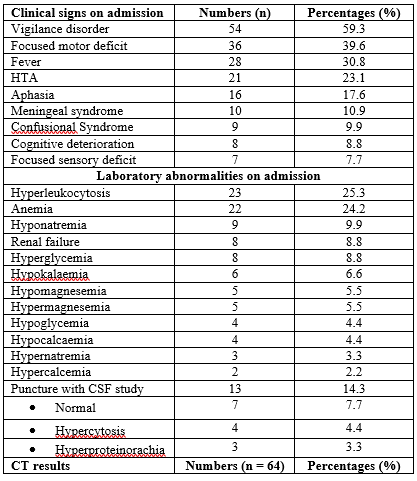
On admission, a focused motor deficit with 36 cases (46.7%), fever in 28 patients (30.8%), hypertension in 21 patients (23.1%), aphasia with 16 cases (20.8%), meningeal syndrome with 10 cases (12.9%), were the main clinical signs; hyperleukocytosis with 23 cases (25.3) and anemia with 22 cases (24.2%), were the main laboratory abnormalities. A lumbar puncture with study of cerebrospinal fluid (CSF) was performed in 10 patients and found hypercytosis and hyperproteinorachia, respectively in 4 patients (4.4%) and 3 patients (3.3%). Brain CT scan was performed in 64 patients (70.3%), sequelae with 33 cases (51.6%), acute stroke with 14 cases (21.9%) and acute meningoencephalitis with 8 cases (12.5%), were the most frequent (Table III).
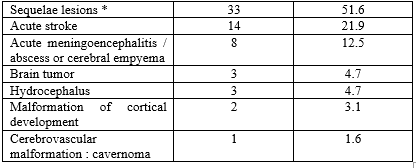
NB : Several lesions were found in the same patient
* Sequelae lesions : cortical atrophy, porencephalic cavity, hypodensity / gliosis sequelae of head trauma, stroke, post anoxo-ischemic encephalopathy or meningoencephalitis
Etiologically, SEs were subdivided into SEs symptomatic of acute brain diseases with 61 cases (67%) and SEs of non-acute or sequelae etiologies with 30 cases (33%) (Table IV).

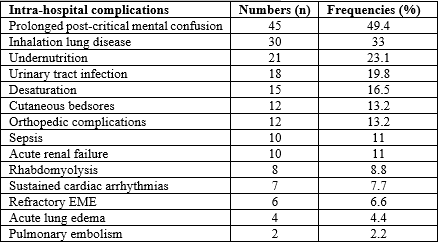
Intra-hospital complications were observed in 58 patients (63.7%) ; prolonged post-critical mental confusion, 45 cases (49.4%), aspiration pneumonia, 30 cases (33%) and malnutrition, 21 cases (23.1%) were the most frequent (Table V)
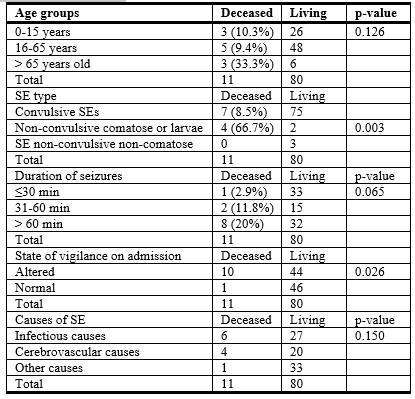
The average length of hospital stay for patients was 10.6 days +/- 16.7 (1 - 60 days). A total of 11 patients died during hospitalization, for an intra hospital mortality rate of 12.1%. According to the age groups, the highest rate of intra-hospital mortality (33.3%) was observed in the oldest patients (> 65 years) (Table VI).
The immediate causes of death were refractory SE in 4 of 11 patients, severe sepsis and multi-organ failure in 3 of 11 patients each, and respiratory distress in 1 of 11 patients.
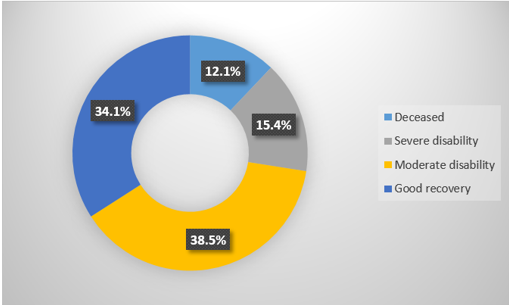
At the end of hospitalization, there was good recovery with normal resumption of activities in 31 patients (34.1%), 35 patients (38.5%) still had a moderate handicap (patient however autonomous in daily life) and 14 patients (15.4%) still had a severe disability (conscious but dependent patient with mental or motor impairment or both) (Figure 2).
In univariate analysis, during the analytical study, comatose or larval EME (p = 0.003), impaired vigilance during admission (p = 0.026), were the risk factors for intra-mortality. hospital identified (Table VI).
Certain important data in this study, in particular the duration of the evolution of the SE, the semiology of the seizures, obtained on the basis of the only questioning of the patients and / or their entourage, could therefore be biased. Indeed, most SEs started before the patients were admitted.
The relatively low proportion of pediatric cases (31.9%) could have biased the data of this study when we know that the high prevalence of epilepsy in children. Conversely, the intra-hospital mortality rate in our study could have been underestimated due to the inclusion of pediatric cases with a better life-threatening prognosis.
Nonetheless, the multicenter nature of our study, extended to all 3 university hospitals in the city of Ouagadougou, allowed us to have fairly exhaustive, representative and reliable data.
In SSA, with fairly comparable methodologies, the intra-hospital or short-term mortality rates reported to date vary from 13.3% to 44.3% [6, 7, 8, 13, 17], contrasting sharply with the low short-term mortality rates of 3.4% reported in the United States of America [5] and 7.6% in Switzerland [18]. However, higher death rates have also been reported in other developed countries [15]. This variation in mortality between studies was linked to whether or not post-anoxic states were taken into account and the differences in initial management.
The causes of death during a SE are, in descending order: its etiology, the patient dying due to the underlying disease and not their SE directly; the complications of intensive care, proportional to the length of stay in intensive care, and therefore also linked to the refractory nature of the SE; prolonged non-controllable refractory SEs [19], including refractory SEs of autoimmune etiology, referred to as NORSE (New Onset Refractory Seizures), or FIRES (Febrile infection-related epilepsy syndrome) [20]. These causes of death, with a few exceptions, were indeed found in our series.
The availability and accessibility of SE drugs, medico-technical infrastructures and equipment (multi-purpose medical resuscitation, neurological intensive care units, etc.) and timely transport of patients, in developed countries, may explain the marked regional disparity in mortality figures.
This heavy mortality of SE in SAA could be explained by the difficulties of the management of SE, linked to the late admissions of patients at the stage of larvae or even refractory SE, the low availability of intensive care units and / or resuscitation, the unavailability of injectable forms of certain AEDs of proven efficacy (such as clonazepam, phosphenytoin, sodium valproate, Levetiracetam), thus causing difficulties in applying SEs support protocols [7]. We must also mention the high proportion of generalized convulsive forms, clinical gravity specific to acute infectious or cerebrovascular aetiologies, the most frequent in this region [7, 9, 17]. In our series, the relatively low early mortality rate of SE is explained by the inclusion of pediatric patients representing 31.9% of cases, the inclusion of a proportion of 17.6% of non convulsive SEs without alteration of consciousness, of better prognosis. In our opinion, the low rate of intra-hospital mortality in our series could also be explained by the efforts to implement protocols for the management of SEs as soon as patients are admitted to the emergency room.
The most robust predictors of intra-hospital or early mortality reported in the literature are: advanced age, most often ≥ 65 years old [10, 11, 12, 21, 22]; acute etiologies of SE, in particular potentially fatal ones such as acute central nervous system infections and acute strokes [10, 11, 21, 23, 24] ; altered consciousness in the initial phase of SE (before administration of treatment), especially non-convulsive SEs with coma [22, 25, 26, 27], maximum duration of seizures (≥ 1 hour) [21, 22]. In our study, only alteration of consciousness in the initial phase of SE and non-convulsive SE with coma, were identified as risk factors for early death, in accordance with the data from the literature. The other predictive factors could not be found, probably due to the inclusion of pediatric cases and certain limitations inherent in our study.
In our series, at the end of hospitalization, 34% of cases had good recovery with normal resumption of activities, close to the results of the study by Cissé et al in Guinea, where a favorable evolution without sequelae was only found in 21.1% of cases [7]. However, in the study by Doumbia et al [13] in Côte d’Ivoire, satisfactory progress with cessation of SE was noted in 63.3% of cases. More than half of our patients had a moderate to severe disability at the end of hospitalization, due to subsequent motor and / or cognitive impairment. However, the responsibility of the SE in the genesis of these sequelae is very difficult to isolate from the neurological deficit associated with the causal neurological injury. Nevertheless, drug-resistant epilepsy and sequelae cognitive-behavioral disorders have been reported after very prolonged SE secondary to bi-hippocampal involvement (edema then cortical atrophy) [28], corroborated by anatomical pathology data in one patient [29].
SE more often affects young patients without a history of epilepsy. The clinical profile is dominated by generalized convulsive forms from the outset or secondarily. Acute central nervous system infections, acute strokes and sequelae of head trauma are the main aetiologies. The prognosis remains unfavorable with early mortality in more than one in 10 patients and poor functional outcome in more than half of the patients. Altered consciousness on admission and non-convulsive comatose SEs were risk factors for early mortality. The fight against infectious diseases, the prevention of vascular risk factors, the promotion of helmet wearing in cyclists and motorcyclists, early admission of patients sufferinf of SE, and adequate and standardized management of SEs, will help reduce the frequency and severity of this disease in our African regions.
Conflict of interest: the authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
