
Case Report | DOI: https://doi.org/10.31579/2641-0419/359
1Children’s Hospital of New Orleans Department of Pediatric Cardiology.
2Children’s Hospital of New Orleans Department of Pediatric Cardiothoracic Surgery.
3Children’s Hospital of New Orleans Department of Pediatric Cardiac ICU and Echocardiography.
4Children’s Hospital of New Orleans Department of Pediatric Interventional Cardiology.
*Corresponding Author: Jesus Jaile IV, Children’s Hospital of New Orleans Department of Pediatric Cardiology.
Citation: Jesus C Jaile IV, Wesam Sourour, Jacquelyn D Brady, Patrick Nelson, Aurelio Reyes, et al, (2024), Short-and-Medium term outcomes of Piccolo Device closure of patent ductus arteriosus in premature infants: A single center review, J. Clinical Cardiology and Cardiovascular Interventions, 7(3); DOI:10.31579/2641-0419/359
Copyright: © 2024, Jesus Jaile IV. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 March 2024 | Accepted: 15 April 2024 | Published: 19 April 2024
Keywords: catheterization; device closure; echocardiography; occlusion; patent ductus arteriosus; Piccolo
Introduction: Obstruction of the left pulmonary artery (LPA) or descending aorta requiring late intervention is a rare complication after transcatheter closure with Piccolo device, but a multidisciplinary approach is often needed to discover and manage the patient when it does occur. We report our center’s experience with the Piccolo device, including 3 cases of late LPA stenosis requiring surgical debridement and pulmonary artery plasty.
Methods: Retrospective chart review of 60 patent ductus arteriosus closures using Amplatzer Piccolo device in premature infants.
Results: 60 cases of device closure in premature infants. Transient LPA stenosis was noted in 8% of patients, LPA stenosis requiring surgical intervention in 5% of patients. LPA velocity of 2.7 m/s at any point following device placement by echocardiogram, and right pulmonary artery (RPA) to LPA ratio of 1.5 to 1 by 2D echo are predictive indicators of need for surgical intervention. Differential lung perfusion scans may also provide important prognostic and follow-up data after intervention.
Conclusion: Transient LPA stenosis is expected after device closure of a patent ductus arteriosus in premature infants. A multidisciplinary approach and vigilant follow-up are required to discover late complications including LPA occlusion and manage the patient when it does occur.
A patent ductus arteriosus (PDA) can be seen in up to 60% of preterm infants and 80% of infants born under 1200 grams. [1] The natural history of the PDA is to close and constrict over time, but in extremely low birth weight and premature infants the ductus fails to close in up to 85% of babies [2]. There has been somewhat of a cyclical thought process on closing the PDA over the last 20 years with a period of non-aggressive management secondary to thoughts that it did not provide any long-term survival improvement in premature infants [3]. Recent data on the hemodynamic effects and well described complications of shunting oxygenated blood away from vital organs through the PDA such as necrotizing enterocolitis (NEC), systemic hypoperfusion, retinopathy of prematurity (ROP), end organ damage, chronic lung disease, and overall mortality have shifted the landscape back towards aggressively closing a hemodynamically significant ductus [4]. Improvements in technology and advancements in the field of echocardiography as well as congenital interventional cardiology specifically the US Food and Drug Administration’s approval of the Amplatzer Piccolo Occluder for transcatheter patent ductus arterioles closure [5] have given neonatologist and cardiologist more suitable options to close a significant ductus. Since the approval in 2019 several centers worldwide have published promising short-term results in ELBW infants, and a comprehensive summary of these results was published by Sathanandam et al in 2023 [6]. This paper aims to summarize our centers experience with the Piccolo device in premature infants including short-and medium-term outcomes, surveillance protocols we’ve implemented due to pitfalls in recognition of new complications and the peri-operative management of device occlusion following device debridement.
Our center has performed 60 PDA closures in premature infants between September 2021 and October 2023, with patient characteristics listed in Table 1 and procedural data listed in Table 2. Short term follow up was defined as immediately post procedure to 1 month and medium term follow up was defined as more than 1 month to 8 months. Our current protocol is a transthoracic echocardiogram (TTE) at the time of device deployment, 1 week following deployment, and then spaced to weekly or monthly depending on progression of LPA stenosis. Metrics used to follow device position and degree of obstruction include spectral doppler, and 2D TTE measurements of the branch pulmonary arteries and aortic arch. Patients who exhibit increasing gradients or evidence of obstruction by 2D echo are referred for lung perfusion study to quantify flow abnormality as part of our centers protocol.
| Patient Characteristics | N=60 (percentage) |
| Gender | 33 female - 27 male |
| Birth weight (kilograms) | 0.814 (0.395-1.730) |
| Gestational age (weeks) | 26.1 (22-32) |
| Mode of Delivery | 29 Vaginal, 31 C-section |
| Prenatal Care | 44 (73%) |
| Prenatal Steroids | 33(55%) |
| PPROM | 32 (53%) |
| Chorioamnionitis | 6 (10%) |
| Surfactant | 60 (100%) |
| APGAR 1 min | 4 (7%) |
| APGAR 5 min | 6 (10%) |
| Type of Feed (formula vs breast) | 34 breast, 26 formula |
| Chronic Lung Disease | 31 (52%) |
| All Cause NEC pre procedure | 9 (15%) |
| Surgical NEC pre prodcedure | 5 (8%) |
| Transfusion prior to procedure | 57 (95%) |
| Length of Hospital stay (days) | 148.7 (53-366) |
| All-cause mortality prior to discharge | 4 (7%) |
Table 1: depicts patient characteristics for the 60 premature infants who underwent device closure in our institution.
| Procedural Data | N=60 |
| Procedural weight (kilograms) average (range) | 1.660 (0.700 - 4.280) |
| Age at procedure (days) average (range) | 49 (14 – 132) |
| Duration of procedure (min) average (range) | 46 (19 – 157) |
| Fluoroscopy time (min) average (range) | 12 (3.2 - 80) |
| PDA minimal diameter (mm) average (range) | 2.4 (1 – 4.3) |
| PDA maximal diameter (mm) average (range) | 3.5 (1.5 - 5.8) |
| PDA length (mm) average (range) | 9.2 (4.3 - 14) |
| Pre procedural growth velocity (grams/day) average (range) | 13.5 (-27, - +58) |
| Post procedural growth velocity (grams/day) average (range) | 18.5 (-14 + 53) |
| Immediate residual ductus: absolute value (percentage) | 3 (5%) |
| LPA stenosis (transient or occlusive): absolute value (percentage) | 8 (13%) |
| LPA stenosis requiring intervention (surgery or angioplasty): absolute value (percentage) | 4 (7%) |
| LPA stenosis requiring surgery: absolute value (percentage) | 3 (5%) |
Table 2 depicts the procedural data for the 60 premature infants who underwent device closure in our institution.
Consistent with previously published data the overall trend in our center is a transient left pulmonary artery (LPA) stenosis, by spectral doppler, and 2D echo, which improves over the course of weeks to months [7]. When comparing all subjects prior to PDA closure the peak pressure gradient through the LPA was 8 mmHg, on average, which rose to a peak gradient of 11.6 mmHg immediately after procedure. At 1-3 month follow up peak gradients in patients that did not end up requiring reintervention began declining to an average of 10 mmHg and returned to baseline by 8 month follow up (Figure 1). When subjects who met criteria for LPA stenosis by echocardiogram velocity or pressure gradients, defined as none (<1>2 m/sec or >16 mmHg), were isolated and compared the overall trend of transient stenosis followed by gradual improvement and return to baseline over 8 months held true (Figure 2a).

Figure 1: depicts the overall trend of LPA stenosis across all subjects. Consistent with previously published data we see a transient increase in LPA velocities immediately after device placement which resolves by 8 weeks post procedure.
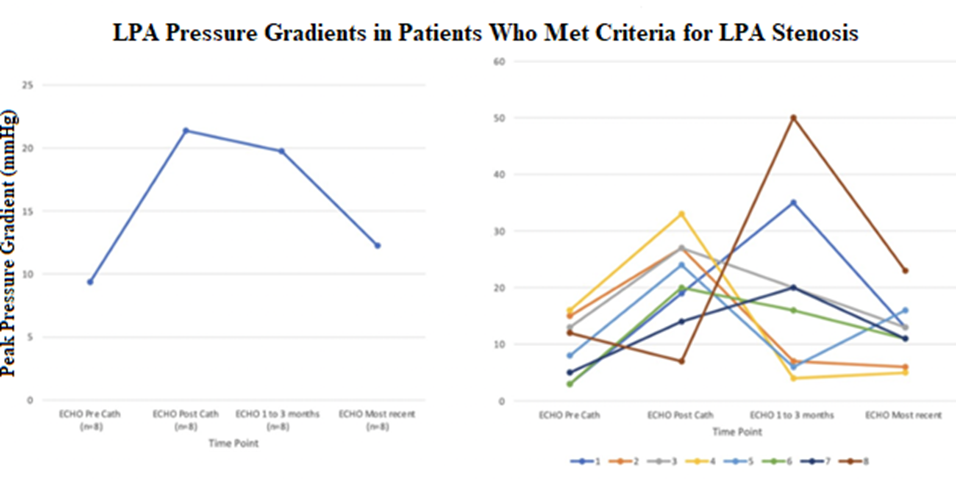
Figure 2a (left) depicts the trend in LPA velocities for the 8 subjects who met echo criteria for LPA stenosis. LPA stenosis defined based on echocardiographic data as none (<1>2 m/sec).
Figure 2b (right) shows the individual trends of LPA velocities across the 8 subjects who met echo criteria for LPA stenosis. Subject 4, 5 and 8 required operative debridement of device and LPA plasty which coincided with their drastic reduction in LPA velocity.
When comparing diameters of the right pulmonary artery (RPA) and LPA patients who did not experience any stenosis showed minimal change in z-score ratio at 8 month follow up, while patients with transient stenosis showed initial increase in RPA to LPA z-score ratio with normalization back to baseline and patients progressing to surgery showed steadily increasing z-score ratio until the time of surgery (Table 4).
| Patients with no LPA Stenosis (n=52) | Patients with Transient LPA Stenosis (n=5) | Patients Requiring Surgery for device debridement (n=3) | |
| RPA to LPA Ratio Pre-procedure | 0.93 to 1 | 0.91 to 1 | 0.95 to 1 |
| RPA to LPA Ratio 4 weeks | 0.99 to 1 | 1.1to 1 | 1.2 to 1 |
| RPA to LPA Ratio 4 months | 0.96 to 1 | 1:05 to 1 | 1.5 to 1 |
| RPA to LPA Ratio 8 months | 0.91 to 1 | 0.96 to 1 | n/a |
| Max RPA to LPA ratio witnessed in groupjesus | 1:1 to 1 | 1.4 to 1 | 1.9 to 1 |
| RPA to LPA Ratio at time of surgery | n/a | n/a | 1.6 to 1 |
Table 4 depicts the ratio of LPA to RPA size over the course of short and medium term follow up. In the group that showed no evidence of stenosis the branch pulmonary arteries exhibited symmetrical growth. In the group that exhibited mild stenosis that improved with time there was transient asymmetrical growth of the RPA which normalized over time. In the group that had severe stenosis requiring intervention the RPA continued to grow asymmetrically until the time of surgery.
When analyzing the patients who progressed to needing operative intervention some trends we noted are patients who achieved a peak pressure gradient over 30 mmHg (2.7 m/s) by spectral doppler at any point all progressed to needing surgical debridement of the device and LPA plasty. (subjects 4, 5, 8 in Figure 2b). In terms of 2D echo parameters RPA to LPA diameter ratio of greater than 1.5 to 1 progressed to requiring surgical debridement of the device. Demographics and comorbidities of each patient are shown in Table 5.
The first two cases showed the Piccolo device to still be intraductal at time of resection with the pulmonary artery disc impinging on the left pulmonary artery from above (Figure 4a & 4b). In case 3 the pulmonary disc was noted to have migrated to the main pulmonary artery (MPA) and LPA junction and the disc was occluding the take-off of the left pulmonary artery with just a pinhole through the center allowing blood flow (Figure 5). In each case the pulmonary disc was debrided, and the LPA was patched to restore laminar blood flow. At 3 months surgical follow up all patients showed normal laminar flow in the LPA as well as normal lung perfusion scan. Prior to the operating room our latest patient had a 88 right to 12 left lung perfusion preference and following the debridement and plasty of the LPA this improved to 40 right to 60 left. (Figure 3a&b) Outside of LPA stenosis other procedural outcomes included, not unexpectedly, transiently diminished left ventricular function, trace pleural effusion, and device embolization and retrieval (Table 3).
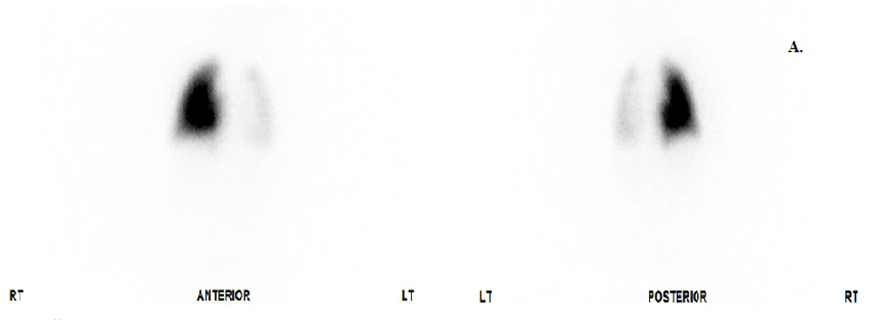
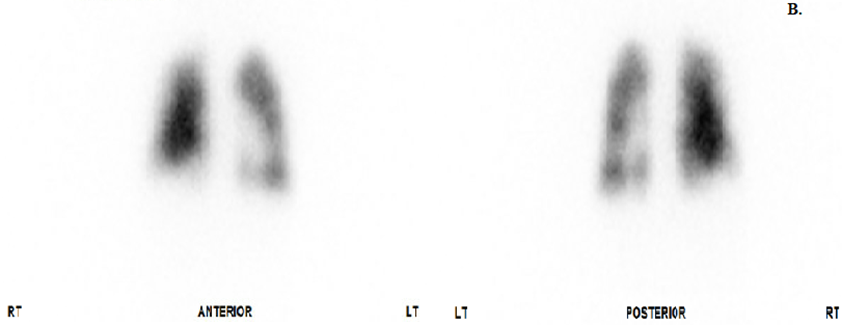
Figure 3a depicts the pulmonary scintigraphy done prior to the surgical debridement and plasty of the LPA. At this time patient had a lung perfusion scan showing 88% perfusion to right lung and 12% to left lung.
Figure 3b depicts the pulmonary scintigraphy done prior to discharge 3 weeks after the surgical debridement and plasty of the LPA. At this time patient had a lung perfusion scan showing 40% perfusion to the right lung and 60% to the left lung.
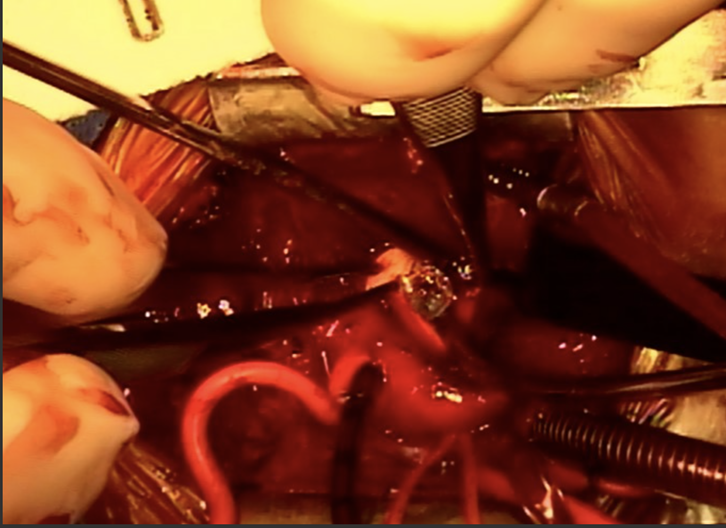
Figure 4a: Patient is oriented with head to the left, feet to the right. The main pulmonary artery has been opened into the LPA, exposing one of the Piccolo discs which was occluding the 2-3mm LPA at approximately 1 o’clock on the disc.

Figure 4b: Patient is oriented with head to the left, feet to the right. The forceps in the bottom left of the image are holding the central pin of the Piccolo, pulling the disc away from and revealing the diminutive LPA orifice where the suction tip is located, at about 2 o’clock on the disc.
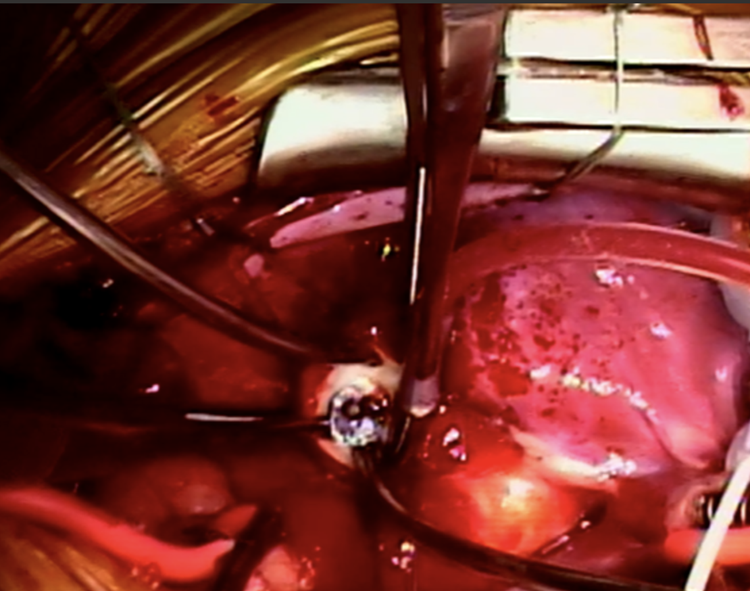
Figure 5: Patient is oriented with head to the left, feet to the right. The main pulmonary artery has been opened into the LPA, exposing one of the Piccolo discs, with the curved suction tip in the near-occluded lumen of the LPA at 6 o’clock on disc.
| Subject # | Procedure Weight | Device Size | Procedure Age (day) | PDA Max Diameter (mm) | PDA Length (mm) | Outcome |
| 1 | 1.11 kg | 4-4 | 31 | 3.9 | 10.9 | Transient LPA Stenosis |
| 2 | 2.47 kg | 4-4 | 65 | 5.6 | 9.6 | Transient LPA Stenosis |
| 3 | 1.44 kg | 5-4 | 52 | 1.5 | 11 | Transient LPA Stenosis |
| 4 | 1.26 kg | 3-2 | 56 | 2.0 | 5.5 | Transient LPA Stenosis |
| 5 | 1.26 kg | 5-4 | 28 | 4.6 | 12.7 | Transient LPA Stenosis |
| 6 | 1.16 kg | 5-4 | 30 | 4.4 | 10 | LPA Stenosis Requiring Surgery |
| 7 | 3.38 kg | 5-4 | 25 | 4.3 | 12.2 | LPA Stenosis Requiring Surgery |
| 8 | 1.47 kg | 4-2 | 54 | 4.3 | 8 | Device Embolization |
| 9 | 2.35 kg | 4-2 | 73 | 3.0 | 10 | Trace Effusion |
| 10 | 1.32 kg | 5-4 | 20 | 3.6 | 12.1 | LPA Stenosis Requiring Surgery |
Table 3: depicts individual procedural data as well as any major or minor complications of the procedure. Diminished left ventricular function improved in a matter of days, trace effusion was not hemodynamically significant and improved over days, and device embolization was retrieved and replaced within the same case without complication.
Data previously published from our center reported the first two known cases of LPA stenosis requiring surgical intervention to debride the device and perform reconstruction of the LPA [6]. Unlike the first two cases in the third case the obstruction to the LPA was by mechanical obstruction of the os by the pulmonary disc of the device, not by compression from above. This type of obstruction most fits the anecdotal reports of the ductus shortening overtime, and with the Piccolo device designed to remain completely intraductal the natural shortening of a ductus could lead to the disc of larger device becoming extra ductal and cause mechanical obstruction of the LPA [7]
Limited data on short- and medium-term outcomes following Piccolo device closure of a PDA in premature infants follow the same trend as data from our institution with some transient LPA or descending aorta stenosis that improves over time, although no one else has published on progression to operative management of LPA obstruction. More data is needed on surveillance and predicting which pulmonary arteries may need intervention prior to resorting to surgical debridement. Each patient underwent cardiac catheterization prior to their operation with attempts made to potentially balloon or stent the LPA without removing the device. In 2 of the cases the os was occluded to the point a wire would not pass. In the third patient, due to the size of the LPA the only option would have been a coronary stent which would have destined the patient for an operation further down the road. A study by Chien et al revealed that the ratio of the device waist after deployment to the nominal waist (<0>
Our institution relies heavily on transthoracic echo measurements and dopplers to trend degree of LPA stenosis, but this does not come without its own challenges. Relying solely on spectral dopplers for assessment of flow can lead to variations between sonographers, angles of insonation, and patient temperament causing variation in flow and doppler measurements delaying recognition of an evolving process. As flow decreases into an obstructed left pulmonary artery there is compensatory increase of flow into the right pulmonary artery which leads to asymmetrical growth of the branch pulmonary arteries. For this reason, we find it important to not only trend spectral dopplers, but also 2D measurements and z scores, as that could be the earliest sign of evolving obstruction. Limitations to this is the scarcity of information surrounding trends in lung perfusion in the setting of evolving obstruction, but is a resource we have started using hope to set guidelines for and correlate to our other metrics in the future.
Since gaining FDA approval the Amplatzer Piccolo device has been used in centers worldwide for closure of PDA in premature infants. Short- and medium-term outcomes show an overall trend of transient LPA or descending aorta stenosis that improves over time in the vast majority of patients. Multiple centers have now reported LPA stenosis requiring intervention to remove the device, and more information and multicenter collaboration is needed on how to accurately predict which patients are at risk of this complication. We recommend using traditional echocardiographic surveillance and using metrics such as 2D measurements and spectral doppler to track evolution. Clinicians should have low threshold to increase frequency of the studies as well nontraditional methods such as nuclear perfusion scans when there is evidence of increasing stenosis.
Patent Ductus Arteriosus: PDA
Left Pulmonary Artery: LPA
Right Pulmonary Artery: RPA
Transthoracic Echo: TTE
Necrotizing Enterocolitis: NEC
The authors have no disclosures about funding, financial or non-financial interest. Retrospective chart review was conducted
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
