
Research Article | DOI: https://doi.org/10.31579/2641-0419/402
Division of Cardiology, University of Arkansas for Medical Sciences, Little Rock, AR.
*Corresponding Author: Iad Alhallak, MD MPH, Department of Cardiology, University of Arkansas for Medical Sciences 4110 Outpatient Circle Outpatient Center, Suite 2H, Little Rock, AR 72205.
Citation: Iad Alhallak, Hakan Paydak, Jawahar L. Mehta, (2024), SGLT2 Inhibitors: Risks and Benefits, J Clinical Cardiology and Cardiovascular Interventions, 7(10); DOI: 10.31579/2641-0419/402
Copyright: © 2024, Iad Alhallak. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 August 2024 | Accepted: 03 September 2024 | Published: 17 September 2024
Keywords: sodium-glucose transporter 2 inhibitors; adverse drug events; canagliflozin
Background: Inconsistent meta-analysis results and the increased risk of co-morbid conditions in type two diabetes make it challenging to distinguish if adverse effects of Fournier’s Gangrene, acute kidney injury, ketoacidosis, genitourinary fungal infections, amputations, and bone fractures are attributed to SGLT2 inhibitors.
Methods: This is a retrospective cohort study that calculates the relative risk and hazard ratio using the Food and Drug Administration Adverse Event Reporting System to compare the users of metformin and the SGLT2 inhibitors for adverse events. The Medical Expenditure Panel Survey database was used to generate total users of dapagliflozin, empagliflozin, canagliflozin, and metformin from the years 2014-2021.
Results: We observed an average increased risk of Fournier’s Gangrene by 156-fold, ketoacidosis by 67-fold, genitourinary fungal infections by 185-fold, amputations by 277-fold, and bone fractures by 15-fold compared to individuals taking metformin. Canagliflozin had the highest increased risk in all categories except for Fournier’s Gangrene, and empagliflozin did not have an increased relative risk of acute kidney injury.
Conclusion: We measured an increase in complications of patients on SGLT2 inhibitors, especially canagliflozin, compared to patients on metformin. We as health providers should re-evaluate our patients with increased risks of these complications and reassess if the cardiovascular benefits outweigh the possible dangerous side effects
When the Food and Drug Administration (FDA) approved the sodium-glucose transport protein 2 (SGLT2) inhibitors for patients with type 2 diabetes, this gave health care providers another oral anti-diabetic medication class that effectively lowers hemoglobin A1C levels by more than 0.5 percent (1-2). In addition to the SGLT2 inhibitor’s glucose lowering effects, recent trials have demonstrated the medication’s protective effects on the cardiovascular system through the reduction of cardiovascular-related mortality and heart failure exacerbations (3-5). This prompted the American Heart Association, the American College of Cardiology, and the Heart Failure Society of America to add SGLT2 inhibitors to the guideline-directed medical therapy for heart failure with reduced ejection fraction in 2022 (6). SGLT2 inhibitors have also been shown to have a renal protective effect, as it reduces the decline of the glomerular filtration rate (3,7-8) and reduces the onset of microalbuminuria (3,5,7,9). With positive effects on glucose metabolism and the cardiorenal system, SGLT-2 inhibitors still have potentially dangerous side effects.
The FDA has placed boxed warnings for the side effects of amputation, bone fracture, acute kidney injury (AKI), ketoacidosis, genital fungal infection, urinary tract infections (UTI), and necrotizing fasciitis of the perineum, known as Fournier’s gangrene (FG) (10). Of all the adverse events, FG is the deadliest with a mortality rate of 20% and 72% in individuals with diabetes (11-12); several case reviews have implicated that FG is associated with the use of SGLT2 inhibitors (13-16). In contrast, meta-analyses have revealed that SGLT2 inhibitors decrease the incidence of AKIs (17-20). Further, most meta-analyses indicated that SGLT2 inhibitors cause a two-fold increased risk of ketoacidosis (17, 21-24), and similarly, a meta-analysis measured an increase in genital fungal infections with SGLT2 inhibitor usage (25). For the side effect of UTIs, many meta-analyses showed no difference in the incidence of individuals taking SGLT2 inhibitors (17,26-28), and likewise, meta-analyses showed no increased incidence for bone fractures (21,29-31). For the side effect of amputations, there are meta-analyses that found an increased incidence of amputations with SGLT2 inhibitors, and some studies found no difference (21-22,29-31). SGLT2 inhibitors act in the proximal tubules by increasing glucose excretion in the urine, which can create a favorable environment for infections and this mechanism is similar to how the body reduces blood sugar levels in diabetic ketoacidosis (34). For the adverse events of bone fractures and amputations, there are proposed mechanisms of how SGLT2 inhibitors increase tissue ischemia (36) and increase bone mineral loss by enhancing fibroblast growth factor-23 and parathyroid hormone levels and reducing 1,25-dihydroxyvitamin D levels (35).
Since these side effects are possible complications of type 2 diabetes (37-38), it is challenging to establish relationships among these adverse events and SGLT2 inhibitors. Further, most patients with type 2 diabetes take metformin, and this is why we used the FDA Adverse Event Reporting System (FAERS) database to study the association among SGLT2 inhibitors and the adverse events of FG, AKIs, ketoacidosis, genital fungal infections, UTIs, amputations, and fractures to compare the SGLT2 inhibitor users to patients using metformin to see which of these effects are attributable to SGLT2 inhibitor use.
| Adverse events | Dapagliflozin (2015-2021) | Empagliflozin (2016-2021) | Canagliflozin (2014-2020) | Metformin (2014-2021) |
| FG | 171 | 450 | 207 | 48 |
| AKI | 360 | 439 | 1,806 | 7,923 |
| Ketoacidosis | 2,885 | 4,262 | 3,917 | 1,778 |
| Fungal Urogenital Infections | 110 | 187 | 336 | 41 |
| Amputations | 96 | 170 | 3,620 | 164 |
| Bone Fractures | 103 | 116 | 148 | 299 |
| Total Number of Drug Users | 2,900,893 | 5,993,571 | 3,537,359 | 137,547,148 |
Table 1: Total number of reported adverse events throughout the indicated years, obtained through the FAERS database, and total number of users in the United States throughout the indicated years, obtained through the MEPS database. Abbreviations: Fournier’s gangrene (FG), acute kidney injury (AKI), and Food and Drug Administration Adverse Event Reporting System (FAERS).
| Adverse Reaction | Dapagliflozin (2015-2021) | Empagliflozin (2016-2021) | Canagliflozin (2014-2020) | Average RR | |||
| RR (CI) | NNH | RR(CI) | NNH | RR(CI) | NNH | ||
| FG | 150 (109-206) | 17,078 | 166 (123-224) | 13,400 | 153 (111-211) | 17,201 | 156 |
| AKI | 2 (1.8-2.3) | 15,895 | 1.1(1-1.2) | 144,630 | 8.7(8.2-9.1) | 2,214 | 4 |
| Ketoacidosis | 70 (66-74) | 1,020 | 45 (43-48) | 1,436 | 85 (81-91) | 913 | 67 |
| Fungal Urogenital Infections | 119(82-171) | 26,596 | 150(97-234) | 32,266 | 287(206-399) | 10,565 | 185 |
| Amputations | 25(20-32) | 31,473 | 19(15-24) | 37,197 | 787(669-925) | 978 | 277 |
| Bone Fractures | 16(13-20) | 30,051 | 9(7-11) | 58,346 | 19(16-24) | 25,207 | 15 |
Table 2: Relative risk with a 95% confidence interval of the side effects of Fournier’s gangrene, acute kidney injury, ketoacidosis, genitourinary fungal infection, amputations, and bone fractures, for the medications dapagliflozin, empagliflozin, and canagliflozin using metformin as the control. Abbreviations: Relative Risk (RR), Confidence Interval (CI), Number needed to harm (NNH), Fournier’s gangrene (FG), and acute kidney injury (AKI).
For this retrospective cohort study, we calculated relative risk (RR) and hazard ratio (HR) with 95% confidence interval (CI) using reported adverse events to FAERS. The information that was used for the calculations comes from patients and providers mostly from the United States who submit adverse events of FG, AKI, ketoacidosis, genitourinary fungal infections, amputations, and bone fractures to FAERS. For our total population group, we have 2,900,893 users of dapagliflozin from 2015-2021, 5,993,571 users of empagliflozin from 2016-2021, 3,537,359 users of canagliflozin from 2014-2020, and 137,547,148 users of metformin from 2014-2021 obtained from the Medical Expenditure Panel Survey (MEPS) database. MEPS is a national survey that asks participants about their prescription medications and then is confirmed with their pharmacies. This survey publishes the 200 most reported medications. MEPS publishes the number of users of specific medications, and this was used to estimate the number of individuals taking SGLT2 inhibitors. Based on the years that SGLT2 inhibitors were one of the top 200 most prescribed medications, FAERS was used to gather the frequency of adverse events, including sex and age of the affected individuals.
The FAERS database medication search included dapagliflozin, dapagliflozin propanediol, empagliflozin, canagliflozin, canagliflozin anhydrous, metformin, metformin extended release 500mg, metformin hydrochloride, metformin hydrochloride extended release 500mg, metformin pamoate.
For FG, we combined the FAERS adverse reactions FG and scrotal gangrene. For AKI, we included the FAERS adverse reaction of acute kidney injury. For ketoacidosis, we included the FAERS adverse reactions diabetic ketoacidosis, ketoacidosis, and euglycaemic diabetic ketoacidosis. For fungal urogenital infections, we included the FAERS adverse reactions vulvovaginal mycotic infection, genital infection fungal, balanitis candida, vulvovaginal candidiasis, genital candidiasis, urinary tract candidiasis, urinary tract infection fungal, fungal cystitis, fungal balanitis, urogenital infection fungal, bladder candidiasis, and fungal urethritis. For bone fractures, we included the FAERS adverse reactions hip fracture, femur fracture, lower limb fracture, fracture, ankle fracture, foot fracture, upper limb fracture, humerus fracture, rib fracture, hand fracture, shoulder fracture, spinal compression fracture, radius fracture, fibula fracture, tibia fracture, lumbar vertebral fracture, clavicle fracture, spinal fracture, femoral neck fracture, fractured coccyx, forearm fracture, cervical vertebral fracture, facial bones fracture, scapula fracture, pelvic fracture, ulna fracture, sternal fracture, and skull fractured base. For amputations, we included the FAERS adverse reactions toe amputation, leg amputation, foot amputation, amputation, limb amputation, finger amputation, hand amputation, and arm amputation.
The statistical program R was used to adjust the weight of the reported users of SGLT2 inhibitors to accurately reflect the total number of users in the United States. The statistical program R was also used to calculate RR and HR from the FAERS and MEPS databases. For the RR and HR calculations, metformin was used as the unexposed/control group. The CI was calculated, and a CI above the number one is considered statistically significant. During the RR and HR analyses, identical years of both SGLT2 inhibitors and metformin was used depending on the MEPS data that were available, for example dapagliflozin adverse events from 2015-2021 was compared to the adverse events of metformin from 2015-2021. Data were extracted and checked at three different time periods, and the data were compared between the three periods for any input errors. Data for age and sex of the individuals have been extracted from the FAERS website and graphed as a percentage. The analyses were performed using RStudio (Boston, MA, USA), and the figures were made using BioRender (Toronto, CA) and Prism 9 (Irvine, CA).
As shown in Figure 1, we observed an average 156-fold increase in FG with SGLT2 inhibitors compared to individuals on metformin, and we measured an inconsistent relative risk of AKI among the medications, with canagliflozin having the highest relative risk of 9 for AKI. Further, we observed an average 67-fold increase in ketoacidosis with the use of SGLT2 inhibitors compared to the individuals on metformin; canagliflozin had the highest relative risk of 85. We observed an average 185-fold increased risk of genitourinary fungal infections, again, with highest relative risk of 287-fold from canagliflozin. We also observed a 787-fold higher risk of amputations for individuals taking canagliflozin compared to individuals taking metformin. Further, we observed an average 15-fold increased risk of bone fractures among the users of these medications.
As shown in Figure 2, there were no consistent trends in side effects affecting a particular age group, except for FG and ketoacidosis, as the majority for these adverse events occurred in subjects under the age of 65. We also observed a consistent pattern for sex, except for individuals that developed AKI and ketoacidosis. We observed a male majority being affected by FG and amputations, and a female majority being affected by bone fractures and genitourinary fungal infections.
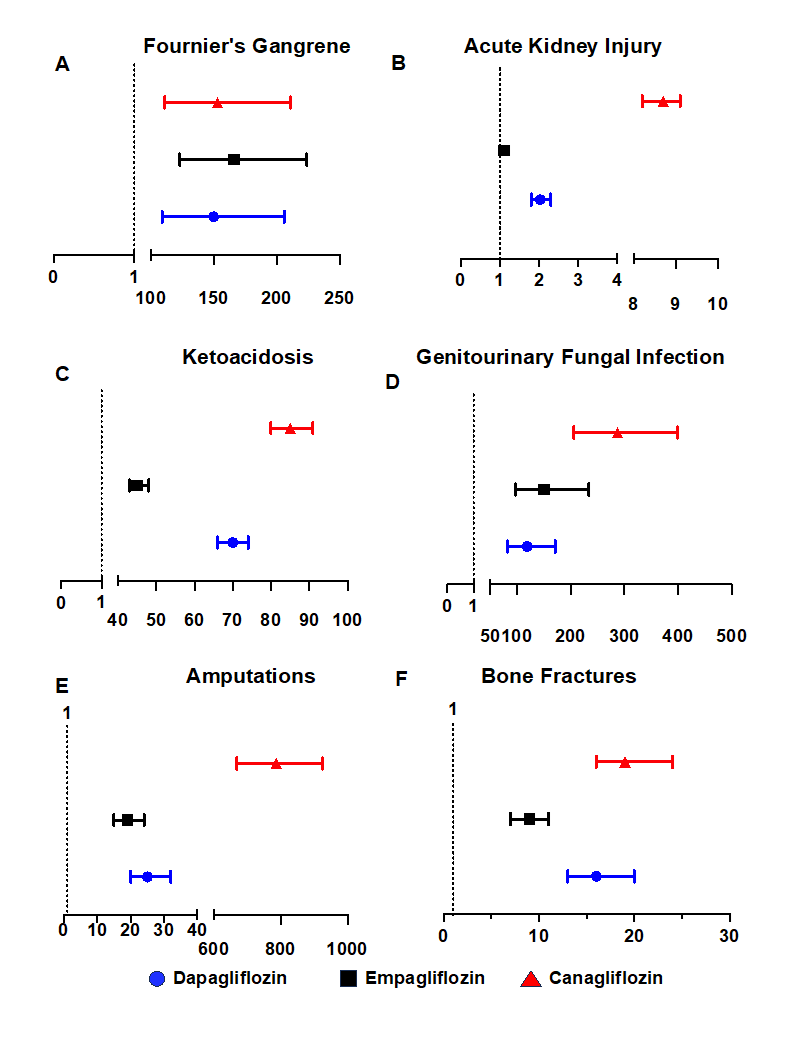
Figure 1: Relative risk with 95% confidence interval of adverse events of Fournier’s gangrene, acute kidney injury, ketoacidosis, genitourinary fungal infection, amputations, and bone fractures, for the medications dapagliflozin, empagliflozin, and canagliflozin using metformin as the control.
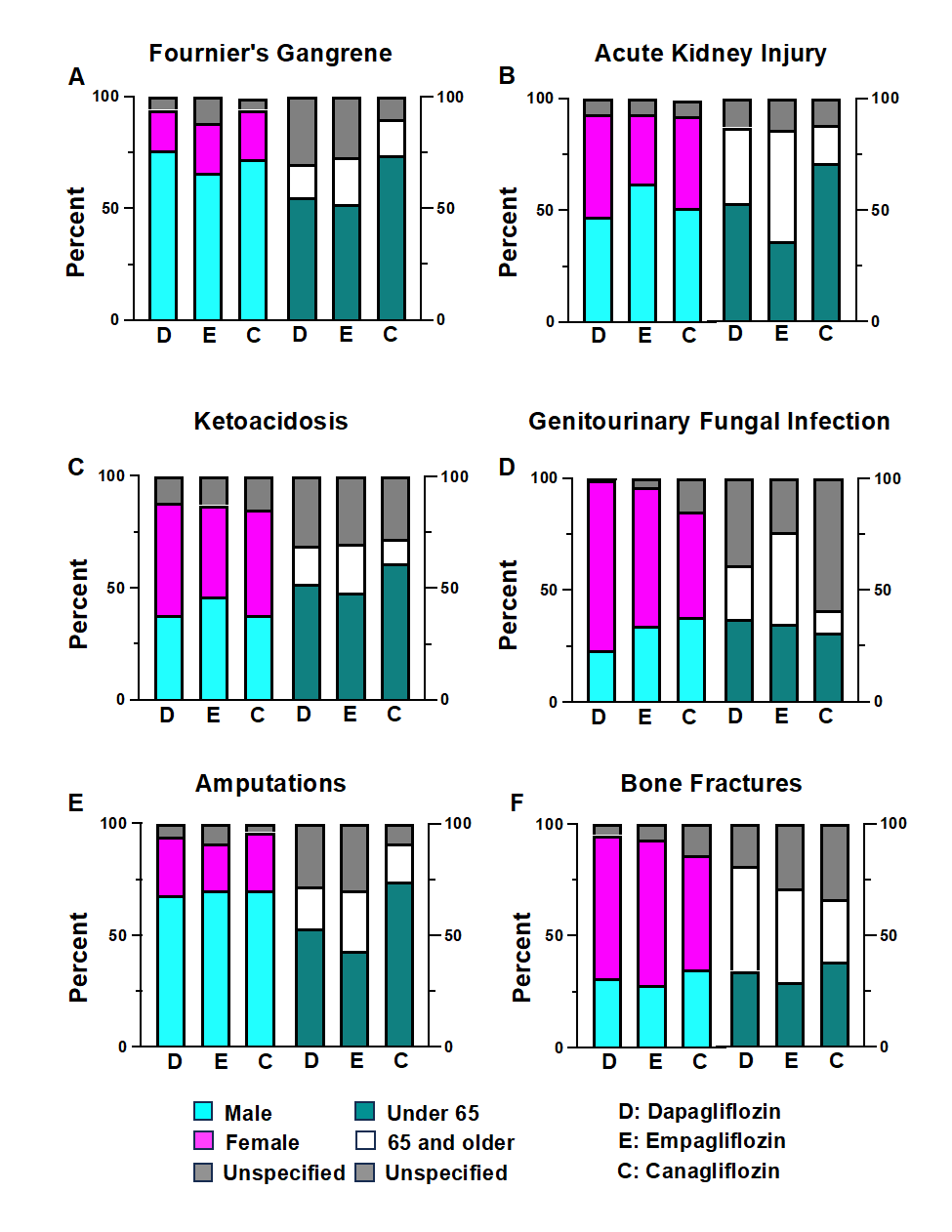
Figure 2: Sex and age of affected individuals for the side effects of Fournier’s gangrene, acute kidney injury, ketoacidosis, genitourinary fungal infection, amputations, and bone fractures.
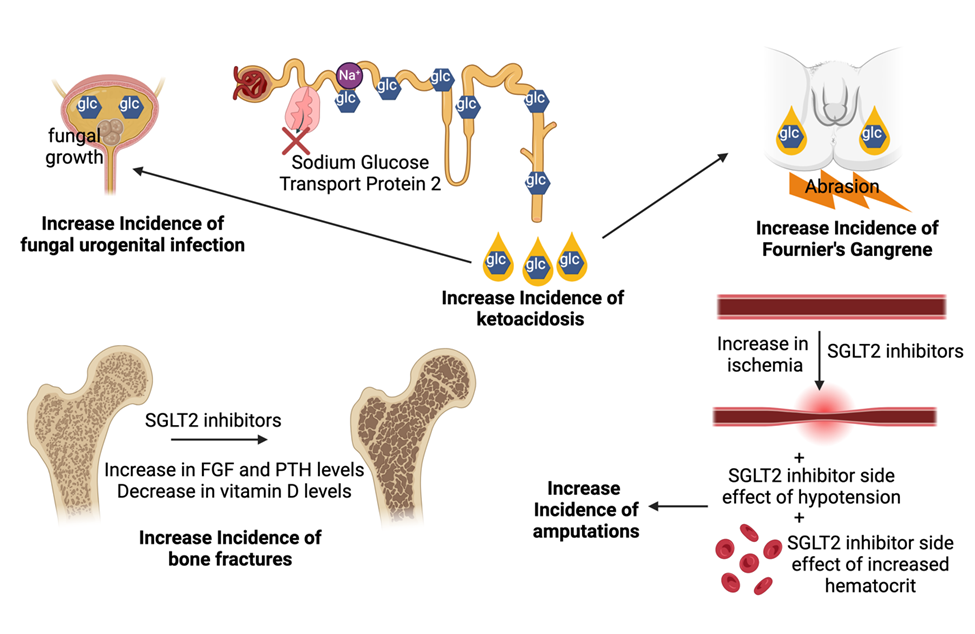
Figure 3: Illustration of the mechanism of action of the potential side effects of the SGLT2-inhibitors. Abbreviations glucose (glc), sodium glucose transport protein 2 (SGLT2), fibroblast growth factor 23 (FGF), parathyroid hormones (PTH).
Compared to users of metformin, we observed increased relative risks for FG, ketoacidosis, genitourinary fungal infections, and amputations among users of dapagliflozin, empagliflozin, and canagliflozin, with canagliflozin having the highest relative risk. We saw variable effects of SGLT2 inhibitors on AKI, with empagliflozin having no increase in relative risk and canagliflozin having the largest relative risk for AKI. Our data with empagliflozin does support the meta-analyses that did not find a difference in AKI (17,19) but does not show any decreased risk of AKI with SGLT2 inhibitors.
Interestingly enough, canagliflozin had the highest relative risks among the adverse events, except for FG. Pharmacokinetic-wise, canagliflozin has the longest half-life in the plasma among the SGLT2 inhibitors (39), which may explain its unfavorable profile. Similarly, canagliflozin has increased urinary glucose excretion and decreased post prandial glucose excretion compared to dapagliflozin (40), which may explain the increased risks of ketoacidosis and fungal urogenital infections. Further, the relative risk for amputations with canagliflozin was significantly higher than metformin and much higher than dapagliflozin and empagliflozin. Canagliflozin has been shown to inhibit the paracrine function of bone marrow derived mesenchymal stem cells, impairing reperfusion of ischemic vessels (41), which is exacerbated by the SGLT2 inhibitor side effect of hypotension and blood hyperviscosity, due to increase in hematocrit, leading to reduced limb perfusion and thus amputation (35).
The sex differences in the affected individuals can be explained by increased prevalence of smoking and peripheral neuropathy in men, which increases risks of amputations (42) and epidemiological prevalence of FG in men (43). The female majority for fractures and urogenital fungal infection can be explained by the overall lower bone mineral density (44), the higher incidence of urogenital fungal infection, and the shorter urethra in women (45). Male patients on SGLT2 inhibitors should be warned of
the side effects of FG and amputations, and female patients should be warned of the adverse event of fungal urogenital infections and bone fractures.
Importantly, the reporting of adverse events to FAERS is vastly underreported with a study indicating that the FAERS only captures 0.01% to 44% of all adverse events (46). Similarly, another study estimates that the FDA only receives about 1-10% of all adverse events (47). This can be attributed to the 5% of providers who do not report these adverse events because of ignorance, procrastination, and the belief that only safe drugs are currently available on the market (48-49). This suggests that the relative risks may be higher and NNH may be lower than what was calculated in this study.
A limitation to this study is that FAERS does not include existing medical conditions, A1C levels, and other medications taken by the patients, which simplifies possible complicated setting of adverse events. This paper did not include all the possible SGLT2 inhibitors. However, this is due to the MEPS database and according to this database and most Americans are using these SGLT2 inhibitors.
With high relative risks of potentially life-threatening conditions like FG and ketoacidosis and serious conditions of amputations, fractures, and fungal urogenital infections from empagliflozin, dapagliflozin, and canagliflozin, should we attempt to restrict certain patients from taking all or certain SGLT2 inhibitors? Based on this data and the positive cardiorenal effects shown by SGLT2 inhibitors (3-9), we believe a personalized risk and benefit analysis should be done with every patient and providers should reconsider SGLT2 inhibitors for patients with increased risks of complications. For instance, immobility drastically increases the risk for the potentially fatal side effect of FG (50).
Due to the limited data on empagliflozin and metformin combination, future research can help distinguish if the adverse events are either solely due to SGLT2 inhibitors, in part due to metformin, or due to the etiology of type 2 diabetes. Future research should also focus on the possible mechanisms for these side-effects to help us understand and prevent these dangerous adverse effects, so we can utilize SGLT2 inhibitors’ cardiorenal protective effects.
Patients on a SGLT2 inhibitor with history of ketoacidosis, immobility, history of frequent genitourinary fungal infections, osteoporosis, and patients with pre-existing conditions like peripheral arterial disease that increases risk of amputation should be re-evaluated for a SGLT2 inhibitor, especially if it is not needed for heart failure with reduced ejection fraction management. However, if the benefits outweigh the risks, empagliflozin has the lowest relative risk of ketoacidosis, amputations, and bone fractures. Since canagliflozin had the highest risk of adverse events, except for FG, among dapagliflozin and empagliflozin, we encourage providers to transition patients to a safer SGLT2 inhibitor.
None
None
None Declared
The data underlying this article are available in [FDA Databases, FDA Adverse Event Reporting System (FAERS)], at https://www.fda.gov/. The datasets were derived from sources in the public domain: [https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
