
Review Article | DOI: https://doi.org/10.31579/2693-4779/114
Endocrinology Division, Department of Medicine, Olive View-UCLA Medical Center, David-Geffen UCLA Medical School, Sylmar, CA, USA
*Corresponding Author: Nasser Mikhail, Endocrinology Division, Department of Medicine, Olive View-UCLA Medical Center, David-Geffen UCLA Medical School, Sylmar, CA, USA
Citation: Nasser Mikhail (2023) Sglt-2 Inhibitors: A Useful Addition for Treatment of Heart Failure with Mildly Preserved and Preserved Ejection Fraction. Clinical Research and Clinical Trials. 7(1) ; DOI :10.31579/2693-4779/114
Copyright: : © 2023 Nasser Mikhail, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 October 2022 | Accepted: 21 November 2022 | Published: 20 January 2023
Keywords: SGLT2 inhibitors; heart failure; mortality; ejection fraction; safety
Background: The use of sodium-glucose cotransporters type 2 (SGLT2) inhibitors is associated with reduction in cardiorenal outcomes in patients with heart failure and reduced left ventricular ejection fraction (HFrEF).
Objective: To clarify the therapeutic role of SGLT2 inhibitors in patients with heart failure and mildly preserved ejection fraction (HFmpEF) and heart failure with preserved ejection fraction (HFpEF).
Methods: Pubmed search until October 13, 2022. Search terms included: heart failure, SGLT2 inhibitors, hospitalization, mortality, safety. Randomized clinical trials and guidelines of major societies were reviewed.
Results: 2 well-designed trials, the EMPEROR-Preserved and DELIVER trials, have shown that use of SGLT2 inhibitors was associated with decrease cardiac events in patients with HFmpEF and HFpEF. In the EMPEROR-Preserved, empagliflozin 10 mg/d decreased a composite primary outcome of cardiovascular (CV) death or hospitalization for heart failure (HHF) compared with placebo, hazard ratio (HR) 0.79 (95% CI, 0.69-0.90, P<0.001). In the DELIVER Trial, dapagliflozin 10 mg/d decreased the primary outcome of CV death or worsening HF, HR 0.82 (95% CI 0.73-0.92, P<0.001). The effects of empagliflozin and dapagliflozin on the primary outcome were evident and statistically significant versus placebo after 13-18 days post randomization. In both EMPEROR-Preserved and DELIVER trials, no significant effects on CV death were demonstrated. By pooling data from the 2 trials, the effects of empagliflozin and dapagliflozin on CV death was close but did not reach statistical significance, HR 0.88 (95% CI 0.77-1.00, P=0.052). Meanwhile, after pooling 2 dapagliflozin trials to include patients with HFrEF (DAPA-HF trial) and HFmpEF + HFpEF (DELIVER trial), dapagliflozin significantly decreased CV death, HR 0.86 (95% CI, 0.75-0.98, P=0.02) and all-cause mortality, HR 0.90 (95% CI, 0.82-0.99, P=0.03). The CV effects of empagliflozin and dapagliflozin were consistent regardless of age, gender, presence or absence of diabetes or atrial fibrillation. Yet, the effect of empagliflozin on decreasing HHF was attenuated in patients with baseline left ventricular ejection fraction (LVEF) of ≥60% and disappeared at LVEF ≥65%. On the other hand, dapagliflozin effects on cardiac outcomes remained consistent regardless of baseline LVEF. Both empagliflozin and dapagliflozin were generally well tolerated, with rates of drug discontinuation due to adverse effects similar to those with placebo.
Conclusions: SGLT2 inhibitors should be the standard of care in patients with HFmpEF and HF pEF similar to their established indication in patients with HFrEF. Until direct comparison between empagliflozin and dapagliflozin becomes available, dapagliflozin should be the SGLT2 inhibitor of choice, particularly in patients with HFmpEF and HFpEF.
Accumulating evidence have shown that use of SGLT-2 inhibitors was associated with decrease in HHF and CV death in patients with HFrEF (defined as LVEF ≤40%) with and without diabetes [1,2]. Accordingly, current guidelines recommend SGLT2 inhibitors in patients with HFrEF to reduce HHF and CV mortality irrespective of presence of type 2 diabetes (class IA recommendation, i.e., strong recommendation, high-quality evidence) [3]. In patients with HFmpEF (LVEF 41-49%) and HFpEF (LVEF ≥50%), treatment options of are limited [3]. The first study that suggested a role of SGLT2 inhibitors in treatment of HFpEF was the SOLOIST-WHF trial that evaluated sotagliflozin versus placebo in patients with diabetes and recent HF (n=1,222) [4]. In the latter study, sotagliflozin decreased HHF, urgent visits for HF, or CV death by an impressive 52% (HR 0.48, 95% 0.27-0.86) in the subgroup of patients with LVEF ≥50%. This subgroup constituted 21% of the study population) [4]. Unfortunately, the SOLIST-WHF was terminated prematurely after a median follow-up of 9 months due loss of funding [4].
More recently, 2 landmark trials, the EMPEROR-Preserved and DELIVER, were published [5,6]. Both trials were specifically designed to examine the effects of empagliflozin and dapagliflozin, respectively on CV clinical outcomes in patients with HFmpEF and HFpEF [5,6]. The main purpose of this review is to provide a critical appraisal on the therapeutic role of the 2 SGLT2 inhibitors empagliflozin and dapagliflozin in patients with HFmpEF and HFpEF based on the findings of the EMPEROR-Preserved and DELIVER trials.
Overview of the EMPEROR-Preserved and the DELIVER trials
The EMPEROR-Preserved and the DELIVER trials are 2 large multinational randomized trials that examined the effects of empagliflozin and dapagliflozin, respectively on CV events in patients with symptomatic HFpEF [5,6]. Overview and main results of the 2 studies are summarized in table 1. Participants had New York Heart Association (NYHA) class II-IV and an LVEF of >40%, with evidence of structural heart disease (left ventricular hypertrophy or left atrial enlargement) associated with N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels of > 300 pg/ml and > 900 pg/ml in patients with atrial fibrillation. In general, inclusion and exclusion criteria of the 2 trials are similar with 2 differences. First, the DELIVER included patients with improved LVEF, i.e., those who had had a previous LVEF of < 40> 40% at the time of enrollment [6]. Second, the cutoff of estimated glomerular filtration rate (eGFR) required for enrollment was different. Thus, patients were excluded from EMPEROR-preserved and DELIVER trials if their eGFR was < 20>
Main results of EMPEROR-Preserved and the DELIVER trials
In the EMPEROR-Preserved trial, over a median of 26.2 months, a primary outcome event occurred in 13.8% and 17.1% of patients randomized to empagliflozin and placebo, respectively; HR 0.79 (95% 0.69-0.90; P< 0>
Effect on empagliflozin and dapagliflozin on cardiovascular and all-cause mortality
In EMPEROR-Preserved and DELIVER trials, the decreased risk of the second component of primary outcome, CV death, did not reach statistical significance (table 1) [5,6]. Similarly, neither empagliflozin nor dapagliflozin significantly decreased all-cause mortality (table 1) [5,6]. After pooling the results of both trials (n=12,251), the effect of empagliflozin and dapagliflozin on all-cause mortality remained non-significant, HR 0.97 (95% CI, 0.88-1.06), and reduction in CV death was close to statistically significant, HR 0.88 (95% 0.77-1.00; P =0.052) [9]. Meanwhile, in a meta-analysis of the 2 trials of dapagliflozin including patients (n=11,007) with HFrEF (DAPA-HF trial) and HFmpEF + HFrEF (DELIVER trial), dapagliflozin significantly decreased CV mortality (HR 0.86, 95% CI 0.75-0.98, P=0.02) as well as all-cause mortality (HR 0.90, 95% CI 0.82-0.99), P=0.03) [10]. Taken together, the above observations suggest that dapagliflozin, but not empagliflozin, may decrease CV death and all-cause mortality in patients with HF across the whole spectrum of EF i.e HFrEF, HFmpEF and HFpEF.
Subgroup analysis
The CV effects of empagliflozin and dapagliflozin on cardiac outcomes did not vary in subgroups classified by age, gender, body mass index, presence or absence of diabetes or atrial fibrillation, degree of frailty, or background use of CV medications [5,6,11-16]. However, a remarkable difference between empagliflozin and dapagliflozin emerged in terms of baseline LVEF. Thus, in case of dapagliflozin, its effects on CV outcomes did not differ across different values of LVEF ranging from ≤30% up to ≥ 60% [17]. However, in case of empagliflozin, the risk reduction in CV death and HHF was attenuated with LVEF ≥60% and is totally lost with LVEF≥65% [5, 18].
Patients with improved LVEF
Improved LVEF refers to those patients with a previous LVEF < 40> LVEF > 40% [3]. Patients with improved EF deserves particular attention due to the following causes. First, despite their growing prevalence, they are usually excluded from trials of HFpEF [19]. Second, even when LVEF return to normal range, these subjects may have worse clinical outcomes than patients with no history of HF [19]. Third, preliminary data suggest that withdrawal of pharmacological HF drugs was associated with relapse in 36% of patients within 6 months of withdrawal [20]. Accordingly, current guidelines recommend that patients with improved EF should continue HF treatment [3]. Patients with improved LVEF were excluded from the EMPEROR-Preserved trial but were allowed to participate in DELIVER trial forming 18.3% of the study population [6,21]. Importantly, results from the DELIVER trial showed that the CV benefit of dapagliflozin was consistent in the subgroup of patients with improved EF [6].
Effects on symptoms of heart failure
Dapagliflozin and empagliflozin improved health-related quality of life symptoms of HF as evaluated by the Kansas City Cardiomyopathy Questionnaire (KCCQ) scored from 0 to 100, with higher scores indicating fewer symptoms and physical limitation. The amelioration in the KCCQ score was modest (mean improvement < 5>
Effects of empagliflozin on renal function
Effect of empagliflozin on renal function was among the prespecified secondary outcomes of the EMPEROR-Preserved trial but was not reported in the DELIVER trial [5,6]. The EMPEROR-preserved showed that the rate of decline in the eGFR was slower in the empagliflozin group than in the placebo group (-1.25 versus -2.62 ml/min/1.73 m2 per year; P<0>300 mg/g, by 19% (HR 0.81; 95% CI 0.70-0.94; P=0.005) [23]. The latter effect was consistent in patients with baseline LVEF ≤40% and >40%, with eGFR ≤ 60 and > 60 ml/min/1.72 m2, and those with and without diabetes [23].
Safety of empagliflozin and dapagliflozin
Both empagliflozin and dapagliflozin were well tolerated. Proportions of patients with serious adverse effects and those who discontinued treatment due to adverse effects were similar to those randomized to placebo (table 1) [5,6]. In EMPEREOR-Preserved, some adverse effects were reported more commonly with empagliflozin compared with placebo including hypotension (10.4% vs 8.6%), urinary tract infections (UTI) (9.9% vs 8.1%), and genital infections (2.2% vs 0.7%) [5]. These adverse effects were not mentioned in DELIVER trial, except for “serious” UTI, which occurred equally in 1% of dapagliflozin and placebo groups [6]. It was reassuring that frequency of acute renal injury and hypoglycemia was not increased with empagliflozin or dapagliflozin [5,6].
Differences between empagliflozin and dapagliflozin
In terms of treatment of HF, dapagliflozin seems to be superior
to empagliflozin in 3 aspects. First, as mentioned above, when data from DELIVER trial and DAPA-HF trial were pooled to encompass the whole range of LVEF, dapagliflozin was associated with significant 14% reduction in CV death and 10% in all-cause death [10]. On the contrary, no mortality benefit was shown with empagliflozin [5]. Second, the cardiac benefits of dapagliflozin extends to patients with LVEF >60%, whereas in case of empagliflozin, this benefit was attenuated with LVEF >60%, and is totally lost with LVEF > 65% [5,18]. Third, in terms of safety, hypotension, UTI, and genital infections were reported more frequently with empagliflozin compared with placebo, whereas these adverse effects were not mentioned with dapagliflozin. The reasons for this discrepancy between empagliflozin and dapagliflozin are unclear but might be related to differences in patients’ characteristics and presence of some dissimilarities in drug properties. Therefore, until head-to-head trials for direct comparison of empagliflozin and dapagliflozin become available, dapagliflozin should be the agent of choice in patients with HF in general, and those with HFpEF in particular.
Although the EMPEROR-Preserved and DELIVER trials are well-designed, they suffer from several limitations [5,6]. First, owing to the multiple exclusion criteria, included patients are relatively healthier than patients in real-life. For instance, patients with eGFR <20>
Empagliflozin-Preserved and DELIVER trials provide strong evidence that the use of SGLT2 inhibitors in patients with HFmpEF and HFpEF may be associated with significant reduction in HHF [5,6]. These 2 categories of HF are of utmost need for new medications that convincingly reduce CV morbidity and mortality. Most recent guidelines published before the release of DELIVER Trial recommend SGLT2 inhibitors as class 2aB recommendation, i.e moderate-strength recommendation, moderate quality evidence, in patients with HFmpEF and HFpEF [3]. After release of results of the DELIVER Trial, it is likely that this recommendation will be upgraded to class 1A, similar to that in HFrEF. While neither empagliflozin nor dapagliflozin individually demonstrated decreased CV death and all-cause mortality in patients with HFmpEF and HFpEF over a median follow-up of up to 2.3 years, longer follow-up (e.g. 5 years) is needed to clarify the effects of SGLT2 inhibitors on these 2 outcomes. Nevertheless, pooling data of the 2 dapagliflozin trials, DAPA-HF and DELIVER, suggest that dapagliflozin may be associated with significant 14% reduction in CV death and 10% in all-cause death [10]. In addition, contrary to empagliflozin, dapagliflozin cardiac benefits persist at LVEF > 60%. Moreover, safety profile might be more favorable with dapagliflozin (table 1) [5,6]. Therefore, until head-to-head trials become available, dapagliflozin may be the SGLT2 inhibitor of choice for use in patients with HF. Advantages and limitations of SGLT2 inhibitors for treatment of HFmpEF and HFpEF are summarized in table 2.
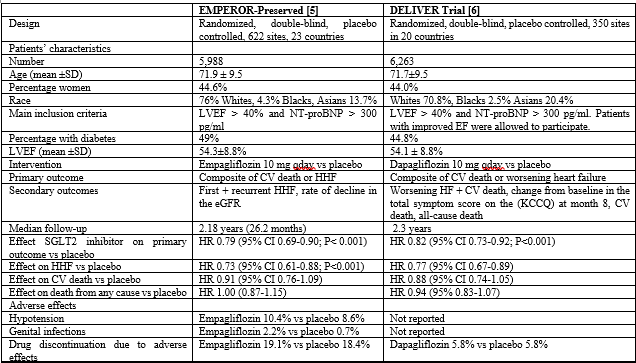
Table 1: Trials of empagliflozin and dapagliflozin on heart failure with preserved ejection fraction
NT-proBNP: N-terminal pro-B type natriuretic peptide, LVEF: left ventricular ejection fraction, CV: cardiovascular, HHF, hospitalization for heart failure, eGFR: estimated glomerular filtration rate, KCCQ: Kansas City Cardiomyopathy Questionnaire, SGLT2: sodium-glucose cotransporter 2, HR: hazard ratio
CV: cardiovascular, HHF: hospitalization for heart failure, UACR; urine albumin-creatinine ratio, LVEF: left ventricular ejection fraction, CKD: chronic kidney disease, eGFR: estimated glomerular filtration rate.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
