
Case Report | DOI: https://doi.org/10.31579/2690-4861/520
1Department of Neuroscience, Psychology, Drug’s Area and Child’s Health, University of Florence, Florence, Italy.
2Department of Neuroscience, Reproductive Science and Dentistry, Section of Audiology, University of Naples ‘’Federico II’’, Napoli, Italy.
3Department of Neurology, Ospedale San Luca di Vallo della Lucania, ASL Salerno, Salerno, Italy.
4University of Salerno, Faculty of Medicine and Surgery, Salerno, Italy.
5Department of Neuroscience, Reproductive Science and Dentistry, Section of Audiology, University of Naples ‘’Federico II’’, Napoli, Italy.
*Corresponding Author: Vincenzo Marcelli, Department of Neuroscience, Psychology, Drug’s Area and Child’s Health, University of Florence, Florence, Italy.
Citation: Giannoni B., Marcelli V., Volpe G, Marcelli E., Fetoni AR, (2024), Severe isolated bilateral posterior semicircular canal hypofunction inducing perverted head shaking downbeat nystagmus, International Journal of Clinical Case Reports and Reviews, 20(2); DOI:10.31579/2690-4861/520
Copyright: © 2024, Vincenzo Marcelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 August 2024 | Accepted: 29 August 2024 | Published: 29 November 2024
Keywords: perverted head shaking nystagmus; down beating nystagmus; head shaking test; head shaking nystagmus; posterior semicircular canals hypofunction
Downbeat nystagmus evoked by horizontal head shaking is most often a sign of central vestibular pathology. Rarely, however, such a sign may be present in peripheral pathologies that are well recognized clinically and semeiologically.
Isolated hypofunction of the two posterior semicircular canals is also a very rarely described condition, often idiopathic or mainly due to deficiency, traumatic, autoimmune or ototoxic disorders.
A 77-year-old man presented to our observation with a history of severe unsteadiness.
The clinical and instrumental examination showed a downbeat nystagmus elicited by a horizontal head shaking test (perverted) and an impairment of both posterior semicircular canals.
Findings suggesting other peripheral vestibular pathologies responsible for this sign or even a central vestibular lesion were absent. Clinical evaluation and blood testing ruled out the conditions reported as potentially responsible for bilateral posterior canal hypofunction.
The case described should lead us to consider isolated idiopathic hypofunction of both posterior semicircular canals associated only with the nystagmus finding of a head shaking downbeat nystagmus, among the peripheral vestibular pathologies already described in the literature that could be responsible for perverted Head Shaking Down Beat Nystagmus (p-HSDBN). Therefore, when faced with the latter finding in a non-emergent outpatient setting, among the various etiopathogenetic hypotheses, this type of peripheral cause should be carefully excluded before sending patients for more invasive and costly tests that may be useless and may delay healing and recovery.
The aim of our study is to present the unique case of a patient with downbeat nystagmus elicited by a horizontal head shaking test (perverted) due to an impairment of both posterior.
The Head Shaking Test (HST) is a simple bedside method used to highlight vestibular asymmetry induced by both peripheral and central lesions. In fact, in the case of predominance of one vestibular hemi-system over the other, the rapid oscillation of the seated patient's head in the horizontal plane can induce the appearance of nystagmus (Head Shaking Nystagmus - HSN), the direction of which generally indicates the predominant side [1-4]. Rarely, HST performed in the horizontal plane may generate a pure vertical nystagmus or a vertical/torsional nystagmus. This type of response is termed 'perverted' head shaking nystagmus (p-HSN) or 'cross coupled' nystagmus and is most often indicative of central pathology [5-7].
Among the different types of p-HSN, downbeat nystagmus (p-DBHSN) is the most common. It represents an altered response, often seen in stroke [7-11], drug intoxication [12,13], carential [11,14], toxic [15-18], neoplastic [7,19] and paraneoplastic [20,21] and degenerative diseases [7,22-24], due to dysfunction of the neurological structures that normally provide the correct coupling of head movements with the oculomotor response. Lesions of the nodal/ventral uvula are responsible for the inappropriate transmission of the vestibulo-ocular reflex (VOR) response elicited by horizontal HS to the vertical VOR pathways [25].
In the case of p-DBHSN, another possible pathomechanism involves a floccular/parafloccular lesion responsible for the loss of the normal inhibitory action that these structures exert on the central connections of the anterior semicircular canals to the vestibular nuclei (and not those of the posterior canals). The latter mechanism would lead to a relative predominance of the anterior semicircular canal signals over those of the posterior canals [5, 11, 24] and thus to an imbalance of the signal in favor of a tonic slow upward sliding of the eyeball.
On the other hand, p-HSN can occasionally be found as a sign of common peripheral vestibular pathologies such as benign paroxysmal positional vertigo (BPPV) [26], unilateral vestibular loss (UVL) or Menière's disease (MD) [27-29], and in rarer conditions such as vestibular paroxysmia [30]. In these cases, however, the clinical history and the morphological and temporal peculiarities of spontaneous or positional nystagmus can help clarify its origin.
In this report we present the unique case of a patient with p-HSDBN due to an idiopathic impairment of both posterior semicircular canals, in the absence of findings suggesting other peripheral vestibular pathologies responsible for this sign or even a nuanced central vestibular lesion.
A 77-year-old man presented in January 2023 with a two-month history of severe unsteadiness in the absence of oscillopsia. A slight bilateral subjective hearing loss was present before the onset of vestibular dysfunction and unchanged at the onset of vestibular dysfunction.
At the time of first evaluation a thorough general and specialized medical history was taken.
The patient underwent audiometric and impedance testing and a complete neuro-otologic examination including visuo-oculomotor (gaze-evoked nystagmus, saccade and smooth pursuit) and vestibulo-oculomotor (positional and positioning maneuvers with and without visual fixation) and hyperventilation testing. A clinical head impulse test (cHIT), a VOR cancellation test, a clinical infrared suppression head impulse test performed on all planes (IR-cSHIMP) and a horizontal head shaking test (HHST) were also administered. Instrumental vestibular evaluation included a Fitzgerald-Hallpike bithermal binaural caloric test, air conduction oVEMPs and c-VEMPs (Interacoustics, Middelfart, Denmark) to assess utricular and superior and saccular and inferior vestibular nerve function, and a video head impulse test (vHIT) recording (ICS Impulse, GN Otometrics, Taastrup, Denmark) with 20 impulses per canal (amplitude 5°-20°, head velocity 50° to 250°/s, sampling rate 250 Hz, cutoffs 0. 8 and 0.7 for horizontal and vertical canals, respectively) with a v-SHIMP test as well.
The patient also underwent routine blood tests and more specific ones with particular emphasis on folic acid, vitamin B1 and B12, electrolytes and thyroid hormone testing; a screening immunologic blood profile was also performed.
Finally, patient was submitted to a thorough neurological examination and to a cranial MRI with and without contrast targeted to the regions of the posterior fossa and of the cerebellopontine angle.
In the patient's personal history, there was no evidence of exposure to solvents or other toxic substances or recent head trauma. The patient's only general pathology was hypertension.
Blood laboratory tests were normal (especially regarding folic acid, vitamin B1 and B12, electrolytes and thyroid hormones) and there was no hematologic evidence of autoimmunity.
Audiometry and impedance testing revealed a mild bilateral sensorineural hearing loss compatible with presbycusis.
Bedside neuro-otologic examination revealed no spontaneous, positional, or positioning nystagmus. In particular, there was no spontaneous and/or positional downbeat nystagmus. cHIT, and VOR cancellation test were normal, as were bedside oculomotor tests. Performing the IR-cSHIMP test in the horizontal plane provided evidence of the normal horizontal anti-compensatory saccades generated at the end of the rotation to recover the visual target in motion integral with the head, which was briefly lost due to normal VOR gain. The same was the case when testing the vertical VOR with downward motions, thus stimulating the anterior canals. In contrast, rapid upward rotations, then with excitatory stimulus on the posterior canal, failed to show any anti-compensatory response, bilaterally. Horizontal Head shaking test revealed a pure and long-lasting p-DBHSN (video 1) which was associated with a strong subjective increase of postural imbalance.
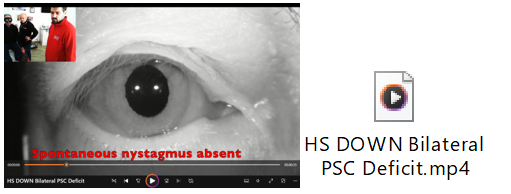
Video 1: The video shows first absence of spontaneous nystagmus and then the down beat nystagmus induced by horizontal head shaking test. Note the patient's need to hold on to the operator and be supported from behind due to the strong unsteadiness.
Video-HIT revealed severe bilateral posterior semicircular canal (PSCC) hypofunction with left and right PSCC VOR gains of 0.3 and 0.23, respectively (normal gain cut-off: 0.7) (Figure 1). However, “clustered” refixation compensatory saccades were present as an indication of the non-acute nature of the disorder and its partial compensation. c-VEMPs and o-VEMPs plotting resulted normal on both sides. Caloric testing was within the normal range.
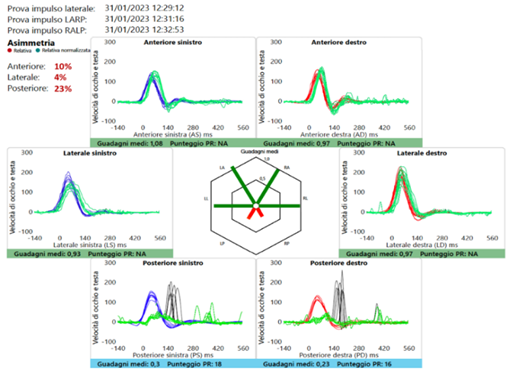
Figure 1: The patient's v-HIT trace shows normal function of the horizontal and anterior canals and a marked reduction in the gain of both PSCCs. Rapid rotation of the head in the plane of the latter with an earth-fixed target results in the appearance of overt saccades, which are already sufficiently clustered at the time of the first evaluation (v-HIT: video Head Impulse Test; PSCCs: Posterior Semicircular Canals).
The neurological examination was unremarkable. MRI of the brain showed only a few and small white matter areas of gliosis. Therefore, our diagnosis was bilateral hypofunction of the posterior semicircular canals of idiopathic nature.
Nevertheless, we started the patient on a course of specific vestibular re-education that lasted about 3 months. At the same time, the patient was recommended piracetam therapy at the dose of 1200 mg twice a day, for about 2 months.
At the 3-month follow-up, the patient reported a marked subjective improvement in postural complaints. The IR-cSHIMP test performed in the posterior canal plane was now positive for the presence of small upward vertical anti-compensatory saccades, and the HST now showed only a small DB nystagmus, still without torsional components.
We report on a clinical case that has in itself the peculiarity of the diagnosis of severe, idiopathic and isolated bilateral posterior canal hypofunction, and thus of rarely encountered disorder of peripheral vestibular function, but above all that of having, as the main revealing bedside vestibular sign, that of a pure DB nystagmus evoked by a HHST (“perverted” nystagmus), which in many cases suggests a disorder of central vestibular structures.
Testing for head-shaking nystagmus is a useful bedside vestibular test to detect asymmetry of velocity storage within the vestibulo-ocular reflex that occurs after peripheral or central vestibular lesions.
The HST is primarily performed in the horizontal plane, as performing the test in the vertical plane is more complex due to the frequent functional limitations of the cervical spine and the resulting lower standardization of results [1]. For generating HSN, asymmetric vestibular input during head rotation and asymmetric charging of the velocity storage system (VSM) is essential [3]. Another possible mechanism to induce HSN could be an asymmetric VSM function [32] and asymmetric peripheral dynamics [3], as might occur when one cupula responds more slowly than the other.
Since the lateral semicircular canal is almost always involved in peripheral vestibular pathology and the input from this canal is functionally predominant, the most observed HSN is a horizontal nystagmus, usually with its rapid phase directed to the predominant side [2,3,33,34]. More rarely, in labyrinthine disorders, there is exclusive or predominant dysfunction of the vertical semicircular canals, which may result in HSN whose rapid phase beats mainly or exclusively downward or upward in the frontal plane, even when the system is stimulated in the horizontal plane. On the other hand, an HSN that beats in a different plane than the one on which the stimulus is applied is called "perverted" or "cross-coupled" nystagmus [5,6] and is much more often an expression of dysfunction of central vestibular structures including stroke [7-10], demyelinating disorders [6], drug toxicity [12,13] and degenerative disorders [22-24]. In most cases, perverted HSN of central origin is purely vertical and with down beat direction (p-DBHSN).
The exact pathomechanism of central p-DBHSN remains uncertain and several hypotheses have been proposed. The first is based on a pathological loss/reduction of the normal inhibitory effect of the flocculus/paraflocculus on the activity of the central connections of the anterior semicircular canals, which otherwise physiologically override the activity of the posterior semicircular canals, at the vestibular nuclei [5,24,35]. Another hypothesis considers the function of the nodulus/ventral uvula, which is known to be important in ensuring that eye rotation occurs in the same plane as head rotation [25,36-37], and whose lesion is responsible for the inappropriate transfer of the activity of the horizontal VOR pathways, evoked by horizontal head shaking, to the vertical VOR pathway [38].
Therefore, when faced with a p-HSDBN, especially in an acute setting and in a first aid context, it is imperative to rule out the presence of a potentially life-threatening central pathology before considering other possible explanations.
As a matter of fact, in our patient's case, although we were not dealing with an acute-onset condition but with a long-standing disorder, among the first causes we were concerned to rule out was that of a potential morphological or functional lesion of a central nature underlying the p-DBHSN. Thorough neurological and neuro-radiological investigation and hematochemical findings seemed to exclude such an origin.
As mentioned above, other possible causes of p-HSDBN may be present in some cases of peripheral pathology. In a large cohort of subjects with a positive HST, p-DBHSN was indeed found in 24.1% of peripheral vestibular disorders, particularly benign paroxysmal positional vertigo (11.8%), acute unilateral vestibular loss (18.2%) and Meniere's disease (8.3%) [39]. Sometimes p-DBHSN could be a sign of pathology between the periphery and the centrality, i.e. vestibular paroxysmia [30].
In these cases, a p-DBHSN can be generated by an absolute or relative prevalence of the activity of the anterior semicircular canals, in the presence of normal and symmetrical functionality in the horizontal plane. Actually, an anterior semicircular canal signal predominance could theoretically be produced by a peripheral posterior semicircular canal hypofunction (i.e., caused by a canal jam altering normal endolymphatic dynamics, neuritis, hydrops) as well as by an abnormal excitation of the anterior canal afferents (ephaptic mechanism). All these above-mentioned peripheral disorders often exclusively or predominantly affect one of the two labyrinths, so any p-DBHSN that may be present is likely to have a torsional component in addition to the vertical. Peripheral vestibular pathologies that are rarely associated with p-DBHSN are usually well identified with an accurate history and careful bedside examination, and p-DBHSN is often almost completely reversible when the pathology is in an interictal phase or is healing. Our patient had no history of positional vertigo nor one suggestive of long-lasting, recurrent, episodic vertigo. He had no auditory symptoms (aural fullness, continuous or pulsatile tinnitus) or vestibular disturbances other than unsteadiness and postural instability. The sign of p-DBHSN was present at the time of the visit despite the onset of symptoms dating back to a few months earlier and bedside neuro-otologic examination revealed no nystagmus findings other than p-DBHSN. The only sign evidenced by the vestibular clinical examination and allowing a direction toward peripheral organ pathology was the bilateral lack of anti-compensatory saccades at IR-cSHIMP performed on the posterior canal plane. This observation confirms the extreme usefulness of this simple test (and whose method and results are reported elsewhere [31], which allows the evaluation of the vertical canals function with only basic instrumentation such as VOS. Instrumental testing with vHIT did indeed confirm a marked reduction in VOR gain with stimulation of PSCCs and normal function of the horizontal and anterior canals. Posterior canal hypofunction was evidenced by the presence of overt saccades that appeared sufficiently clustered to suggest that the lesion was not recent. The v-SHIMP paradigm was also performed, but this test, unlike the IR-cSHIMP, does not have the ability to verify posterior semicircular canal function under these conditions. A normal low-frequency horizontal VOR function was also demonstrated by caloric testing. Among the instrumental studies, cVEMPs were also normal, indicating proper function of the inferior vestibular nerve and supporting a primary and exclusive lesion of the PSCC afferent pathways.
There are few contributions in the literature that report on isolated bilateral PSCC hypofunction and analyze its possible causes and implications. In 2017, Tarnutzer and coll. [40] (reported that in 52 patients with PSC dysfunction, only 12 (23%) had bilateral hypofunction. Only 2 out of 12 patients with bilateral deficits showed impairment of other cochleo-vestibular receptors sufficient to allow diagnostic guidance, as was the case with most of the unilateral deficits. Thus, in the case of bilateral posterior canal hypofunction, as in our patient, the diagnosis of idiopathic nature of the lesion often remains the most common. In fact, our subject's audiometric studies showed only a picture of presbycusis, and his vestibular tests did not show any signs other than PSC hypofunction. Lerchundi and colleagues [29] also reported that among the 41 patients in their cohort with bilateral PSC failure, the most common cause was idiopathic (68%), followed by hypovitaminosis (12%), trauma (9.7%), autoimmune disease (5%), bilateral Meniere's disease, superficial siderosis, hypothyroidism, and ototoxicity, each accounting for less than 2%. All the causes just mentioned had been excluded in our patient.
In 2021 Li et al. [30] report a case series of 23 patients with loss of PSC function, of whom only 14 had isolated loss of function and of these only 2 had bilateral loss. Of these 2, only one of the subjects complained of unsteadiness as in our patient and was diagnosed with autoimmune disease. The other patient had a diagnosis and symptomatology compatible with vestibular paroxysmia. In the patient we studied, both possible causes were excluded by the hematologic and neuroradiologic (no evidence of neurovascular conflict) examinations. Moreover, in the 2 patients studied by Li and colleagues, p-DBHSN was indeed reported, but always in the presence of spontaneous DB nystagmus. Spontaneous DB nystagmus was instead absent in our patient.
To the best of our knowledge, this is the first description of a p-DBHSN associated to bilateral PSCC hypofunction peculiar for at least five different reasons: 1) bilateral PSCC hypofunction was not associated with other nystagmus findings and it was possible to attest its presence only thanks to video-HIT or by performing a simple IR-cSHIMP test, the latter of recent description but of extreme ease; 2) on video-HIT, “clustered” refixation compensatory saccades indicates a good compensation of the VOR reflex and justifies the absence of oscillopsia, while patient’s symptom testifies a weak compensation of vestibulo-spinal reflex; 3) normal c-VEMPs indicated a normal function of inferior vestibular nerves, confirming a primitive lesion of PSCC (and not a relative hyperactivity of the two anterior semicircular canals); and 4) despite the severe bilateral PSCC hypofunction the absence of spontaneous and/or positional downbeat nystagmus in static conditions suggests a good control of the tonic imbalance on the vertical plane but completely lost in dynamic conditions; 5) etiology of bilateral PSCC hypofunction remained unknown.
Although the cause could not be determined, the prompt identification of the pathological signs in the case of our patient allowed us to start a vestibular rehabilitation therapy that was of great subjective help to the patient and led to an objective improvement of the clinical and instrumental situation.
The case presented is, in our opinion, interesting because, first, it brings to light a rare diagnostic probability such as that of isolated and idiopathic bilateral hypofunction of the two posterior semicircular canals and, second, that such pathology was evidenced by the presence of a unique nystagmus sign, p-DBHSN, the latter generally and more frequently indicating a central vestibular pathology.
Except in a first aid setting, where such a sign can only be deepened for an acute central origin, in a second to third level outpatient setting and in the presence of a chronic disturbance a p-DBHSN should also raise the suspicion of the simultaneous and isolated presence of a posterior canal deficiency, even in the absence of autoimmune, toxic, deficiency or neurological pathology.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
