
case report | DOI: https://doi.org/10.31579/2690-4861/685
1 Resident internal medicine, Rijnstate Hospital, depart. Internal medicine, Arnhem, the Netherlands.
2 Neurologist, Rijnstate Hospital, depart. Neurology, Arnhem, the Netherlands.
3 Oncologist/internist; Rijnstate Hospital, depart. Internal medicine, Arnhem the Netherlands.
*Corresponding Author: M.L. Mak, resident internal medicine, Rijnstate Hospital, depart. Internal medicine, Arnhem, the Netherlands.
Citation: M.L. Mak, E. Verstraete, I.M. Werter, (2025), Severe Immune-Related Adverse Event with Myocarditis and Neuromuscular Symptoms with Adjuvant Nivolumab in Esophagus Carcinoma: A Case Report, International Journal of Clinical Case Reports and Reviews, 22(5); DOI:10.31579/2690-4861/685
Copyright: © 2025, M.L. Mak. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2024 | Accepted: 23 January 2025 | Published: 30 January 2025
Keywords: myocarditis; esophageal carcinoma; immunotherapy
Dear reader, ‘I will not harm the patient’ is one of the basic principles of medicine as part of the Hippocratic Oath. Unfortunately, the case below involved an unintended serious side effect due to adjuvant immunotherapy (nivolumab) in the treatment of a patient with esophageal carcinoma.
Case Report
In April 2023, a 70-year-old male presented to the outpatient clinic of gastroenterology with complaints of dysphagia and weight loss. A diagnosis of iT3N1M0 adenocarcinoma of the distal esophagus was established. Prior to a planned curative esophagectomy, chemoradiotherapy was administered according to the regimen used in the CROSS-trial (1). In November 2023, following an R0 resection with residual pathological disease, the patient began adjuvant immunotherapy with nivolumab (2). Fourteen days after starting nivolumab, the patient developed complaints of palpitations and worsening dysphagia. Liver enzyme abnormalities were noted (ALAT 186 U/L, ASAT 263 U/L, LD 508 U/L) as well as thyroid dysfunction (TSH 0.001, FT4 51 pmol/L, FT3 17 pmol/L), with no signs of abnormalities in other endocrine axes. Hepatitis B/C/E serology and EBV/CMV IgM were negative, and abdominal ultrasound revealed no liver abnormalities. A suspicion of immune-related hepatitis, gastritis, and thyroiditis was raised. The patient was admitted to the hospital, and intravenous prednisone (80 mg) and propranolol (40 mg) were initiated. Two days later, liver enzymes showed insufficient improvement (Y-GT 83 U/L, ALAT 451 U/L, ASAT 196 U/L, LD 700 U/L), prompting the initiation of intravenous methylprednisolone (100 mg), which was increased to 200 mg after 2 days due to continued inadequate response. Six days later, the patient developed bradycardia (47 bpm) and required supplemental oxygen. An ECG revealed a complete AV-block with atrial flutter (Figure 1), along with elevated troponin (2729 ng/L) and CK levels (1090 U/L). Although MRI of the heart showed no significant abnormalities, immune-related myocarditis was considered. Mycophenolate mofetil (MMF) twice a day 1000 mg was started, and methylprednisolone was continued. Subsequently, the liver function improved. Due to persistent complete AV-block, a pacemaker was implanted.
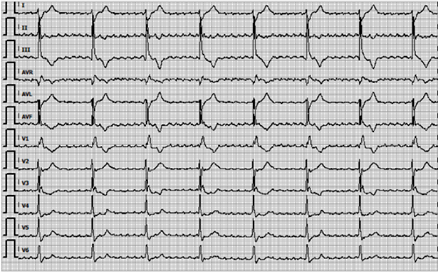
Figure 1: ECG with an atrium flutter and total AV-block provoked by inflammation in myocarditis.
Despite the stabilization of the cardiac condition, the patient remained oxygen-dependent. A CT-scan of the chest excluded pulmonary embolism and immune-related pneumonitis, but revealed dorsobasal atelectasis with pleural effusion, likely attributable to decompensated heart failure due to bradycardia. The patient was started on furosemide (40 mg), which resulted in a reduction of body weight and a decrease in oxygen requirements from 4L to 2L. The patient continued treatment with MMF and prednisone during this period. Eighteen days after the initiation of MMF and six weeks after nivolumab administration, the patient was found unresponsive with a Glasgow Coma Scale (GCS) of 3. A CT scan of the brain revealed no significant findings. Arterial blood gas analysis demonstrated respiratory acidosis, with marked hypercapnia being the most likely explanation for the reduced GCS (pH 7.13, pCO₂ unmeasurable high, pO₂ 24.6 kPa, bicarbonate unmeasurable high). Retrospectively the patient had reported symptoms of diplopia, difficulty speaking and swallowing, hoarseness, and difficulty using his phone several days prior to the acute decline in GCS. Differential diagnoses were immune-related myasthenic syndrome or an inflammatory neuropathy such as Guillain-Barré syndrome (GBS). An EEG showed diffuse slowing with polymorphic delta activity but no epileptiform abnormalities. An EMG revealed no evidence of neuromuscular transmission defects but did show signs of polyneuropathy, without clear demyelinating features. Antibodies against acetylcholine receptors and muscle-specific kinase (MuSK) for diagnosing myasthenia gravis (MG) were negative. Anti-ganglioside GQ1b antibodies, which are associated with the Miller-Fisher syndrome (a variant of GBS), were also negative. Given the clinical suspicion of an immune-mediated neuromuscular complication related to immunotherapy, treatment with intravenous immunoglobulins (IVIG) (0.4 g/kg) was initiated for five days. Initially, the patient showed improvement while on mechanical ventilation, leading to extubation. However, after a few days, respiratory function deteriorated again. The patient clearly expressed a preference not to undergo reintubation. Following thorough counseling of the patient and family, comfort measures were instituted. The patient passed away 38 days after the first dose of adjuvant nivolumab.
| Date | Y-GT (U/L) | ALAT (U/L) | ASAT (U/L) | LD(U/L) | NT proBNP (pmol/l) | Troponine-I (mmol/l) | CK (U/L) |
| 31-10-2023 | 34 | 25 | 21 | 171 | - | - | - |
| 20-11-2023 | - | 186 | 263 | 508 | - | - | - |
| 23-11-2023 | - | 272 | 361 | 631 | - | - | - |
| 15-11-2023 | 40 | 362 | 304 | 701 | - | - | - |
| 27-11-2023 | 46 | 420 | 294 | 746 | - | - | - |
| 1-12-2023 | 83 | 451 | 196 | 700 | 222 | 2729 | - |
| 2-12-2023 | - | 406 | 160 | 599 | 149 | 1407 | 1090 |
| 3-12-2023 | 106 | 373 | 125 | 541 | - | 1122 | - |
| 4-12-2023 | 172 | 444 | 136 | 517 | 138 | 834 | 616 |
| 7-12-2023 | 319 | 435 | 124 | 372 | - | 339 | - |
| 9-12-2023 | 284 | 342 | 74 | 371 | 159 | 201 | - |
| 12-12-2023 | 296 | 268 | - | 584 | - | - | - |
| 14-12-2023 | 285 | 236 | 48 | 333 | - | - | - |
| 18-12-2023 | 242 | 186 | 44 | 336 | - | 138 | - |
| 19-12-2023 | 246 | 187 | 53 | 370 | 236 | 149 | 127 |
| 20-12-2023 | - | - | - | - | 196 | 183 | - |
| 21-12-2023 | 163 | 117 | 42 | 268 | - | - | - |
| 22-12-2023 | 142 | 97 | 32 | 240 | - | 107 | 163 |
| 23-12-2023 | 149 | 98 | 36 | 266 | 83 | 99 | 189 |
| 24-12-2023 | 127 | 80 | 31 | 233 | - | - | - |
Table 1: Course over time of liver enzymes and cardiac markers including troponin during admission. On November 3th 2023, the patient received his first dose of nivolumab.
Neuromuscular Side Effects
Nivolumab, an immune checkpoint inhibitor (CPI, is widely used in oncology in cancers such as melanoma, renal cell carcinoma and esophageal carcinoma. It binds to the programmed cell death protein-1 (PD-1) receptor, a negative regulator of T-cell activity, thereby blocking its interaction with the ligands PD-L1 and PD-L2 on tumor cells. This results in enhanced T-cell activity against tumor cells(3). In addition to the beneficial effects on tumor growth, CPIs are associated with immune-related adverse events (irAEs). Common side effects include skin rashes, endocrine disorders, gastrointestinal issues, pneumonitis, and hepatitis (4, 5). Less commonly, myocarditis and neuromuscular disorders such as myasthenia gravis (MG) can occur, often in combination with one another (6-8).
In the discussed case, the neuromuscular symptoms of the patient were not recognized at first. It is essential to recognize early signs and symptoms such as diplopia, ptosis, dyspnea, dysphagia, and muscle weakness, as well as indications of cardiac involvement. When diagnosing conditions like myositis, myocarditis, and/or MG, it is important to be alert for overlapping presentations, as in the case described here, which could be classified as a myasthenia-myositis-myocarditis overlap syndrome (MMMOS). This condition arises from a systemic immune response involving both the myocardium and neuromuscular junction. Diagnosis can be made using EMG, acetylcholine receptor antibody testing, troponin levels, ECG, and cardiac MRI. Treatment typically involves systemic immunosuppressive therapy with corticosteroids and intravenous immunoglobulin (IVIG) (9). Myocarditis associated with CPI has a poor prognosis, with fatal outcomes occurring in approximately 25% of cases. The prevalence of MG in nivolumab-treated patients has been reported to be 0.12% in a Japanese study, with even a smaller amount presenting with an overlap syndrome. In our case, acetylcholine receptor antibodies were negative, and the patient’s presentation did not fully meet the criteria for MG. In other described cases similar patrons are registered (6, 7, 10). However, considering the clinical course, MG remained highly suspect. A retrospective examination indicated that the patient had experienced symptoms of diplopia, difficulty speaking and swallowing, hoarseness, and difficulty using his phone for several days before the acute decline in GCS. Given the earlier diagnosis of myocarditis, greater vigilance for the development of neuromuscular side effects, would have been prudent in the context of the MMMOS.
Since the first of January in 2024, the Dutch Commission for the Evaluation of Oncological Drugs has withdrawn its initial positive recommendation for adjuvant nivolumab in esophageal cancer, citing limited improvements in disease-free survival and the lack of mature survival data (11). The European Society for Medical Oncology (ESMO) and American Society of Clinical Oncology (ASCO) still recommend adjuvant nivolumab for esophageal cancer both based on CheckMate 577 study (2). Both nivolumab and pembrolizumab have various adjuvant indications; however, long-term survival data are often not convincing yet. More long-term data is needed to better understand the benefit of adjuvant immunotherapy in esophageal carcinoma. It is therefore crucial to carefully weigh the risk of serious complications against the potential uncertain survival benefit.
Dear colleague, the decision to initiate (adjuvant) immunotherapy must be thoroughly considered. Clinicians should be particularly alert of the possibility of MMMOS as a rare but serious complication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
