
Case Report | DOI: https://doi.org/10.31579/2690-4861/644
Intensive Care Unit, Department of Intensive Care Medicine - Ente Ospedaliero Cantonale, Ospedale Regionale Bellinzona e Valli, Bellinzona, Switzerland.
*These authors contributed equally.
*Corresponding Author: Ermes Lupieri and Enrico Patrese, Intensive Care Unit, Department of Intensive Care Medicine - Ente Ospedaliero Cantonale, Ospedale Regionale Bellinzona e Valli, Bellinzona, Switzerland.
Citation: Ermes Lupieri, Enrico Patrese, Alessandro F. Chiesa, Marco Previsdomini, (2025), Severe Hypoxemia and Hemodynamic Instability Following Salt Tablet Broncho-Aspiration: In-Hospital Mimicking of Saltwater Drowning, International Journal of Clinical Case Reports and Reviews, 22(4); DOI:10.31579/2690-4861/644
Copyright: © 2025, Ermes Lupieri and Enrico Patrese. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2024 | Accepted: 13 January 2025 | Published: 24 January 2025
Keywords: postural ventricular tachycardia; antidiuretic hormone secretions
A 70-year-old woman, hospitalized for asymptomatic hyponatremia secondary to SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion), requires emergency intubation due to severe acute respiratory failure and hemodynamic instability following broncho-aspiration of a salt tablet. We hypothesize that a pathophysiological mechanism resembling saltwater drowning may have contributed to the clinical presentation.
Hyponatremia is the most common electrolyte abnormality encountered in clinical practice, and the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), the nonosmotic release of arginine vasopressin, is the most frequent cause. [1] Certain drugs, including antidepressants, can enhance ADH release or effect. [2] Oral sodium chloride tablets are a recognized treatment for hyponatremia in non-edematous patients with mild or absent symptoms [3, 4].
We describea case of a salt tablet broncho-aspiration, resultingin severe acute respiratory failureand shock requiring intubation.
A 70-year-old woman with a history of active smoking and schizoaffective disorder, currently on trazodone and risperidone therapy, presented to the emergency department with a three-day history of progressively worsening dyspnea, exacerbation of a chronic non-productive cough, and mild hypoxemia evidenced by a saturation of 88-89% on room air and a PaO2/FiO2 ratio of 210 mmHg. Two weeks prior to presentation, the patient underwent percutaneous needle biopsy of a 10 cm lump in the left breast, which identified an estrogen receptor-positive infiltrating carcinoma of no special type (NST). She did not report fever, and inflammatory markers were only mildly elevated (C- Reactive-protein at 10 mg/L and Leucocytes at 12,8 x10E9/L). She had no edema, the NT-Pro-BNP level was normal (474 ng/L), and auscultation revealed several added sounds, including rhonchi and wheezes. A chest X-ray (figure 1) showed a predominantly interstitial involvement, consistent with vascular congestion in the small circulation. In this context, the emergency department colleagues administered bronchodilators, for a possible exacerbation of a previously undiagnosed chronic obstructive pulmonary disease, and diuretics. This treatment resulted in an improvement of symptoms. Laboratory tests subsequently revealed hypotonic hyponatremia (Na+ 116 mmol/L, plasma osmolality 242 mmol/Kg, urine sodium 109 mmol/L, urine osmolality 278 mmol/Kg). Given the absence of neurological deficits and the patient’s history, these findings were deemed consistent with the syndrome of inappropriate antidiuretic hormone secretions (SIADH) induced by antidepressant medications. Although the initial differential diagnosis included a potential paraneoplastic origin, this was considered unlikely, as such syndromes are rarely associated with this type of tumor.
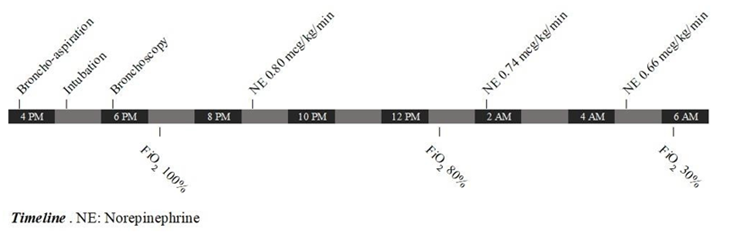
The patient was admitted to our Intensive Care Unit to monitor and correct sodium levels appropriately and for potential non-invasive ventilation (NIV), while awaiting further investigations of the clinical picture. Indeed, within 24 hours of admission, the patient exhibited normal breathing patterns and maintained peripheral oxygen saturation with 2-3 liters/min of supplemental oxygen with nasal cannula. However, following the accidental inhalation of a 1-gram sodium chloride tablet, she experienced immediate respiratory distress and rapid significant desaturation. A chest X-ray showed complete opacity of the left hemithorax, parenchymal atelectasis, and the ipsilateral obliteration of the main bronchus (figure 2). Her condition did not improve with NIV, necessitating urgent intubation.

During post-intubation bronchoscopy, performed approximately two hours after the accidental inhalation, no tablet was found in the left bronchial tree. Instead, we observed a clear, greyish liquid, which we hypothesize to be the dissolved tablet. Concurrently, the patient was hemodynamically unstable, requiring up to 0.8 mcg/kg/min of norepinephrine. The patient exhibited mostly the aspects of a distributive shock, as evidenced by warm extremities and preserved urine output, along with some features of relative hypovolemia. Transpulmonary thermodilution parameters, provided by a PiCCO catheter inserted after intubation, indicated a mildly reduced cardiac index (CI 2.88 L/min/m2). These findings were observed in the context of a preload (GEDI 669 mL/m2) and systemic vascular resistance (SVRI 1807 dyn*s*cm-5*m2) at the lower limits of normality, despite high vasopressor use. Additionally, a cardiac ultrasonography showed a preserved biventricular function.
Following endotracheal intubation and bronchoscopy, the patient required high-inspired oxygen fractions (FiO2) of 80-100% for several hours and hemodynamic instability resolved within 36 hours. Two days later, a contrast-enhanced chest CT scan ruled out pulmonary embolism, showed some residual parenchymal consolidations in the left lung and revealed carcinomatous lymphangitis as the cause of the interstitial involvement. Viral and bacterial cultures were negative.
Once the needs for catecholamines and ventilatory assistance decreased, the patient was successfully extubated. At the time of discharge from the ICU, the patient still required low flow oxygen at 1-2. liters per minute. Additionally, secretion management was complicated by previously unrecognized dysphagia.
We present a case of salt tablet broncho-aspiration with a well-documented timeline, resulting in the sudden onset of severe hypoxemia and hemodynamic instability, in a previously mildly symptomatic patient We believe that simple inhalation of a foreign body does not fully account for the high catecholamine requirements and severe hypoxemia, which persisted well beyond the dissolution of the tablet. Another pathophysiological mechanism may have contributed.
We hypothesize that the hypertonicity of the dissolved salt tablet (NaCl equivalent of about 30 mL of seawater [5]) triggered a rapid influx of fluid from the plasma into the alveoli of the left lung, leading to damage to the surfactant function [6], disruption of the alveolar-capillary membrane, and generation of foam. These combined factors significantly impaired gas exchange, mimicking the pathophysiology observed in saltwater drowning [7] and producing a pronounced shunt effect through the affected lung.
The patient developed warm shock without lactate elevation and maintained urine output, which is inconsistent with hypovolemia or elevated intrathoracic pressure as the sole cause. An echocardiogram performed after intubation showed normal biventricular function. Although inflammatory markers increased 24 hours later, cultures remained negative for bacterial growth, making an infectious cause of the shock unlikely. Instead, a systemic inflammatory response due to the release of mediators in the lung, as described following drowning events, might be the most plausible explanation [8].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
