
Case Report | DOI: https://doi.org/10.31579/jnmir/005
1 General Surgery Division, Hospital de Pediatría Prof. Dr. Juan P. Garrahan. Buenos Aires. Argentina.
2 Plastic and Reconstructive Surgery Division, Hospital de Pediatría Prof. Dr. Juan P. Garrahan. Buenos Aires. Argentina.
3 Anestesiology Division, Hospital de Pediatría Prof. Dr. Juan P. Garrahan. Buenos Aires. Argentina.
4 Neonatal Intensive Care Unit, Hospital de Pediatría Prof. Dr. Juan P. Garrahan. Buenos Aires. Argentina.
*Corresponding Author: Boglione Mariano, General Surgery Division, Hospital de Pediatría Prof. Dr. Juan P. Garrahan. Buenos Aires. Argentina.
Citation: Boglione Mariano, Reusmann Aixa, Aleman Santiago, Rodríguez Paula, Strambach Julieta, Médici Walter, Schaigorodsky Lorena, Dacoff Héctor, Arbio Soledad, and Barrenechea Marcelo (2021). Separation of Thoracoomphalopagus Conjoined Twins. Use of Tissue Expanders and Abdominoplasty According to the San Martín Technique, J. New Medical Innovations and Research, 2(1): DOI: 10.31579/jnmir/005
Copyright: © 2021 Boglione Mariano. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 February 2021 | Accepted: 17 February 2021 | Published: 23 February 2021
Keywords: conjoined twins,thoracoomphalopagus, abdominoplasty, expanders
We present a set of female thoracoomphalopagus conjoined twins who were separated at ten months of age. Tissue expanders were used to expand the available soft tissue to cover the defect. The abdominal wall was closed by making a release incision on the outer aspect of the anterior sheath of the rectus muscle, detaching the anterior sheath of the muscle fibers, and flipping it over towards the midline. Meshes of decellularized collagen matrix were used to close the thorax.
They had no major complications and were discharged from the hospital 60 days later.
The girls are currently 5 years old and lead a normal life according to their age.
We believe that the use of tissue expanders combined with the mobilization of aponeurotic flaps through discharge incisions adds a useful tool for the treatment of these patients.
There are two types of twin pregnancy: dizygotic or fraternal, which represent 70%; and monozygotic, which are around 30%. Sometimes monozygotic twins persist together in some segments after 13 days of embryonic development, and so-called conjoined twins develop, which are classified according to the anatomical region that joins them [1]. Thoracic is the most frequent (40 to 75%), then omphalopagus (15 to 33%), ischiopagus (6 to 10%), and cephalopagus (2%). They are of the same sex and genetically identical. Its frequency varies between 1 in 200,000 to 1 in 40,000 births and occurs in women and men in a ratio of 3 to 1 [2-4].
We present a case of female thoracoomphalopagus conjoined twins who were separated at ten months of age.
Female thoracoomphalopagus conjoined twins born by elective cesarean section at 36.6 weeks of gestation with a joint weight of 3,840 grams from a 27-year-old mother (Figure 1). The diagnosis was made in the prenatal period by ultrasonography and magnetic resonance imaging.

After birth, a brain ultrasound was performed on both girls, which was normal. Echocardiography showed a single pericardial cavity with two hearts in it, without being able to define whether or not they shared ventricular myocardial wall. Abdominal ultrasound observed 4 kidneys, 2 bladders, and one liver fused in the midline that passed from one girl to the other. Two hepatic pedicles were identified in the liver, each consisting of a normal bile duct, hepatic artery, and portal vein. Two suprahepatic venous drainage systems were also observed.
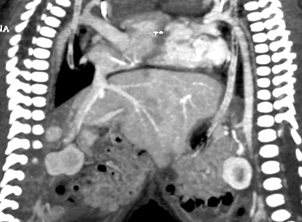
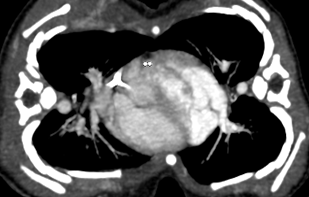
A computed tomography angiogram scan (Figure 2) showed a single pericardial cavity, with two hearts inside. From each heart, and aorta emerged that supplied the rest of the body of each twin, and the venous return was effected through a vena cava for each girl. The liver fused in the midline with two independent vascular and biliary pedicles. Four kidneys forming two independent urinary systems. Each sister had a separate digestive system (esophagus, stomach, small and large intestine). A barium contrast study through a nasogastric tube was performed to verify gastrointestinal anatomy.
The thorax was made up of two rib cages with rectifiedribs that approached 2 sternum outlines (located one on each side), which faced the rectified ribs of the other twin (Figure 3).
Due to the fact that the girls were hemodynamically compensated without the need for any type of medical support, it was decided to delay separation to allow the placement of tissue expanders with the aim of increasing the amount of skin and subcutaneous cellular tissue available for wall closure.
At 9 months of age, 2 expanders of 160 cc each were placed on each shoulder, with the valves externalized by counter-opening. Thirty-five days after placement, it was observed that one of the expanders began to extrude, so it was decided to separate the girls. This was performed 6 days later.
Surgical Technique:
Skin flaps were designed and tissue expanders were removed. A longitudinal skin incision advancing over expanded tissue and a median laparotomy up to the umbilicus, sectioning it in its midline, was performed. The sternum was identified and was sectioned through the midline. Both pleural cavities were opened and phrenic nerves identified. The thymus was dissected free and the single pericardial cavity was incised, observing the complete separation of both hearts. The diaphragm and posterior surface of the pericardium were dissected and sectioned. Both hepatic hila were identified and the liver was sectioned using electrocautery and ultrasonic sealer (Focus®). Hemostasis of liver surface was done with argon gas (Force Fx, Medtronic®). The other sternum (posterior) was incised and then posterior soft tissues were sectioned (Figure 4).

The abdominal wall was closed by making a release incision on the outer aspect of the anterior sheath of the rectus muscle, detaching the anterior sheath of the muscle fibers, and flipping it over towards the midline; according to the San Martín technique.
Due to the inability to approximate both edges of the rib cage, a decellularized collagen matrix mesh (Surgisis®) was placed, attached to both sternal bars with separate braided polyester stitches (Ethibond®) and a second reinforcement suture of the same material.
Closure of subcutaneous tissue flaps was done with 3/0 polyglycolic acid (Polisorb®) and the skin was closed using 4/0 nylon stitches.
Blake® 19 type drains were left in both pleural spaces, and Blake® 15 drains were left inside the abdomen and at subcutaneous tissue.
Both patients received inotropic support for the first 4 postoperative days. They were on mechanical ventilation (MV) for 15 days and non-invasive ventilation (NIV) for another 13 days.
They had no major complications and were discharged from the hospital 60 days later.
The girls are currently 5 years old and lead a normal life according to their age.
Treatment of conjoined twins generates complex ethical dilemmas since the fact of sharing anatomy implies risks of loss of organs or functions, or even life, during separation. This is not always the same for both twins, and sometimes forces physicians to choose between favoring one or the other [5].
Monozygotic twins constitute a deviation from embryological development, because some factor, at a given moment, produces the division of the product of conception. The moment of development at which this division occurs is the factor on which the morphology of the fetuses and the placenta ultimately depends. The division can occur from the second to the fifteenth to sixteenth days after fertilization. Therefore, if the separation takes place before or on the third day (in the 2-cell stage, prior to the development of the inner cell mass), the development potential is complete. In such a situation, two embryos are formed with their corresponding chorion and amnion, that is, a diamniotic and dichorionic gestation occurs.
By the fourth to seventh days after fertilization, the inner cell mass has formed and the outer cells have differentiated into the chorion; the amnion is not yet differentiated, so division at this stage produces 2 embryos, each with its own amnion and covered by a single chorion (ie, a monochorionic and bi-amniotic pregnancy). Finally, if the duplication occurs after the eighth day after fertilization when the trophoblastic cells have differentiated into a single amnion, the pregnancy is monoamniotic and monochorionic; the embryonic disc divides and develops into two complete embryos within a single amniotic sac.
Division of the embryonic disc at any time of development after the date of formation of the embryonic axis, around days 13 to 15 after fertilization, produces an incomplete separation of the embryos. In such a situation, conjoined twins are formed in the same amniotic sac. The binding site can correspond to any embryonic pole [6-8].
Another theory holds that conjoined twins result from the second union of two originally separate monoovular embryonic discs. During the third or fourth week of embryonic development, the previously separated embryonic discs are reattached dorsally (craniopagus, spinal, pygopagus), ventrally (cephalopagus, thoracopagus, omphalopagus, ischiopagus, parapagus) at sites where the ectoderm is absent or open. These areas include the heart, diaphragm, oropharynx, cloacal membranes, neural tube, and the periphery of the embryonic discs [9].
Regarding the optimal moment of separation, bearing in mind that the girls were hemodynamically compensated, feeding orally, and without the need for any type of medical support, we understood that there was no urgency to separate them, so we decided to let them grow for a few months [10].
Because we anticipated insufficient integuments to cover the very large defects that would remain in both patients after separation, we agreed to place tissue expanders on each side of the medial junction area to expand the amount of skin and subcutaneous cellular tissue available [11, 12]. We decided to place the expanders at 9 months of age in order to wait for an increase in the thickness of the subcutaneous cellular tissue that could prevent decubitus and extrusion. Despite this, 35 days after being placed, one of the expanders began to extrude, so it was decided to perform the separation at that time.
The operating room was organized with two anesthesia machines and their respective ventilators, and two complete surgical teams (surgeons and scrub nurses) were arranged. Likewise, as we had not been able to determine whether the girls shared ventricular heart muscle or not, two extracorporeal circulations (cardiopulmonary by-pass) pumps were prepared in the case where necessary.
Once the girls were separated, a very large thoracoabdominal surface was left in each of them. Therefore, to closure the abdominal muscle wall, we used the technique of flipping over towards the midline the anterior sheath of each rectus muscle, as described by San Martín [13]. We had successfully used this technique to repair large abdominal hernias secondary to epithelialization of the amniotic membrane in patients with giant omphalocele [14].
When bringing the sternal edges closer, they compressed the lungs and heart, so we decided to place a prosthesis (mesh) made of decellularized collagen tissue derived from the submucosa of the pig intestine (Surgisis®, Cook Medical). We chose this mesh because it is biodegradable. Other authors report the use of similar meshes, both biodegradable and non-absorbable [15-17].
Both the abdominal muscle wall and the meshes (prosthesis) were seamlessly covered with expanded subcutaneous skin and tissue.
Prenatal diagnosis is important since it allows to study these patients at this stage, searching and detecting associated malformations; and also allows determining the characteristics of shared structures. This information is useful to support parents, instruct them on the prognosis of these children, and program and plan neonatal management in a tertiary care center [18, 19].
The only indication of emergency separation is when one of the twins is dying or already dead and an attempt is made to maintain the life of the other. Undoubtedly, emergency separation has a high mortality rate, which decreases with coordinated and planned separation. Those that require emergency separation have survival ranges of 30 to 50%. Scheduled surgery raises the survival range from 80 to 90% [20, 21]. Although in our case we had to advance the separation due to the extrusion of one of the expanders, this did not imply a risk of life for them and they were always hemodynamically compensated.
We believe that the use of tissue expanders combined with the mobilization of aponeurotic flaps through discharge incisions adds a useful tool for the treatment of these patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
