
Review Article | DOI: https://doi.org/10.31579/2768-2757/056
Ippokratous 209, 11472, Athens, Greece.
*Corresponding Author: Chrisostomos Sofoudis MD, Ippokratous 209, 11472, Athens, Greece.
Citation: Chrisostomos Sofoudis. (2022). Sentinel Node in Endometrial Cancer. Metastatic Pathways. Journal of Clinical Surgery and Research, 3(5); DOI:10.31579/2768-2757/056
Copyright: © 2022 Chrisostomos Sofoudis. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 July 2022 | Accepted: 29 August 2022 | Published: 04 August 2022
Keywords: sentinel node; endometrial cancer; staging; grading
Endometrial cancer represents the second most frequent malignant entity among gynecologic malignancies.
Many predisposition factors reflect and affect the chronical outcome of the lesion.
Age of the patient, obesity, postmenopausal vaginal bleeding among with endometrial hyperplasia, histologic type, grading, staging, vascular or lymph node penetration consist factors with direct depiction concerning the therapeutic mapping.
Sentinel node consists the first regional lymph node infiltration, indicating local or external spread of the lesion.
In order to explore and investigate potential infiltration or metastatic capability of the lesion, sentinel mode infiltration represents optimal solution.
According to current literature, sentinel node infiltration depicts increased sensitivity and specificity concerning surgical or conservative therapeutic management.
Aim of our study represents assiduous decoding of sentinel node infiltration and potential metastatic pathways, with ultimate scope the increased optimal survival and quality of life of the patient.
According to current literature, endometrial cancer consists the 2nd most common gynecologic malignancy in developed countries. [1] Focusing on imaging depiction and assiduous reflection of all predisposition factors, most of cases are nearly diagnosed. [2] Endometrial cancer classification remains the most diagnostic tool regarding the therapeutic mapping of such cases. (Table I.)
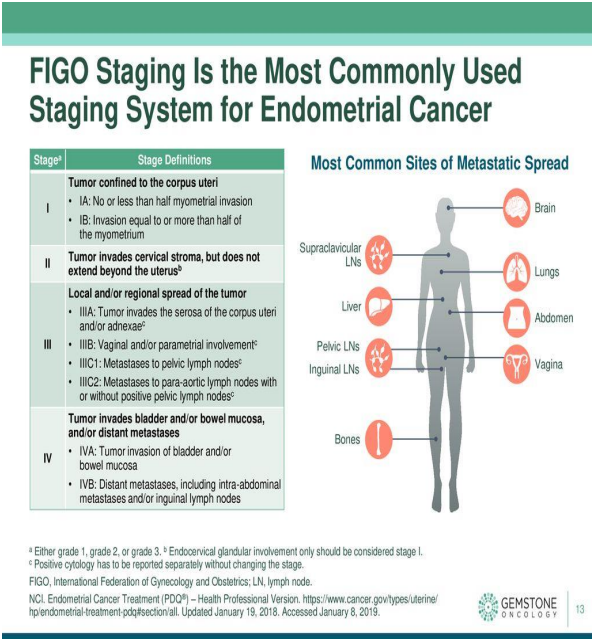
Figure 1: FIGO Endometrial Cancer Classification. Gemstone Oncology
Among age of the patient, staging, grading, postmenopausal bleeding, histologic type, lymph node infiltration presents as most significant prognostic factor. [3] Optimal treatment of endometrial cancer consists total abdominal hysterectomy accompanied with bilateral salpigo oophorectomy. Further surgical intervention is strongly adjusted with the lymphatic infiltration and the staging of the lesion. In cases of more than 50 % of myometrial invasion, bilateral lymphadenectomy should be performed. [3] Many conducted studies have proposed in cases of advanced stages, series of chemotherapy with radiotherapy, combined with hormonal therapy when estrogen and progesterone receptors were found positive. [4] Sentinel node consists as primary lymphatic external spread of each malignant entity. [5] Many recent studies have been conducted mostly in areas such breast malignancies or melanomas with great successful therapeutic management. Cutaneous melanomas presented as primary malignancies in which SLN mapping depicted worldwide acceptance. In cases of vulvar cancer SLN mapping managed to bring promising results in order to establish more precise therapeutic strategy. Radio colloid and blue dye SLN mapping were first described in the early 1990s. Lymphoscintigraphy in the early 1980s was initially used for SLN mapping in breast malignancies. Since 1977, SLN mapping procedures have been included in the treatment for a number of types of tumor, including vulvar, breast, anal, colon, skin, gastric, penile, esophageal, bladder, prostatic neoplasm and non-small cell lung cancer. According to current bibliography, SLN mapping was depicted with Technetium Radio colloid (99Tc) alone or with blue dyes. Besides the daily use of these substances, many side effects were described. [6] In many cases, skin and urine discoloration or allergic reactions were presented. Indocyanine green (ICG) consists an intravascular fluorescent dye, optimal tool concerning the visualization of retinal and choroid vascularization. [6]
Discussion
Many recent conducted studies, establish ICG as screening tracer regarding the SLN (Sentinel Node) mapping in endometrial cancer. Indocyanine green (ICG) consists a tricarbocyanine dye which can lead to emission of a fluorescent signal in the infrared light range capable of detecting the first lymphatic drainage concerning cases of endometrial cancer. Fluorescence‑guided imaging with ICG has a number of advantages, compared with conventional methods, including real-time lymphography, a low incidence of adverse reactions and an increased sensitivity, without requiring radiation. Isolation and detection of SLN biopsy enables complete mapping of potential lymphatic infiltration. [7] Besides the low rate of lymphatic invasion in early stages of endometrial malignancies, complete lymphadenectomy represents ultimate scope of precise endometrial cancer staging. [7] (Figure I.)
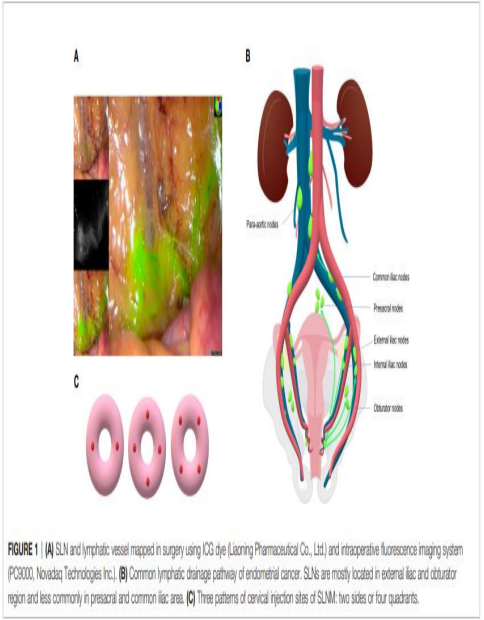
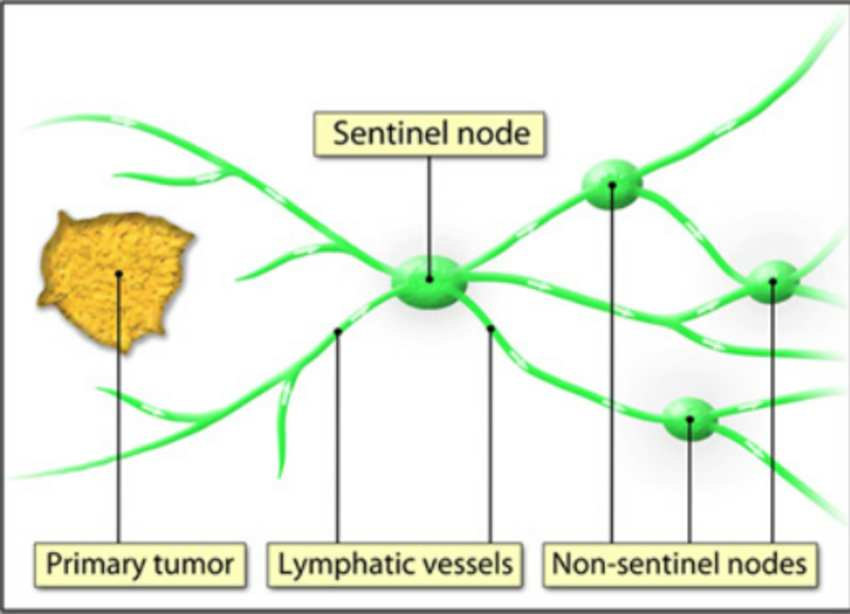
Figure 3: Sentinel lymph node drainage in endometrial cancer. Sentinel Lymph node mapping in endometrial cancer: a comprehensive review. Zhai et al. Front. Oncol., 29 June 2021.

Figure 4: Sentinel node depiction after ICG application.Laparoscopic sentinel node mapping complicating endometrial cancer. Report of three cases and systematic review of the literature. Sofoudis C, Syrios K, Oikonomidis M, Betas P, Zioris K. Obstet Gynecol Int J 2022;13(2):135-138
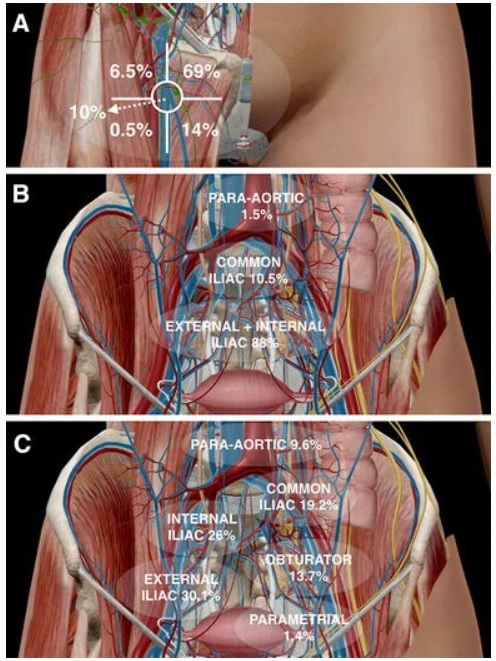
Lymph node staging and lymph vascular invasion and infiltration consist without doubt ultimate prognostic factors. [8] Myometrial infiltration is strongly accompanied with nodal metastasis. Recent literature depicts nodal metastasis less than 3% in cases with less than 50% myometrium infiltration. [9] Due to anatomic area of the uterus (midline structure), lymphatic spread divides into bilateral pelvic lymph nodes. On the other side, depiction of one at least SLN in every hemi pelvis area, underlies the significance of SLN mapping. Many conducted studies raised from current literature, perform different ways of injecting ICG. Optimal decoding of these manuscripts underlies the significance of the pathophysiologic mechanism. The injection is diffused around 3rd and 9th para cervical hour, before setting and beginning of the laparoscopic exploration. (0,5-1ml superficial/1-3mm) and (0,5-1ml in depth/1-2cm) (Figure III.) [10]
An alternative injection method represents the four clock positions. In many cases the injections were placed intracervical at 2,4,8,10 o’clock positions. (Figure IV.) [10] Only obstacle presented by cervical method depicts the decreased para-aortic detection rate in comparison with the endometrial method via hysteroscopy. [11] Pathophysiologic mechanism of this method reflects the avoidance of ICG into the cervical arteries which can lead to diffusion of the dye into the systematic circulation causing many operative complications. [12]
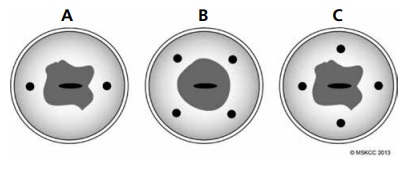

Figure 7: Sentinel Lymph Node mapping procedures in endometrial cancer. Boruta D.M, Chapter 12, Translational Advances in Gynecologic Cancer.
ICG injection is strongly accompanied with patient’s body mass index. In almost 20 min. complete lymphatic spread is being depicted. Sentinel node consists the first lymph node infiltration concerning the lymphatic spread. Staging of the lesion is strongly accompanied with number and lymphatic penetration depth. [13] Positive lymphatic spread of SLN consists with appearance of macro metastasis (tumor spread > 2mm), micro metastasis (tumor spread 0,2- 2mm) and isolated tumor cells (tumor spread< 0,2mm). [14] Classical surgical therapeutic mapping in cases of endometrial cancer consists total hysterectomy, bilateral salpigoopherectomy and complete pelvic lymphadenectomy due to staging of the lesion. [15] Less radical mapping reflects in low risk cases (FIGO IA, grade 1-2). Decoding current bibliography, lymph vascular dissection seems to be controversial. [16] In cases of complete and assiduous bilateral lymphadenectomy, many potential operative and post-operative surgical complications can be performed. [17] Lymphedema local or diffuse accompanied with abdominal pain, skin breakdown and severe increased patient’s quality of life consist examples of postoperative complications. Extended surgical intervention, nerve injury and potential blood loss in cases of complete lymphadenectomy, accelerate the entrance of SLN evaluation. Focusing on SLN mapping as ultimate recurrence factor, depiction of lymph vascular infiltration, leads to postoperative strategy, such as adjuvant therapy. Although in most of cases preferred SLN technique consists 99m Tc and preoperative lymphoscintigraphy, SLN detection with ICG reflects new diagnostic pathways. [18] Many conducted studies suggest SLN mapping with ICG incidence of overall detection from 84% and 100% and more specific increased bilateral detection rate from 71% and 84%, without doubt higher than 58% and 75% of the classical technique (99m Tc and blue dye). [19] SLN mapping with ICG allows more increased drainage of the contrast substance and depicts visualization of the whole pelvic lymphatic route in real time. IGC technique consists an easily medical intervention, independent from patient’s BMI without adequate surgeon’s experience. SLN detection procedure is based on the SLN protocol of Memorial Sloan-Kettering Center with H& E stain and CKAE1/AE3 immunostaining (Table I.) [20]. Many conducted studies arise from current literature have adopted the Memorial Sloan Kettering Cancer Centre SLN mapping. According to these studies, detection rate of SLN was calculated. Detection rate is equal with the ratio of number of patients with SLN positive to the number of patients who underwent SLN mapping. Additionally, positive and negative prognostic value can be calculated. Most significant prognostic factors concerning SLN consist sensitivity and specificity of the method. [21] Many recent studies express higher sensitivity rather than specificity, concerning SLN mapping due to false negative cases. On the contrary, in well-organized medical centers SLN mapping can lead to decrease of false negative patient numbers as well depiction of aortic metastatic lesions. [21] With the assiduous studies of Abu-Rustum et al., a low curve of false negative patients was reflected. According to recent bibliography, there are cases with SLN mapping failure. Besides lack of medical expertise, lymphatic obstruction due to tumor infiltration, obesity and only use of contrast medium represent failure factors concerning SLN mapping. [22] (Figure VI.)

Table 1: Memorial Sloan Kettering Cancer Centre SLN mapping. Int. J. Gynecol Cancer 2013 June 9:23(5:964-970).
Many conducted studies arise from current literature have adopted the Memorial Sloan Kettering Cancer Centre SLN mapping. According to these studies, detection rate of SLN was calculated. Detection rate is equal with the ratio of number of patients with SLN positive to the number of patients who underwent SLN mapping. Additionally, positive and negative prognostic value can be calculated. Most significant prognostic factors concerning SLN consist sensitivity and specificity of the method. [21] Many recent studies express higher sensitivity rather than specificity, concerning SLN mapping due to false negative cases. On the contrary, in well-organized medical centers SLN mapping can lead to decrease of false negative patient numbers as well depiction of aortic metastatic lesions. [21] With the assiduous studies of Abu-Rustum et al., a low curve of false negative patients was reflected. According to recent bibliography, there are cases with SLN mapping failure. Besides lack of medical expertise, lymphatic obstruction due to tumor infiltration, obesity and only use of contrast medium represent failure factors concerning SLN mapping. [22] (Figure VI.)
Many conducted studies are focusing on morbidity minimization due to SLN mapping. In advanced stages of endometrial cancer, negative histopathologic evaluation of SLN can lead to lack of paraortic complete bilateral lymphadenectomy, down staging of the lesion and increase of overall survival, free disease survival and patient’s quality of life. [23] (Figure VII.)
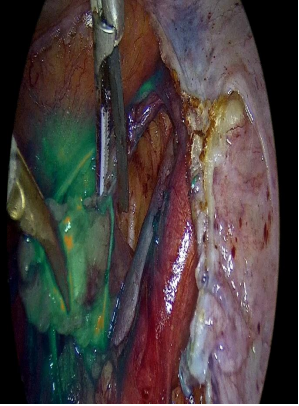
Figure 9: Laparoscopic right sentinel node dissection. Laparoscopic sentinel node mapping complicating endometrial cancer. Report of three cases and systematic review of the literature. Sofoudis C, Syrios K, Oikonomidis M, Betas P, Zioris K. Obstet Gynecol Int J 2022;13(2):135-138.
According to recent literature, many conducted studies suggest SLN mapping as alternative therapeutic strategy towards systematic pelvic and para-aortic lymph node dissection in cases with low grade endometrial cancer and second thinking for cases with high grade endometrial cancer. (Figure VIII.) Many well organized surgical centers take advantage of increased medical equipment and manage to determine precise therapeutic alternatives towards premenopausal patients with endometrial cancer focusing on potential fertility preservation.
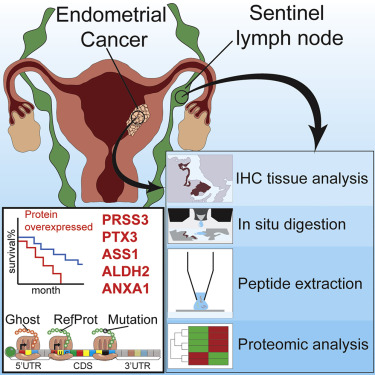
After the establishment of SLN mapping especially in cases of low risk endometrial cancer, critical question of all recent conducted studies remains what will be the crucial next step. Focusing on histologic type in cases of endometrial cancer such as clear cell or serous endometrial cancer and staging of the lesion such as cases with grade three type, many organized centers across Europe or in the U.S. working towards a SLN protocol absolutely acceptable in order to establish more accurate and precise therapeutic strategy. [21] Resulting in many conducted studies and algorithm proposals, surgical randomized trials with SLN mapping have been performed. STATEC (Selective Targeting of Adjuvant Therapy in Endometrial Cancer) represents a randomized phase 3 study, which includes two independent groups. [24] Study group depicting patients underwent total hysterectomy with pelvic and para-aortic node dissection with optional SLN mapping comparing with control group of patients underwent total hysterectomy without pelvic and para-aortic dissection in cases of extended stages of endometrial cancer. [21] Focusing on the increased step of medical technology, molecular analysis of SLN mapping could provide promising information regarding early diagnosis of endometrial cancer cases. [21] Aboulouard et al. suggested in depth molecular analysis of proteomics variations in SLN proteins, comparing with parallel analysis inside proteins of endometrial tumors. [25] These protein variations depict potential markers with direct affection of overall survival. Five major proteins for EC and SLN (PRSS3, PTX3, ASS1, ALDH2, and ANXA1) were identified in large-scale proteomics and validated by immunohistochemistry. Study of Aboulouard et al. consists protein correlation of SLN mapping and endometrial cancer, optimal tool concerning early or advanced stages of endometrial cancer. (Figure IX.)
This conducted study reflects promising pathways in order to establish optimal therapeutic strategy in cases of endometrial cancer affecting especially premenopausal patients direct correlated with fertility preservation.
Author declares any financial interest with respect to this manuscript.
Endometrial cancer represents the 2nd most often gynecologic malignancy after cervix carcinoma among female population.
SLN mapping depicts first lymphatic drainage throughout lymphatic channels.
Increased sensitivity and decreased false negative rate lead to promising pathways concerning less surgical interventions and less intraoperative and postoperative potential complications.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
