
Case Report | DOI: https://doi.org/10.31579/2693-4779/099
1 Topmed Medical Center, Tîrgu Mureș, Romania.
2 Resident Laboratory srl, Oradea, Romania.
*Corresponding Author: Corina Florica Ioniță, Topmed Medical Center, Tîrgu Mureș, Romania.
Citation: Corina Florica Ioniță, Adriana Gomotîrceanu, Daniela Cojocaru, Florin Costea, Ovidiu Pop. (2022) Seminal vesicle adenocarcinoma associated with Zinner Syndrome: case report and literature review. Clinical Research and Clinical Trials. 6(1); DOI:10.31579/2693-4779/099
Copyright: © 2022 Corina Florica Ioniță. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 May 2022 | Accepted: 18 May 2022 | Published: 25 May 2022
Keywords: zinner syndrome; seminal vesicle carcinoma
The Zinner Syndrome is a rare congenital malformation represented by a triad of characteristics: ipsilateral renal agenesis, seminal vesicle cysts and ejaculatory duct obstruction. The aim of this study is to present a 69 year old man case, with seminal vesicle adenocarcinoma developed in association with Zinner Syndrome.First off all, patient presented with severe urinary retention. Had clinical and imaging examinations: ultrasound scan, computed tomography of the chest, abdomen and pelvis, abdominal-pelvic MRI and biochemical evaluation: PSA. As a result, diagnosis of Zinner Syndrome has been established and was suspected a carcinoma of seminal vesicle. The pacient underwent robotic removal of the tumoral cyst. The postoperative evolution of the patient was uneventful. The diagnosis of seminal vesicle adenocarcinoma was confirmed by immunohistochemistry, staining negative for PSA and positive for CK7. Seminal vesicle carcinomas are particularly rare. Their occurrence in patients with Zinner Syndrome is exceptional, but should be considered in differential diagnosis of pelvic tumors.
PSVA: Primary seminal vesicle adenocarcinoma
MRI: Magnetic resonance imaging
CT: Computer tomography
PSA: Prostate specific antigen
CK: Cytokeratin
AMACR(p504s): Alpha methyacyl CoA racemase
Primary seminal vesical adenocarcinoma (PSVA) is a rare malignancy, of the male genito-urinary system which sporadically occurs, with only 60 documented cases in literature [1,2]. Because of the fact that the symptoms are not specific and because it is difficult to diagnose, most cases are discovered in extensive stage or metastatic, with prostate invasion or lung metastases, therefore the prognostic is poor [3]. Despite the fact that there are no standard guidelines, basic treatment is considered to be surgical intervention with seminal vesiculectomy. Due to the anatomical features and because many cases are late diagnosed, frequently post intervention there is residual disease which needs further adjuvant treatment. Immunohistochemistry plays an important role in differentiation of the primary tumor and documentation of the origin’s site. Adjuvant treatment consist in radiotherapy, chemotherapy or both, and in some cases anti-androgen therapies [4].
Zinner Syndrome is characterized by unilateral renal agenesis, seminal vesicle cysts and obstruction of the ejaculatory ducts, due to developmental disorders of the intrauterine life in 2-4 weeks of gestation [5]. The purpose of this study is to present a rare case of seminal vesicle adenocarcinoma associated with Zinner Syndrome.
A 69 year old man presented with constipation, unspecific pain in the lower region of the abdomen and urinary retention and was admitted in our service. He had no important medical history. Abdominal ultrasound revealed a pelvic cystic tumor of 11 cm diameter, first misdiagnosed as the bladder. A urinary catheter was inserted and urine was eliminated, but the cyst’s dimension remained the same, therefore suspicion of a pelvic tumor was raised. The digital rectal examination revealed the existence of a tumor of about 10 cm, which was coming in contact with the anterior rectal wall, without being able to specify the organ belonging, taking into consideration the intimate contact with the prostate.
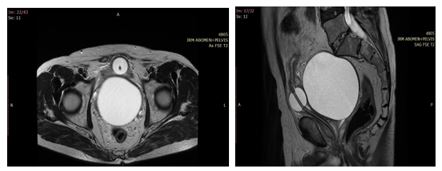
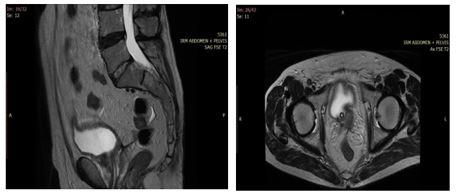
In order to elucidate the diagnosis, it was decided to practice abdominal-pelvic MRI, using a GE Signa Explorer 1.5T device, 2019.
The MRI confirmed the pelvic cyst of 11 belonging to the right seminal vesicle, with a polypoid proliferation of 15 mm attached to the inner slope of the wall with a wide implantation base, without lymph node involvement or spread to the other organs, without apparent extension in or beyond the cystic wall.
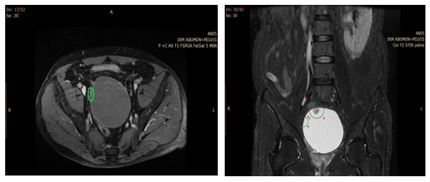
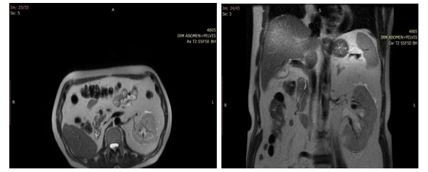
It also highlighted renal unilateral right agenesis and ejaculatory right duct obstruction, so the patient had been diagnosed with Zinner Syndrome. Preoperative value of PSA was double than normal, testosterone level was normal.
On august 2021, it was performed robotic excision of the tumor cyst. The postoperative evolution was favorable, patient being discharged on the 4th postoperative day. The anathomopatological examination confirmed a seminal vesicle tumor cyst with friable papillary projections over an area of 3/3 cm on the inner wall represented by an adenocarcinoma predominant papillary architecture, focally tubular. The tumor invades the wall of the cyst focal in the area of intersection with the prostate and infiltrates the prostate stroma over short distances.
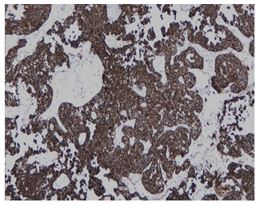
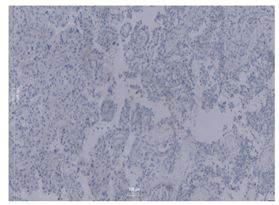
Histological examination indicated negative surgical margins, without perineural or angiolymphatic invasion, The IHC (immunohistochemically) study revealed positivity for CK7, AMACR (p504s), GATA3, and negativity for PSA, CDX-2, p63, AR and NKX3.1, that is why the diagnosis of primary seminal vesicle adenocarcinoma was confirmed.
PSA values increased slightly in the postoperative period, therefore suspicion of prostatitis was raised, which is why treatment with antibiotics and anti-inflammatory drugs was prescribed. Postoperative levels of CEA and ACE were within the normal range.
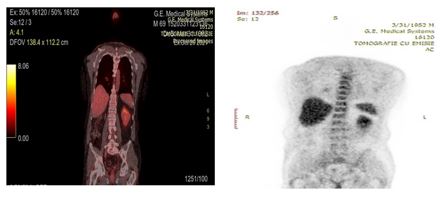
Postoperative abdominal-pelvic MRI and PET-CT (positron emission computed tomography) made at one, respectively two month from surgical intervention did not give evidence of residual disease.
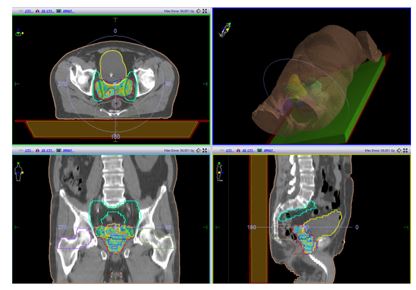
Patient did not receive adjuvant chemotherapy, because there was not lymph node involvement or positive margins at the histopathological exam of the surgical specimen. Adjuvant radiotherapy was established within the multidisciplinary commission, because of the cystic volume and high risk of recurrence.
Patient performed 5 weeks of postoperative radiotherapy sessions with Elekta Infinity Device, type 2020, VMAT-SIB technique (volumetric modulated arc therapy - simultaneous integrated boost) up to 56Gray/25fractions, 2.24 Gray/fractions at tumor bed, prostate and at pelvic lymph nodes.
Treatment was well tolerated, with no side effects during the radiotherapy sequences. Patient is due follow-up appointments every 3 months in the first year and then every 6 months for another 4 years. So far the patient has show no signs of recurrence.
Adenocarcinomas of the seminal vesicles is the most common malignant primary neoplasm of the seminal vesicles. The first adenocarcinoma of the seminal vesicles was reported in literature by O. Lyons in 1925[6]. It can occurs at different ages from 19 to 90 years old [7]. There are a small number of cases of bilateral PSVA [2,8]. Uncommon neoplasm of the seminal vesicles are sarcomas, neuroendocrine carcinoma, squamous cell carcinoma or yolk salk tumor.
Because there are not specific symptoms, male usually are diagnosed at advanced stages [9-12]. Most frequently the symptoms are hematuria, dysuria, haematospermia, unspecific pelvic pain. Digital rectal examination can indicate the presence of a tumor in the seminal vesicles in up to 30% of cases. CT and MRI give the best evidence of the extent of the tumor. However, there have been cases cited in the literature in which imaging examinations were inconclusive (including endorectal ultrasound), which is why the definite diagnosis is based on biopsy [13].
Based on imagistic findings, there must be a differential diagnostic between malignancies of the seminal vesicles and the prostate cancer, bladder cancer, rectal cancer. Due to the anatomical location the most difficult difference is with prostate cancer, but the PSA level is defining
It should be noted that all tumors derived from the seminal vesicles are cystic. By association, these malignant tumors can be considered cystic malignancies, so we could say that this is a case of cystadenocarcinoma, but we didn’t find literature data to support this.
Because of the cystic appearance of this tumor it was necessary to discriminate it from a benign tumor, such as cystadenoma or a cystic malignancy like cystosarcoma, but in our case these diagnostics were invalidated by histological examination [14]. The existence of intracystic proliferation in this case, observed in imaging examinations, may represent a suspicious sign of malignancy. If it is possible to demonstrate the presence of vascularization in the proliferation by CEUS for example it will be a strong argument for a malignancy.
Immunohistochemistry is very important for the histological diagnosis. Stains are usually positive for CA-125 , CK7, CEA, while PSA and CK20 should be negative.
Given the small number of cases published in the literature, there is no consensus on staging. Due to the fact that the tumor was intracystic, with extension focally in the wall of the cyst and infiltrates the prostate stroma over short distances, we can consider it a stage III.
The prognosis is poor, given the fact that most patients die within 3 years, probably due to the advanced stage in the moment of diagnosis. The most important contribution for survival is the quality of the surgical resection, which usually is difficult to perform due to the local anatomy and cystic structure [3]. It is unclear if it is necessary prophylactically to resect the draining lymph nodes, especially if they are negative on imagistic findings. Radiotherapy is often used for residual tumors or tumors with positive margins after surgery [15,16].
The role of chemotherapy is unclear. It is though recommended in patients with metastases or with residual tumor. The most frequent combination is Gemcitabine plus Cisplatinum in fit patients, followed by radiotherapy [2]. In patient with metastases, usually chemotherapy convert to a lower stage.
Anti-androgen therapy is used as an adjuvant or palliative treatment for androgen-dependent PSVA, but the results are unclear [17]. In our case, testosterone levels serum were normal, so there was no recommendation for such therapy.
The Zinner Syndrome is a rare congenital malformation, frequently associated with infertility. Surgery is the main treatment, especially on symptomatic patients [18]. The appearance of Zinner Syndrome is due to abnormalities in the development of Muller's duct in men.
Zinner Syndrome diagnosis is common in men between the 2nd and 4th decade of their life, and is usually asymptomatic until this age. Recently, the number of cases cited in the literature had increased significantly with accuracy of imaging methods [19]. Due to the fact that approximately 45% of patients with Zinner Syndrome are infertile, diagnosis is sometimes given during infertility investigations [20]. Therefore, in patients with confirmed infertility, the existence of renal agenesis or obstruction of the deferent duct requires the exclusion of the existence of Zinner Syndrome.
Frequently, seminal vesicle cysts are difficult to diagnose given surrounding anatomical structures, often being confused with ureters or diverticula of the bladder. As a therapeutic attitude, in some cases the conservatory attitude is preferred. If patients become symptomatic, surgical excision of the seminal vesicle cysts is recommended by open, classic or laparoscopic surgical approach, respectively robotic. Cases have been reported in the literature of patients who have had a puncture of these cysts, but they frequently recur [21].
The occurrence of seminal vesicle cancer in patients with Zinner Syndrome is particularly rare, with very few cases being mentioned in the literature. The most frequently cases were adenocarcinomas or squamous cell carcinomas [22]. There are also mentioned cases of patients with Zinner Syndrome who have been diagnosed with clear prostate cell carcinoma [23].
The particularity of the presented case is represented by the appearance of a seminal vesicle carcinoma in a patient with Zinner Syndrome.
The belonging of a cyst in the lower abdomen, should raise the suspicion of a seminal vesicle cyst.
Seminal vesicle adenocarcinomas are particularly rare, but must be taken into account in the diagnosis of pelvic tumors. They are an even rarer occurrence in patients with Zinner Syndrome. So when a patient is discovered with Zinner Syndrome probably he must be imagistic monitored for the detection of intracystic proliferation.
The patient agreed to publish this manuscript.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
