
Research Article | DOI: https://doi.org/10.31579/JHV-2021/005
*Corresponding Author: James Elliott, Department of Vascular Surgery, Princess Alexandra Hospital, Queensland, Australia.
Citation: Elliott J., Lal V., McGahan T., Stacey L. BMaths (2021) Selection of patients with ruptured abdominal aortic aneurysm for long distance inter-hospital transfer in Australia J, Heart and Vasculature 1(2); DOI: 10.31579/JHV-2021/005
Copyright: © 2021, James Elliott, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 March 2021 | Accepted: 10 March 2021 | Published: 08 April 2021
Keywords: ruptured abdominal aortic aneurysm; surgery; surgical repair
Backgrounds: It is possible that a patient with Ruptured Abdominal Aortic Aneurysm (rAAA) who has features of critical illness, may receive a futile inter-hospital transfer for treatment in a tertiary centre. The goal of this study was to better identify patients who will benefit from transfer and surgery, so that these limited resources can be used effectively where needed.
Methods: All patients diagnosed with rAAA at this institution over a study period of 10 years were analysed. Data collection was conducted via a retrospective chart audit. Primary outcome was 30-day mortality for patients who undergo surgical repair.
Results: No evidence of an association between transferred and not transferred patient populations was found for the primary outcome of 30-Day mortality (p=0.94). There was slight evidence of an association between 30-Day mortality and transfer distance (p=0.048), with a higher frequency in those transferred less than 100km compared to those who travelled further (41% vs. 19%, respectively). Some evidence of an association was found for intervention type (p=0.038), with mortality in 37% of patients who had an open repair surgery, compared with 14% for patients who underwent EVAR surgery. There was also evidence of an association with an initial presentation of ALOC (p=0.005), and requiring inotropic/vasopressor support upon initial presentation (p=0.037).
Conclusions: Patient transfer from another hospital was not found to be associated with increased 30-day mortality. The data in this study supports the practice of offering treatment to patients with rAAA who are referred from distant (≥100km) locations.
This is a retrospective observational study of all patients diagnosed with rAAA at this institution from January 1st 2009 to Dec 31st 2018 (10 years). Inclusion criteria includes patients with a diagnosis of ruptured AAA clinically and/or radiologically or as a surgical finding within the specified date range. Exclusion criteria included patients with a non-ruptured, symptomatic or infected AAA. Patients who had a history of previous Abdominal Aortic intervention were also excluded.
Primary outcome is 30-day mortality. Other measures include patient age; gender; serum creatinine on first presentation; serum Hb on first presentation; transferred (transfer distance) or not transferred; surgical management of AAA or not (and if so, EVAR vs Open Surgical Repair); Any Systolic Blood Pressure (SBP) measurement of <80mmHg; Altered level of consciousness (ALOC); presence of Hypothermia (temperature <35degrees Celsius); Transfusion of 4 or more units of Packed Red Blood Cells (PRBCs) pre-surgery; evidence of Myocardial Infarction (MI) pre-surgery; Inotropic/vasopressor support pre-surgery; post-op MI/CVA/Dialysis. The presence of shock was recorded. Shock was defined as the presence of any one of these pre-operative features: Any SBP readings <80mmHg, ALOC at initial presentation, Transfusion of at least 4 units of PRBCs, Inotropic support. The subsequent Glasgow Aneurysm Score was calculated for each patient.
Associations between patient groups of interest and categorical patient characteristics, in the populations of interest, were examined using χ2 tests of independence or the Fisher’s exact test, where more than 20% of the expected values were less than five. Associations between patient groups of interest and continuous patient characteristics were examined using a two-sample t-test. Categorical patient characteristics were summarised by frequency and percentage and continuous patient characteristics were summarised by mean and standard deviation (SD). Statistical analyses were performed in Stata version 15 (StataCorp, College Station, TX, U.S.A.).
The receiver-operator characteristic (ROC) curve with the Youden index was used to determine which Glasgow aneurysm score (GAS) cut-off was predictive of postoperative mortality. Logistic regression was used to investigate the association of GAS to 30-day mortality, at the 5% significance level. Statistical analyses were performed in Stata version 15 (StataCorp, College Station, TX, U.S.A.). Logistic regression was used to investigate the association between year (as a continuous predictor) and use of EVAR surgery, at the 5% significance level. Statistical analyses were performed in Stata version 15 (StataCorp, College Station, TX, U.S.A.).
Approval for the conduct of this study has been granted by the Metro South Hospital and Health Service Human Research Ethics Committee in accordance with the ethical standards laid down in the Declaration of Helsinki.
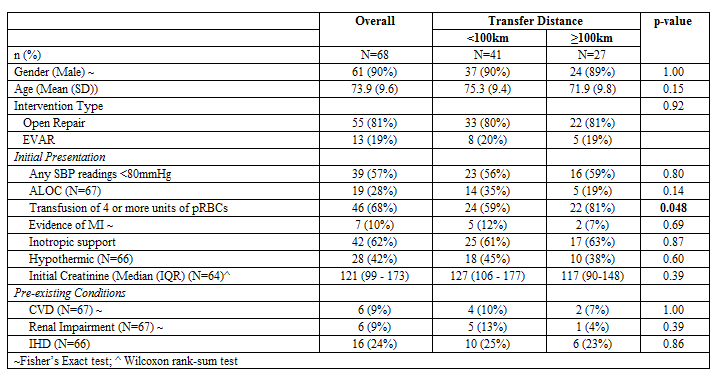
A total of 158 patients met inclusion. 79 patients (50%) had their initial presentation to the tertiary hospital, 79 patients (50%) were transferred to the tertiary hospital from a smaller institution without a dedicated Vascular Surgery unit. A total of 109 patients proceeded to surgery (87 underwent open repair, 22 underwent EVAR) (see table 1). The patients that met inclusion were then further divided into 3 surgical groups: those who presented locally (n=41), those who were transferred <100km from another institution (n=41), and those who were transferred ≥100km (n=27) from another institution. No evidence of an association with markers of pre-operative critical illness, GAS or shock, between these groups was found.
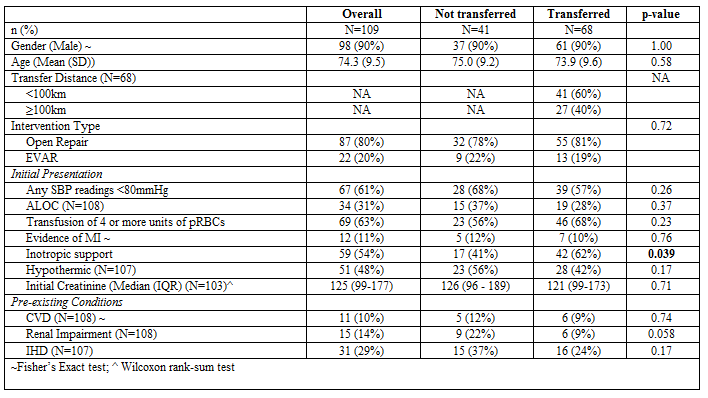
Amongst all patients who proceeded to surgery, there was a higher proportion in the transferred group who required inotropic support compared to the non-transferred group (62% vs. 41%, respectively; p=0.039). A larger proportion of patients (81%) in the ≥100km transfer distance group required transfusion of 4 or more units of PRBCs than in the <100km transfer distance group (59%) (p=0.048, table 2).
Of all patients undergoing surgery, 11 patients (11.2%) had a post-operative Myocardial Infarction (MI), 6 patients (6.3%) suffered post-operative Stroke/Cerebrovascular Accident (CVA), 15 patients (15.3%)
required post-operative haemodialysis/renal replacement therapy. Post-operative complications were not associated with inter-hospital transfer (see table 3).

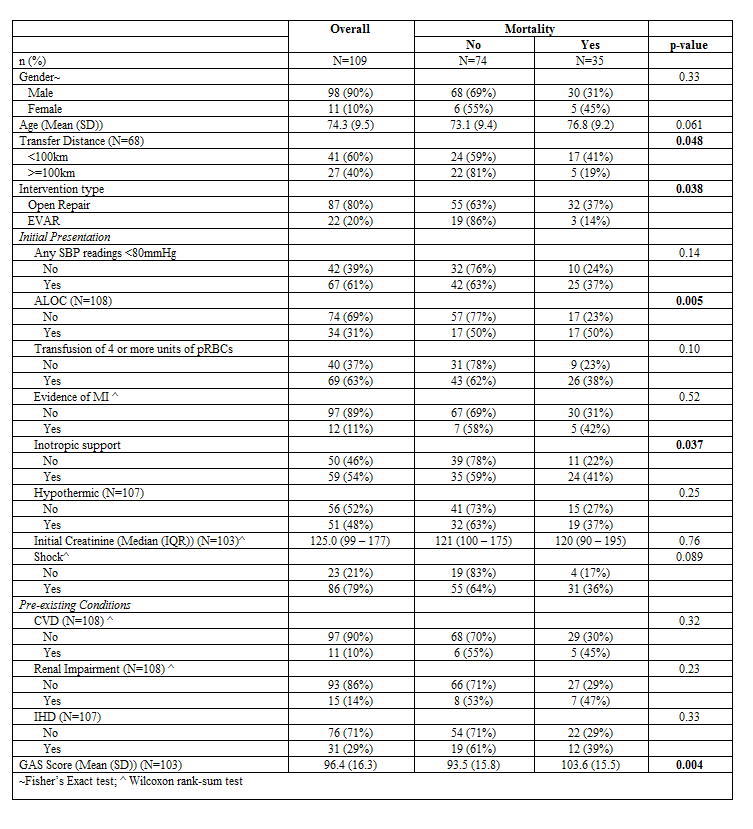
In patients who proceeded to surgery, no evidence of an association between transferred (regardless of distance) and non-transferred patient populations was found for the primary outcome of 30-Day mortality (p=0.94) with mortality for 32% and 38% of patients in each transferred and non-transferred group, respectively. There was slight evidence of an association between 30-Day mortality and transfer distance (p=0.048) (see table 4), with a higher frequency in those transferred less than 100km compared to those who travelled further (41% vs. 19%, respectively). Some evidence of an association was found for intervention type (p=0.038), with mortality in 37% of patients who had an open repair surgery, compared to 14% for patients who had EVAR surgery.
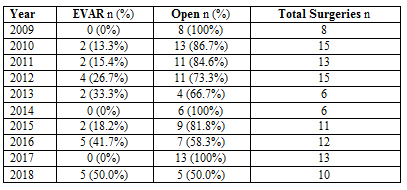
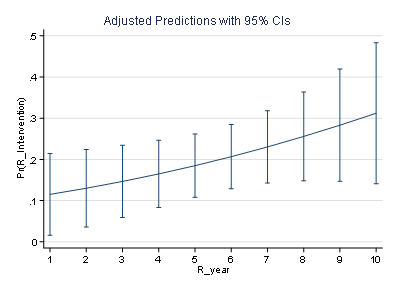
Open Repair vs EVAR was evaluated, as there were lower rates of EVAR than expected. Table 5 presents the number and percentage of the surgical intervention types for each year. A total of 87 Open repair and 22 EVAR surgeries were performed. Table 6 presents the logistic regression model for year as a predictor of EVAR surgery use, the model does not suggest evidence of a statistically significant association (OR 1.15, 95% CI: 0.97 to 1.36; p=0.101. Figure 1 provides the average predicated probability of EVAR surgery use over the ten year period. Although a trend can be noted in increasing probability, the large confidence intervals for each year, for which the predicted probabilities overlap across all years, highlight the insufficient evidence for a statistically significant relationship.

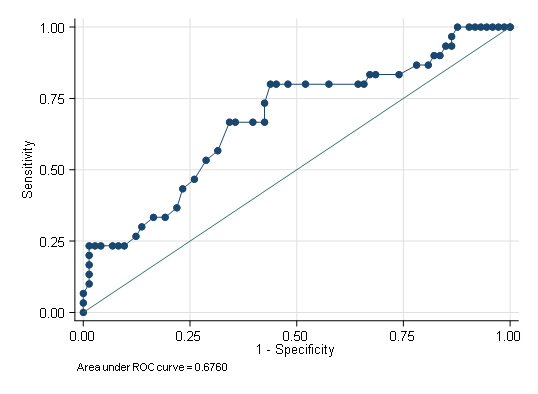
Evidence of associations with increased mortality rate were found with presentations that included ALOC (50% vs. 23% p=0.005) and requiring inotropic/vasopressor support (41% vs. 22%, p=0.037). The GAS Score was found to be strongly associated with mortality (p=0.004) in this study. Table 7 presents the logistic regression model for GAS score as a risk factor for post-operative mortality. There was strong evidence to suggest that the odds of post-operative mortality increased by a factor of 1.56 for each 10-unit increase in GAS score (95% CI: CI: 1.14 – 2.13, p=0.006). ROC curves showed the optimum GAS score cut-off was 95, at which the correct classification rate was maximised with a sensitivity of 80.0%, specificity of 56.1% and an Area Under the Curve (AUC) of 0.68 (95% CI: 0.56 – 0.79), as shown in Figure 2. Patients in the study population with a GAS score lower or equal to 95 had a mortality of 13% (6/47), compared with 43% (24/56) for a higher score (p=0.001).

68/79 (86.1%) of those who were transferred had surgery vs 41/79 (51.9%) of those who presented directly to this institution. Operative mortality overall was 35/109 (32%). Operative mortality in those presenting locally was 13/41(38%). Operative mortality in those transferred any distance was 22/68 (32%) with those transferred <100km 17/41(41%) and >100km 5/27(19%) (p= 0.048).
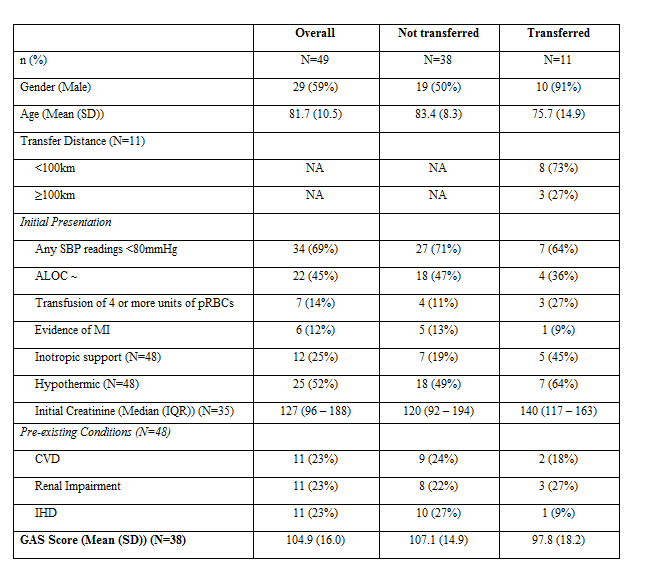
Those not offered surgical intervention were much older (mean age 81.7) and more likely to be female (41% vs 10%) (See table 8). They had higher proportions of pre-existing cerebrovascular disease (23% vs 10%) and renal impairment (23% vs 14%). No formal comparisons have been made from this group as the study did not capture patients from regional hospital who could have been transferred but were not. The possible reasons for not transferred include: surgery/transfer not requested by the regional hospital/patient/family, proceeding to surgical repair locally, or this institution’s vascular team advising that transfer appeared to be futile based on known clinical factors.
A negative disease status for either renal, cardiovascular or myocardial disease, was assigned across 17 patients (11%). The largest frequency of missing data was for initial creatinine levels, with 15 patients missing data and having no previous indication of renal impairment. Pre-existing conditions were also missing for two additional participants. GAS scores were not calculated for these 17 patients. Missing data was also encountered in the recording of post-operative complications for which approximately 10% had missing data. Sample sizes have been reported in tables for all variables where any frequencies of missing data was an issue. All missing data in this study is believed to be missing at random (MAR) as patients with missing data were distributed across all subgroups.
Patient transfer itself was not found to be associated with 30-Day mortality in those who underwent surgical intervention. However, if the patient is transferred from ≥100km away and proceeds to surgery, they appeared to have a lower 30-day mortality rate compared with other interhospital transfers. It’s possible that these patients have more physiological reserve as those transferred further displayed increased proportions of a marker of being critically unwell. This study supports the practice of offering interhospital transfer to patients who are referred from long distances (who are not obviously too frail or receiving CPR for example) with rAAA as they may have a favourable survival rate despite high rates of requiring massive transfusion and/or receiving inotropic support. These results may be influenced to some degree by an underlying data sampling bias, due to an unknown number of patients who were not transferred from peripheral institutions.
Presentations of rAAA associated with ALOC and/or requiring Inotropic/vasopressor support were associated with higher 30-day mortality rates. Both of these are indicative of shock, and reflect a higher GAS score. Further to this, in this study, those with higher GAS scores had higher mortality rates. Its use as an adjunctive scoring system is supported by this study, but it should not be relied solely as a decision-making tool given the range of other individual patient factors that are shown to be significant in this study including operative technique and interhospital transfer distance. Denying potentially lifesaving treatment to a patient because of a scoring system alone would be controversial, particularly given previous attempts to apply a cut-off value (i.e. a score of 84) would effectively deny life-saving treatment to a proportion of survivors (35%) who have a pre-operative score above that threshold19. Though that study did not specifically explain which method they used to calculate their cut-off value, we attempted our own investigation of optimal GAS score optimal cut-off value calculation and found that in this cohort a score of 95 could more accurately predict mortality, and promote the offering of interhospital transfer and possible surgery to a larger proportion of patients with rAAA. Neither are perfect on their own. The GAS may be useful, for example, in providing patients and their families with further specific information if the pursuit of non-operative/palliative measures were being considered and some operative mortality risk rates were being sought. The slightly higher “cut-off score” to help guide decision making with intervention suggested by the analysis in this study may reflect differences in how the scores were analysed (as mentioned above). Alternatively it could also reflect other improvements in care. Other institutions are encouraged to measure their recent outcomes using GAS as part of any audit of their surgical activity.
This study also showed a significant reduction in 30-day mortality for EVAR compared with Open repair for rAAA in patients who are deemed suitable candidates for this approach. Patients who underwent EVAR in this cohort, however, all underwent pre-operative CT-Angiography, indicating a degree of relative haemodynamic stability. Open Repair (rather than EVAR) was more commonly utilised in this study, and its ongoing use in rAAA is supported by the relatively superior 30-day mortality rate (37%) in this study when compared with other published rates for Open repair for rAAA from larger cohort studies1-2,6. The rates of EVAR for rAAA at this institution are increasing based on the analysis performed in this study and this may reflect firstly that this unit’s first hybrid theatre was opened near the start of this study 10 year period. Furthermore, the mix of the surgeons working within the unit included a range of individual surgeon preferences for modality of treatment of rAAA and decisions are based on individualised patient parameters on arrival. But over time there has been increased experience with EVAR as a modality of treatment in the rAAA setting.
There was a major limitation in this study in that patients who were not transferred were not captured. Open repair (rather than EVAR) and initial presentations including ALOC and/or Inotropic/vasopressor support were found to be strongly associated with 30-Day mortality. Open repair was by far the most common modality of surgical treatment, and still has its place in the treatment of this lethal condition. Shorter transfer distance appears to have an increased 30-day mortality risk in patients undergoing surgery, and this may reflect data sampling bias and/or could reflect a more robust group of patients who present with rAAA from a more distant location. Alternatively, it could represent an increased propensity to offer emergency surgery to critically unwell patients who had transferred relatively shorter distances. The data in this study supports the practice of offering selective transfer for potential treatment to patients with rAAA who are referred from distant (≥100km) locations, bearing in mind that the patients captured in this study are those who were referred to, accepted by, and successfully arrived at this institution.
A multicentre study of critically unwell patients with rAAA undergoing interhospital transfer in Australia would add value to defining the current logistical challenge this country faces. Any future study in this manner should include data from ambulance services, death certificates and regional centres to more accurately measure the incidence, prevalence, and effects of the illness and its treatment in different locations of Australia in order to better implement effective services to the community.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
