
Case Report | DOI: https://doi.org/10.31579/2690-4861/919
1 Department of Surgery, Uster Hospital, Switzerland.
2 Department of Orthopedics and Traumatology, Winterthur Cantonal Hospital, Switzerland.
3 Department of Orthopedics and Trauma Surgery, Schaffhausen Cantonal Hospital, Switzerland.
*Corresponding Author: Dimitrios Thodis, MD. Department of Surgical Disciplines, Department of Orthopedics, Uster Hospital, Brunnenstrasse, 42, 8610 Uster, Switzerland.
Citation: Dimitrios Thodis, Franziska Ziegenhain, Marco Di Lazzaro, Severin Meili, Michele Arigoni, (2025), Secondary Migration of the Lesser Trochanter after Surgical Treatment of a Trochanteric Fracture: A Case Report, International Journal of Clinical Case Reports and Reviews, 28(3); DOI:10.31579/2690-4861/919
Copyright: © 2025, Dimitrios Thodis. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 July 2025 | Accepted: 29 July 2025 | Published: 08 August 2025
Keywords: pertrochanteric fracture; intramedullary nail; lesser trochanter migration; revision surgery
Secondary displacement of the lesser trochanter into the groin after osteosynthesis of trochanteric fractures is not common and only scarcely described in the literature. Most reported cases are associated with neurovascular damage caused by the displaced fragment and lead to revision surgery with resection of the migrated fragment. However, revision surgery due only to persistent pain and impairment of mobility without neurovascular compromise is even less common.
We present the case of a 79-year-old female patient with a pertrochanteric fracture of the left proximal Femur (AO 31.A1.3) with a lesser trochanter fragment after a fall from her own height. She underwent closed reduction and intramedullary nailing with satisfactory intraoperative reduction and implant positioning. Initial postoperative radiographs showed a moderate proximal displacement of the lesser trochanter. The patient was mobilized with full weight bearing and enrolled in an early rehabilitation program. Five weeks postoperatively, she returned with acute immobilizing pain in the left hip. Imaging confirmed a complete proximal displacement of the lesser trochanter into the groin. Due to persistent, immobilising pain, she underwent surgical revision with resection of the lesser trochanter via a direct anterior approach. Postoperative recovery was uneventful, and the patient regained painless full weight-bearing mobility. The clinical benefit in our case was striking, highlighting the need to consider early revision surgery regardless of neurovascular involvement.
Pertrochanteric fractures of the femur are among the most frequent injuries in the elderly and are typically managed with intramedullary nailing [1]. The lesser trochanter is involved in approximately 50% of these fractures. While often considered clinically insignificant, displacement of the lesser trochanter can lead to complications and significant morbidity. Secondary migration of this fragment into the groin, though rare, has been reported to cause pain, neurovascular compression, and functional impairment. In the majority of documented cases, revision surgery was indicated due to neurovascular involvement. In contrast, cases of revision based solely on symptomatic pain are seldom described [2-6].
This report presents a rare case of symptomatic secondary migration of the lesser trochanter into the groin following intramedullary fixation of a pertrochanteric fracture. The patient experienced significant pain and impaired mobility without neurovascular compromise. Our aim is to highlight the clinical reasoning behind opting for revision surgery and to emphasize the importance of thorough postoperative monitoring, timely diagnosis and appropriate management.
A 79-year-old female with a history of osteoporosis was admitted to the emergency department after tripping and falling on her left hip. Radiographs confirmed a pertrochanteric fracture with a non-displaced concomitant lesser trochanter fracture (Figure. 1), classified as AO 31.A1.3, according to the AO fracture classification system. The patient underwent closed reduction and intramedullary nailing (TFN-ADVANCED™ Proximal Femoral Nailing System, Depuys Synthes). Intraoperative fluoroscopy confirmed good fracture reduction and optimal implant placement (Figure. 2).

Figure 1: Initial anteroposterior (a) and axial (b) radiographs, showing the pertrochanteric fracture and an anatomical position of the lesser trochanter (arrows).
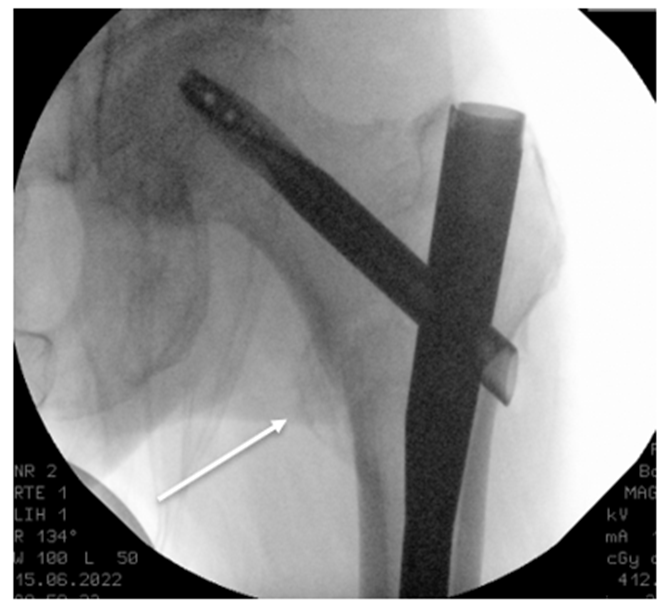
Figure 2: Intraoperative anteroposterior fluoroscopy imaging, showing a good reduction of the fracture without dislocation of the lesser trochanter (arrow).
Postoperatively, the patient was allowed full weight bearing and was enrolled in an early rehabilitation program in our geriatric department. Initial postoperative radiographs revealed a minor, clinically irrelevant, proximal displacement of the lesser trochanter (Figure. 3). Hospital stay
was uneventful and the patient was discharged after two weeks. However, five weeks postoperatively, she was readmitted because of acute onset of immobilizing pain in the left groin. Radiographs and CT imaging showed a migration of the lesser trochanter into the groin (Figure. 4 and 5).

Figure 3: Anteroposterior (a) and axial (b) radiographs 2 days postoperatively, showing the initial, asymptomatik proximal dislocation of the lesser trochanter (circle and arrow).

Figure 4: Anteroposterior (a) and axial (b) radiographs 5 weeks postoperatively, showing the further proximal dislocation of the lesser trochanter up to the groin (circle and arrow)

Figure 5: Axial CT-scan 5 weeks postoperatively showing the exact position of the dislocated lesser trochanter directly anterior to the femoral head (arrow), causing the immobilising inguinal pain.
The patient was admitted for pain treatment and mobilization. Due to persistent, immobilizing pain, she underwent surgical resection of the displaced lesser trochanter through a direct anterior approach. The fragment could be identified with the help of intraoperative fluoroscopy inside the rectus femoris muscle just anterior to the hip joint. Resection of the fragment from the retracted iliopsoas tendon was performed. Postoperative radiographs confirmed the complete resection of the lesser trochanter (Figure. 6). Further hospital stay was uneventful and the patient regained immediate full weight-bearing mobility without pain. The follow up for three months after the revision surgery showed a fully recovered and mobile patient. Especially the flexion of the hip was symmetrical in terms of range of motion and strength compared to the contralateral side. The further radiographs up to 2 years postoperatively showed also an uneventful fracture healing with an optimally positioned implant.
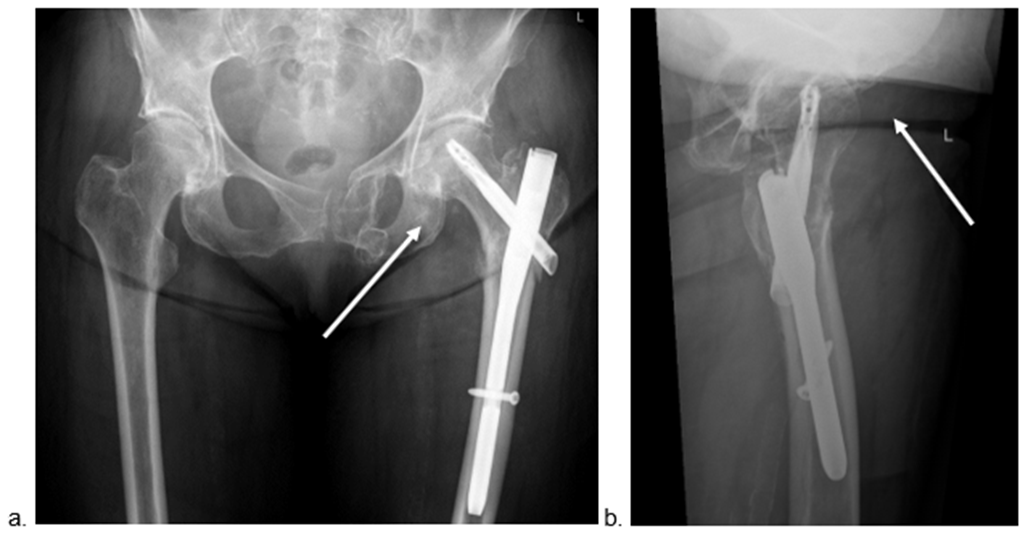
Figure 6: Anteroposterior (a) and axial (b) radiographs after the revision surgery with the resection of the lesser trochanter via a direct anterior approach (arrows indicate the absence of the lesser trochanter).
Lesser trochanter fractures associated with trochanteric fractures are common but there is no consensus in the indication for surgical fixation. While some authors showed a higher complication rate (implant failure, secondary fracture dislocation etc.) for bigger lesser trochanter fragments and displacement > 20 mm, there appears to be no functional difference one year after surgery when compared with trochanteric fracture without involvement of the lesser trochanter [11, 12]. Surgical management remains thus controversial. In our patient, no clear lesser trochanter fragment was visible on the initial radiograph at admission for the trochanteric fracture as well as in the intraoperative imaging and therefore no specific treatment was carried out.
Secondary migration of the lesser trochanter after trochanteric fracture is not well studied in the literature and there are only a few case reports of complications related to the fragment migration. In a review of case reports Altherr et al showed that secondary displacement of the lesser trochanter can lead to vascular (venous or arterial) and nerve injury. Surgical treatment combined with endovascular procedures was necessary in almost all the cases [5].
In our case migration of the lesser trochanter in the groin, lead to immobilizing pain without damage to any neurovascular structures. Surgical resection of the migrated fragment led to a complete remission of pain and restoration of mobility for the patient. The clinical benefit in our patient was striking, highlighting the need to consider revision surgery in symptomatic patients regardless of neurovascular involvement. To our knowledge only two similar cases have been described in the literature. One case was treated conservatively because of the reduced general condition of the patient while in the other case surgical removal of the migrated fragment showed an immediate recovery of the patient like with our case [5, 6].
Additionally, this case highlights the clinical importance of subtle fragment shifts that may be overlooked. Retrospectively, closer radiographic surveillance could have helped anticipate the complication. The striking clinical improvement after resection suggests that persistent groin pain, even without radiographic progression or neurovascular signs, may warrant consideration for revision surgery. It is therefore necessary to thoroughly investigate patients with persistent pain after surgical treatment of trochanteric fractures. Regular radiographs in the early follow up as well as advanced imaging such as CT scans or MRI allow detection of early secondary displacement of the lesser trochanter and prevent complications.
To date only two biomechanical studies and one systematic review has specifically addressed the fixation of the lesser trochanter at the time of initial surgical management, underscoring the limited evidence available to guide clinical decision-making in cases of secondary migration of this fragment [9,10,11].
The importance of patient selection for surgical intervention cannot be overstated. In cases where the fragment remains stable and asymptomatic, conservative treatment remains a viable option. However, in symptomatic cases, especially when pain or functional limitation persists, surgical intervention should be promptly considered to prevent prolonged morbidity and delayed rehabilitation.
Further studies are needed to better understand the fate of lesser trochanter fragments in the treatment of trochanteric fractures. Currently, there is a lack of data on how frequently secondary displaced lesser trochanter fragments migrate into the groin, making it difficult to assess the true incidence and clinical relevance of this complication [7,8,12]. Establishing such epidemiological data would help guide the decision-making process.
In addition, in patients who show initial postoperative displacement of the lesser trochanter fragment, it may be reasonable to consider closer or more frequent radiologic follow-up to detect early signs of migration before symptoms develop. This approach could allow for earlier intervention in selected cases.
Moreover, studies are needed to establish clear and evidence-based criteria for when a migrated lesser trochanter should be surgically treated. At present, the threshold for surgical revision remains subjective, often based on symptom severity rather than standardized indicators. Identifying how many patients truly benefit from fragment resection would help define treatment guidelines.
Finally, individualized rehabilitation protocols, particularly those that modulate early iliopsoas loading, might reduce the risk of fragment migration and improve functional outcomes.
This case report is inherently limited by its single-patient design. No objective functional outcomes were systematically measured, and the applicability of our findings to a broader patient population is limited. Moreover, the decision for revision surgery was based on clinical judgment and radiographic findings rather than on standardized treatment criteria. Nevertheless, the surgical approach we employed, an anatomically guided, minimally invasive anterior technique, is both safe and effective. Because of its protective trajectory through intermuscular planes, this approach minimized trauma to surrounding soft tissues and avoided neurovascular structures. As a result, the patient experienced a rapid and uneventful postoperative recovery, regaining full weight-bearing mobility within a short period.
Symptomatic lesser trochanter displacement, especially progressive migration following intramedullary nailing of pertrochanteric fractures is a rare but significant complication. Surgical resection is a good option in symptomatic cases with persistent pain. In such cases revision surgery should be considered, whether or not there is neurovascular involvement. This case emphasizes the importance of recognizing this complication and considering surgical intervention when conservative management fails.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
