
Research Article | DOI: https://doi.org/10.31579/jsrbi.2021/004
1 Endocrinologist at the Regional Hospital "Omer Nishani", Gjirokastra
2 Laboratory Physician, Department of Nursing, University "Eqrem Cabej" Gjirokastra
3 Family Doctor, Head of Emergency Service of the Regional Hospital "Omer Nishani", Gjirokastra
*Corresponding Author: Altin Goxharaj, Altin Goxharaj, Laboratory Physician, Department of Nursing, University
Citation: Hodo Celo, Altin Goxharaj, Bledi Celo, (2021) Screening test for Hashimoto's thyroiditis and hypothyroidism (Screening results). J. Scientific Research and Biomedical Informatics, 2(1); Doi:10.31579/jsrbi.2021/004
Copyright: © 2021 Altin Goxharaj, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 December 2020 | Accepted: 24 January 2021 | Published: 04 February 2021
Keywords: thyroiditis; echo; laboratory
Disorders of thyroid function are a common problem found in the daily work of family physicians and various specialists. Thyroid function is quite important in a number of organs and systems. Early, prompt recognition and diagnosis of these concerns would contribute to the correct and professional treatment of cases, would prevent the installation of hypothyroidism. The role of the family doctor takes great advantage as the first and most frequent contact is the most. The physician is also often faced with the dilemma of what would be the best cost-effectiveness diagnostic route before these cases? Is the clinic enough? Is imaging alone enough? Is the Laboratory Alone Enough?
Considering the role and function of the thyroid, the reflection of the consequences of its dysfunction in a large number of systems and organs, interdependence and cooperation with a wide range of specialties, here we present the results of screening work towards Hashimoto's disease and its aftermath. Thanks to hypothyroidism.
Methodology
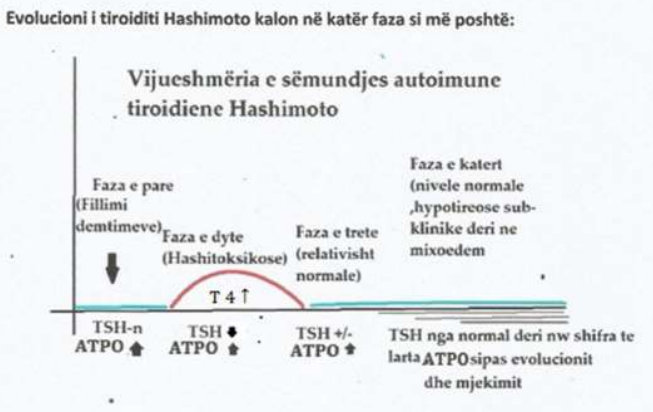
Screening methodology and results and reasons for selecting ultrasound for this screening (in the absence of a rapid test, acceptable cost and maximum accuracy).To make the screening we must consider the clinical stages of Hashimoto's thyroiditis which we are presenting in the table below;
The first stage is the initial stage of lymphocytic infiltration and thyroid cell damage,
Second stage - Hashitoxicosis where we have temporary hyperthyroidism, where after tissue damage an amount of hormone is released into the blood that gives these signs of hyperthyroidism.
The third stage is a "normal" stage where discarded thyroxine continues to be consumed.
The fourth stage part normalizes, part has a "cure" that can be activated, so these cases are kept under observation. Another part passes into sub-clinical and clinical hypothyroidism.
Based on the OMS criteria, from 2008 onwards we practically analyzed the methods which one we should use for spontaneous or continuous screening of Hashimoto's thyroiditis.
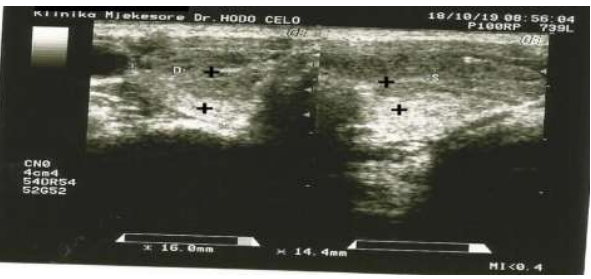
For screening in the absence of a rapid and low-cost test, also to enable the detection of most rates with Hashimoto's and hypothyroidism, we have selected ultrasound examination in search of hypoechoic areas — hypoechgenoic pseudonodes and stretch marks. With ultrasound we noticed that through pseudonodes we identify most of the cases affected by autoimmune thyroiditis as those with autoimmune activity (presence of antibodies), those that have returned to normal function, those "cured" and cases that have evolved towards hypothyroidism. By determining TSH we would only detect cases of hypothyroidism, and hyperthyroidism, so the rest would not be detected.
By determining anti-ATPO we would detect only cases with autoimmune activity, as well as by determining anti-Tg, EBV-IgG, EBV-IgM, etc. by defining which we identify a very small part of the cases, i.e. not helping us for mass screening.
With the determination of immunoglobulins not only by cost but the spectrum captured is very narrow and that does not help for mass screening.
Ultrasound not only identifies a large number of patients who have Hashimoto's thyroiditis but well identifies its early stages which is important for any screening.
Ultrasound poses no physical or psychological risks
Given the workload that imaginers currently have from a workload, unplanned with the number of patients, they are described quickly and without the details needed by the internist and endocrinologist, and it has been observed that pseudodonts are referred to as nodules, removing the possibility of Hashimoto pseudonodes and thyroiditis. To avoid this we would highlight two moments:
1-On the recommendation sheet for the imager to write: "To be seen and for pseudonode"
2-When it is possible to be sent to a licensed endocrinologist after qualification in the relevant course for ultrasound.
The cost of ultrasound is also lower than the other tests mentioned above, and the benefits are great because the disease is detected either in the early stages or in the late or cured ones and is put on medication improving the quality of life.
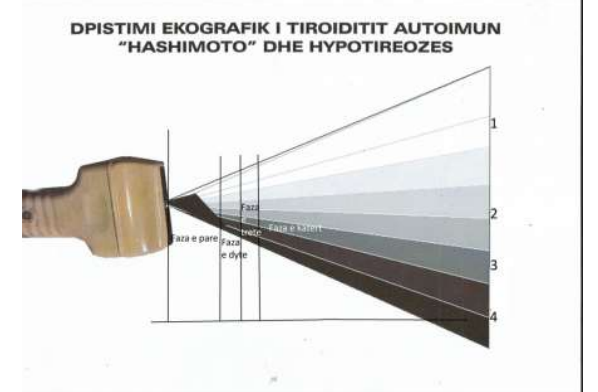
This figure shows the stages of Hashimoto's thyroiditis with ultrasound examination from the first stage, the second stage (hashitoxicosis), the third stage where we have gradual consumption of the hormone that is shed in the blood from necrotic areas of the thyroid and then the fourth stage evolution of lesions and reduction of thyroid function where:
1-A portion of Hashimoto's thyroiditis passes without sequelae (upper white area);
2-Below the light gray area, cases "cured" with a defect that may not currently have laboratory changes for hypothyroidism, or for increased anti-ATPO, EBV-IgG, EBV-IgM. Subclinical hypothyroidism may be common in this area and may progress to hypothyroidism each year.
3-The most pronounced cases (dark gray) where thyroid lesions are more advanced and subclinical and clinically manifested thyroiditis are found, are those cases that should be placed in therapy according to the case
4-Finally the black area where the cases with clinical hypothyroidism enter up to severe cases of mixoedema
On the spectrum of Hashimoto's autoimmune thyroid stages with ultrasound can be identified:
Micropseudonode;

From those with normal thyroid function to those that show functional changes. Although a part of the cases do not have clinical and laboratory signs for thyroid or hypothyroidism, they are recorded in the records, and are kept as cases to be re-checked year after year with endocrinologist consultations, echography and, as the case may be, laboratory examinations. The purpose of these periodic checkups is to detect the recurrence of autoimmune activity or the onset of hypothyroidism as early as possible (although in microseudonodes these are very rare).
Large Hypoechogenic areas;

In this case we define one or both thyroid lobes, cases which are more advanced for compromising thyroid function, anti-TPO, anti-Tg, (IgG, IM) EBV, changes in TSH and T4 levels, but even with normal laboratory data. Cases with normal laboratory data will be kept under observation year after year to look for the possibility of deterioration, increased autoimmune activity, transition to hypothyroidism, and the appearance of other hypoecogenic plasdars. Depending on the case, they consult with the endocrinologist and other specialists whose field is disturbed (eg gynecology in menstrual disorders or infertility, etc.). In these cases we should pay attention to the reduction of functional thyroid tissue and the reduction of the thyroid gland towards an atrophic thyroiditis.
Pseudonodet multiple hypoechogenic;

Hyperechogenic pseudonodes have generally been encountered rarely and associated with hypoechoic pseudonodes, Strias have been encountered frequently especially in cases where hypothyroidism is found.
At the end of this spectrum where it is dominated by hypothyroidism we encounter small, atrophic thyroid.

This ultrasound examination is done for cases that after the interview (anamnesis) present data, cases that have data on the card for various thyroid diseases, cases with autoimmune diseases, cases with type 1 diabetes, cases suspected by specialists, can also It is also used for screening in groups, for example, students, employees, etc. in search of thyroiditis and hypothyroidism.
The cases that we have identified pseudonodes are subjected to laboratory examinations initially T4, TSH, anti-TPO, when the latter is normal we can ask for anti-Tg, and EBV-IgG, EBV-IgM, even cases that need to be differentiated with other diseases such as thyroid carcinoma continue with biopsy puncture. Verified cases that have a high antibody titer are placed in diet and medication.
For “cured” cases, follow-up is recommended year after year and in special situations such as pregnancy, post-partum, puberty, pre-climax, climax and the elderly, hypercholesterolemia, etc.
Conclusion; from our experience we think that combining the good anamnesis with the selection of ultrasonographic examination (echo) as the first complementary examination, we consider that cost-effectiveness, the examination is comfortable and full of , we suggest to find application in future protocols.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
