
Research Article | DOI: https://doi.org/10.31579/2641-0419/417
1Heart and Brain Center of Clinical Excellence, Pleven, Bulgaria.
2Bulgarian Cardiac Institute.
3Medical University, Pleven, Bulgaria.
4Heart and Brain, Burgas, Bulgaria.
5Specialized hospital for active cardiology treatment, Varna, Bulgaria.
*Corresponding Author: А. Ivanova, Heart and Brain Center of Clinical Excellence, Pleven, Bulgaria.
Citation: А. Ivanova, I. Simova, Т. Vekov, V. Коrnovski, J. Кrasnaliev, (2025), Use of Streptokinase for intravenous thrombolysis in pulmonary embolism: Practice and results (Data from the pulmonary embolism registry of Bogodogo University Hospital Center in Burkina Faso (PER/UHC Bogodogo-BF), J Clinical Cardiology and Cardiovascular Interventions, 8(2); DOI: 10.31579/2641-0419/417
Copyright: © 2025, А. Ivanova. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 January 2025 | Accepted: 29 January 2025 | Published: 06 February 2025
Keywords: familial hypercholesterolemia; artificial intelligence; statinе; ezetimibe; PCSK9 inhibitors; xanthomas; corneal arcus
Introduction: Familial hypercholesterolemia (FH) is an autosomal dominant genetic manifestation with early, aggressive, and recurrent cardiovascular events. According to literature data, this is seen in one in 200 individuals in the general population and is interpreted as the most common hereditary cardiovascular disease. Following the current trends in modern medicine, we used the artificial intelligence (AI) method to achieve greater efficiency in the recognition of FH patients.
Objective: Our primary goal was to create, with the help of AI, an algorithm for FH screening in patients, admitted to the Clinics of the Bulgarian Cardiac Institute. A secondary task was to optimize the therapy of patients, according to the latest recommendations for behavior in dyslipidemias of the European Society of Cardiology.
Methods: For a period of one year, we conducted a prospective study in which all hospitalized patients for any atherosclerotic event requiring treatment were followed in three hospitals in Bulgaria - Pleven, Burgas and Varna, covering Cardiology, Cardiac Surgery, Neurology and Vascular Surgery clinics. The electronic records were stored in the hospital's Gamma Cod Master (GCM) program. The algorithm for patient inclusion and data collection uses AI, through which, according to set parameters, patients are selected according to age, diagnosis, LDL-C value, type, and dose of antilipemic therapy. Each indicator gives certain points that are summed up. For each patient with a final score of ≥4, an alarm signal is created in the GSM, which can be easily seen by the attending physician. Despite AI, the main task is the attending physician to check the accuracy of the integrated data, to specify the physical status for the presence of stigmata such as xanthomas and corneal arcus at an early age, to collect additional family history for early atherosclerosis, to additionally recalculate the points of the DLCN score, and to optimize the therapy according to the recommendations of the European Society of Cardiology for dyslipidemias.
Results: We prospectively followed 438 patients signaled by AI. The largest number of electronic files were analyzed in the cardiology clinics, with the most patients being screened for FH in the Cardiology Clinic in Pleven – 174, of which 79 patients (46%) had probable FH. In 49% of the total number of patients (438), we found a family history of an early atherosclerotic event, and 32% of the patients had a previous cardiovascular event. Only 1.5% of those hospitalized were on combined statin and ezetimibe therapy, and 15% of the total number of patients were completely missing lipid- lowering therapy. Through AI, patient therapy was optimized, also increasing the number of PCSK9 inhibitor prescriptions 3-to 4.5-fold (depending on the region).
Conclusion: The development, implementation and use of AI for FH screening is possible and easily applicable. Despite the use of AI, many FH patients remain undiagnosed. This confirms the need for active participation of the attending physician, whose role in correct diagnosis and treatment, as well as in improving the patient's prognosis, remains leading.
Familial hypercholesterolemia (FH) is an autosomal-dominant genetic disease associated with early, aggressive and recurrent atherosclerotic cardiovascular events. It is caused by an allelic mutation in a gene responsible for lipid metabolism, which is associated with persistence of high levels of low-density lipoprotein (LDL-C). According to literature data, the disease is observed in one in 200 individuals in the general population and is interpreted as the most common hereditary cardiovascular disease (1,2,3).
FH has two forms: homozygous and heterozygous, the latter being widespread and having one mutated allele in the following genes: LDLR, ApoB, PCSK9, or LDLRAP1 (1, 4, 8). In the homozygous form of FH, carriers have two pathogenic mutations (homozygotes, i.e. with two identical mutations or compound heterozygotes, i.e. with different mutations). The condition of homozygous FH is very rare (1:160,000 to 1:250,000) and results in a high incidence of acute myocardial infarction (AMI) or other atherosclerotic events in childhood or adolescence (1).
Patients suspected of having genetic dyslipidemia can be recognized by extremely high LDL-C levels, which correlate with a family history of premature atherosclerotic cardiovascular disease (3, 4).
According to the latest recommendations of the European Society of Cardiology (ESC) for dyslipidemias (5, 6), LDL-C target values, in very high and high-risk individuals, should be <1>
| Treatment | Average reduction of LDL-C |
| Statinе with a moderate intensity | ~30 % |
| Statinе withhigh intensity | ~50 % |
| Statinе withhigh intensity + ezetimibe | ~65 % |
| PCSK9 inhibitors | ~60 % |
| PCSK9 inhibitors + statin withhigh intensity | ~75 % |
| PCSK9 inhibitors + statin with high intensity + ezetimibe | ~85% |
Table 1: Expected reduction of LDL-C, with combined therapies:
2021 ESC Guidelines on cardiovascular disease prevention in clinical practice
Despite the well-known behavior algorithm for hypercholesterolemia, the lipid profile is often underestimated by clinicians and not correctly interpreted according to the patient's risk profile. Assessment of physical status for the presence of xanthomas, arcus corneal, and xanthelasma should be a guiding criterion and presumptive factor for FH (Figs. 1, 2, 3).
Components of the diagnosis: Identification of patients with FH is a multifaceted process, including family history of dyslipidemia and early cardiovascular events, physical status stigmata: tendon xanthomas, corneal arcus, manifestation of early atherosclerotic cardiovascular disease, LDL-C values, as well as genetic testing. In recent years, Lipoprotein(a) – for short Lp (a), called the “genetic” lipoprotein, has also found informative value and significance (4, 5, 7).
In the process of determining the causes of hypercholesterolemia, other conditions associated with elevated LDL-C levels, such as thyroid disease, cholelithiasis, kidney disease, hyperglycemia, and hyperalbuminemia, must be excluded (8, 9).
Use of imaging methods for early identification of cardiovascular disease such as 12-lead electrocardiogram, echocardiography, computed tomography angiography scan, selective coronary angiography with intravascular ultrasound (IVUS) and Fractional Flow Reserve (FFR) would also benefit and support the diagnosis (figure 3).
A diagnosis of FH can be made by genetic testing, which is rarely applied in practice, and/or by using the readily available criteria of the Dutch Lipid Clinical Network (DLCN) score (Table 2)
| Category | Characteristic marks | Points |
| Family history | First-degree relatives with known early coronary and/orvascular disease (males<55> First-degree relatives with tendinous xanthomas and/orpresence of cornealarcus, or children aged <18> | 1
2 |
| Clinical history | Patients withearly coronary disease, (men <55> | 2 |
| Patients with early cerebrovascular or peripheral vascular disease (men <55> | 1 | |
| Physical examination | Tendinous xanthomata Corneal arcus before 45 years of age | 6 4 |
| Levels of LDL-C | >8.5 mmol/l 6.5-8.4 mmol/l 5.0-6.4 mmol/l 4.0-4.9 | 8 5 3 1 |
| Genetic analysis | Functional mutations in the genes of LDL-R, APOB, PCSK9 | 8 |
| Genetic analysis | Functional mutations in the genesof LDL-R, APOB, PCSK9 | 8 |
Table 2: Criteria for the diagnosis of Heterozygous FH, according to the Dutch Lipid Clinical Network.
Dutch Lipid Clinic Network criteria for Familial Hypercholesterolemia (FH) Last edited 26 Jan 2018. Last reviewed 28 Nov 2023 <3>8 points: definite FH
According to national registries, Bulgaria is among the countries with the highest number of cardiovascular diseases. Many patients do not suspect that they have FH, and in most cases the disease is discovered after the realization of an acute vascular accident (acute myocardial infarction or stroke at a young age, men <55>

Figure 1: Xanthomas on a 47-year-old patient with newly diagnosed three-vessel coronary disease and newly established hypercholesterolemia. Upon admission to the Pleven "Heart and Brain" Hospital with LDL 8 mmol/l, total cholesterol 9.7 mmol/l, emergency cardiac surgical treatment was performed due to unstable angina pectoris. The family history of early ischemic heart disease.Personal archive, the patient has given consent to publish the material.

Figure 2: Xanthelasma of a 46-year-old patient treated at MBAL "Heart and Brain" Pleven with established hypercholesterolemia, multivessel coronary artery disease, in which aorto-coronary bypass was performed. LDL-C 6 mmol/l, total cholesterol 12 mmol/l at diagnosis, untreated until hospitalization for acute coronary syndrome. Family history: Father died at the age of 47 from acute myocardial infarction, sister with severe dyslipidemia. Personal archive, the patient has given consent to publish the material

Figure 3: Arcus corneal and xanthelasma in a 54-year-old patient hospitalized for a second time with myocardial infarction. First vascular accident of a 50-year-old age. With chronic arterial occlusive disease of the lower extremities. Ineffectively treated dyslipidemia, LDL-C 3.9 mmol/l upon admission against the background of rosuvastatin 10 mg/per day. Personal archive, photo provided for publication with patient consent.
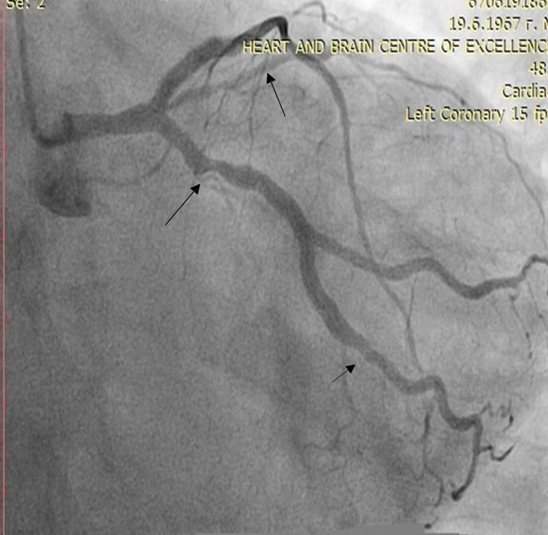
Figure 4: Selective coronary angiography of a 55-year-old woman with established ischemic heart disease, LDL 4 mmol/l, total cholesterol 6 mmol/l, on therapy with rosuvastatin 20 mg/per day. and ezetemibe 10 mg/per day, in which we started treatment with a PCSK9 inhibitor.
For a period of one year, we conducted a prospective study, including all patients (men < 65>
The analysis used data from electronic records of patients treated in a specialized cardiology hospital in Varna and two large multi-specialty hospitals in Pleven and Burgas, where departments of Cardiology, Cardiac Surgery, Neurology and Vascular Surgery were covered. Electronic records were stored and generated using the hospital's Gamma Cod Master (GCM) program.
The follow-up period was one year, starting in the month of July 2021 and ending in July 2022. The algorithm for patient inclusion and data collection uses AI and runs in the following sequence:
I. Patients under 65 years of age for men and under 70 years of age for women are selected.
II.Distribution of points according to diagnosis
a.Each patient with any of the following diagnoses receives 2 points
I20.0 Unstable angina pectoris
I20.1 Angina with documented spasm I20.8 Other types of anginas
I20.9 Angina, unspecified
I21.0 Acute anterior wall transmural myocardial infarction I21.1 Acute transmural myocardial infarction of inferior wall
I21.2 Acute transmural myocardial infarction with other specified locations I21.3 Acute transmural myocardial infarction of unspecified location
I21.4 Acute subendocardial myocardial infarction I21.9 Acute myocardial infarction, unspecified I22.0 Recurrent anterior wall myocardial infarction I22.1 Recurrent inferior wall myocardial infarction
I22.8 Recurrent myocardial infarction with other specified location I22.9 Recurrent myocardial infarction of unspecified location
I23.0 Hemopericardium as an ongoing complication of acute myocardial infarction I23.1 Interatrial defect as an ongoing complication of acute myocardial infarction
I23.2 Interventricular defect as an ongoing complication of acute myocardial infarction
I23.3 Rupture of the heart wall without hemopericardium as an ongoing complication of acute myocardial infarction
I23.4 Rupture of tendon chord as an ongoing complication of acute myocardial infarction
I23.5 Papillary muscle rupture as an ongoing complication of acute myocardial infarction
I23.6 Atrial, atrial auricle, or chamber thrombosis as an ongoing complication of acute myocardial infarction
I23.8 Other ongoing complications of acute myocardial infarction I24.0 Coronary thrombosis not leading to myocardial infarction I24.1 Dressler syndrome.
I24.8 Other forms of acute ischemic heart disease I24.9 Acute ischemic heart disease, unspecified
I25.0 Atherosclerotic cardiovascular disease - described as such I25.1 Atherosclerotic heart disease.
I25.2 Old myocardial infarction I25.3 Cardiac aneurysm
I25.4 Coronary artery aneurysm I25.5 Ischemic cardiomyopathy
I25.6 Asymptomatic myocardial ischemia
I25.8 Other forms of chronic ischemic heart disease I25.9 Chronic ischemic heart disease, unspecified
b.Each patient with your diagnosis receives 1 of the following points: I63.0 Cerebral infarction caused by thrombosis of precerebral arteries I63.1 Cerebral infarction caused by embolism of precerebral arteries.
I63.2 Cerebral infarction caused by unspecified occlusion or stenosis of precerebral arteries.
I63.3 Cerebral infarction caused by thrombosis of cerebral arteries I63.4 Cerebral infarction caused by embolism of cerebral arteries.
I63.5 Cerebral infarction caused by unspecified occlusion or stenosis of cerebral arteries.
I63.6 Cerebral infarction caused by cerebral vein thrombosis - non-pyogenic I63.8 Another cerebral infarction.
I63.9 Cerebral infarction, unspecified
I65.0 Occlusion and stenosis of vertebral artery I65.1 Occlusion and stenosis of basilar artery I65.2 Occlusion and stenosis of carotid artery
I65.3 Occlusion and stenosis of multiple and bilateral precerebral arteries
I65.8 Occlusion and stenosis of other precerebral arteries
I65.9 Occlusion and stenosis of unspecified precerebral artery I66.0 Occlusion and stenosis of middle cerebral artery
I66.1 Occlusion and stenosis of anterior cerebral artery I66.2 Posterior cerebral artery occlusion and stenosis I66.3 Occlusion and stenosis of cerebellar arteries
I66.4 Occlusion and stenosis of multiple and bilateral cerebral arteries I66.8 Occlusion and stenosis of another cerebral artery
I66.9 Occlusion and stenosis of unspecified cerebral artery I67.0 Dissection of cerebral arteries without rupture
I67.1 Unruptured cerebral aneurysm I67.2 Cerebral atherosclerosis
I69.3 Sequelae of cerebral infarction
I69.4 Sequelae of stroke, unspecified as cerebral hemorrhage or infarction I69.8 Sequelae of other and unspecified cerebrovascular diseases
I70.0 Atherosclerosis of aorta
I70.1 Atherosclerosis of renal artery
I70.2 Atherosclerosis of arteries of extremities I70.8 Atherosclerosis of other arteries
I70.9 Generalized and unspecified atherosclerosis I74.0 Embolism and thrombosis of abdominal aorta
I74.1 Embolism and thrombosis of other and unspecified parts of aorta I74.2 Embolism and thrombosis of arteries of upper extremities
I74.3 Embolism and thrombosis of arteries of lower extremities
I74.4 Embolism and thrombosis of arteries of extremities, unspecified I74.5 Embolism and thrombosis of iliac artery
I74.8 Embolism and thrombosis of other arteries I74.9 Embolism and thrombosis of unspecified artery Z95.1 Presence of aortic coronary shunt graft
Z95.5 Presence of coronary angioplasty implant and graft
Z95.8 Presence of other cardiac and vascular implants and transplants
Note: according to category II a patient can receive either 1 or 2 points. Consider the higher points. The maximum number of points in this category is 2.
III.Distribution of points according to LDL cholesterol
a.The LDL cholesterol value on admission is obtained
b.It is determined whether this value is achieved on the background of statin therapy and at what dose
For this purpose, in the History section, all possible trade names of statins (according to the attached list) are searched for, creating an 80% margin of coincidence with the correct spelling (due to the frequently observed cases of incorrect spelling). In addition, we made it possible to write the name of the statin in both Cyrillic and Latin letters. When a statin is detected in therapy from the anamnesis, the dose in which it was administered is extracted (in the absence of a specified dose, a dose of 10 mg is taken).
c.The trade name of the statin is transferred to the corresponding generic.
The value of LDL-C is recalculated by multiplying by a corresponding coefficient, according to the type and dose of statin taken - see table 3.
The recalculation is done at a certain point in time, i.e. if the patient is hospitalized several times, the algorithm is triggered for each of them. Usually, the values of LDL- C and antilipemic therapy at each hospitalization differ, but the recalculated LDL-C remains approximately the same. If there is a difference with the total number of points, it is usually due to the entry of a new diagnosis in the patient's medical record.
| Antilipemic drug | Coefficient of correction |
| Atorvastatin 10 mg | 1.618123 |
| Atorvastatin 20 mg | 1.763668 |
| Atorvastatin 40 mg | 1.937984 |
| Atorvastatin 80 mg | 2.150538 |
| Rosuvastatin 5 mg | 1.709402 |
| Rosuvastatin 10 mg | 1.872659 |
| Rosuvastatin 20 mg | 2.070393 |
| Rosuvastatin 40 mg | 2.314815 |
| Rosuvastatin 80 mg | 2.624672 |
| Simvastatin 10 mg | 1.37741 |
| Simvastatin 20mg | 1.492537 |
| Simvastatin 40 mg | 1.636661 |
| Simvastatin 80 mg | 1.818182 |
| Ezetimibe 10 mg | 1.236094 |
| Ezetimibe/Simvastatin 10/10 mg | 1.855288 |
| Ezetimibe/Simvastatin 10/20 mg | 2.008032 |
| Ezetimibe/Simvastatin 10/40 mg | 2.252252 |
| Ezetimibe/Simvastatin 10/80 mg | 2.463054 |
| Ezetimibe/Atorvastatin 10/10 mg | 2 |
| Ezetimibe/Atorvastatin 10/20 mg | 2.173913 |
| Ezetimibe/Atorvastatin 10/40 mg | 2.173913 |
| Ezetimibe/Atorvastatin 10/80 mg | 2.5 |
| Ezetimibe/Rosuvastatin 10/10 mg | 2.48139 |
| Ezetimibe/Rosuvastatin 10/20 mg | 2.739726 |
| Ezetimibe/Rosuvastatin 10/40 mg | 3.333333 |
| Pravastatin 10 mg | 1.251564 |
| Pravastatin 20 mg | 1.322751 |
| Pravastatin 40 mg | 1.422475 |
| Others | 1.43 |
Table 3: Coefficient of correction, according to the type and dose of statin
d.The value of LDL cholesterol thus obtained is transferred into a number of points, according to table 4:
| LDL cholesterol (mmol/l) | Points |
| ≥ 8.5 | 8 |
| 6.5 – 8.4 | 5 |
| 5.0 – 6.4 | 3 |
| 4.0 – 4.9 | 1 |
Table 4. Values of LDL cholesterol, transferred into number of points
III. The points of categories II and III are added together and the final number of points is obtained.
IV. For each patient with a cut-off score ≥4, an alarm / output signal is created in the GCM to be easily visible to the attending physician.
Our chosen signaling method is the coloring of the at-risk patient, visible to the medical staff with access to the relevant ward, after the signaling has been activated.
Despite the help of AI, the main task remains for the attending physician to check the accuracy of the integrated data and whether the manifestation of the cardiovascular disease is early, to supplement the information with the data of the physical status in view of the presence or absence of xanthomas and corneal arcus of early age, collect additional family information for early atherosclerosis, further recalculate the DLCN score, and optimize therapy according to the recommendations of the European Society of Cardiology.
Statistical analysis: Statistical analysis was performed using SPSS for Windows version 19.0 statistical software. Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were presented as a percentage. The DLCN score was used to calculate the probability of FH.
Demographic and clinical characteristics of patients were analyzed through electronic records stored in GCM.
Ethical considerations: The clinical trial protocol was reviewed and approved by the local ethics committee. All research procedures adhere to the principles of the Declaration of Helsinki. Consent for FH treatment and personal data collection and analysis was obtained from all patients.
Results: 438 patients hospitalized and treated for any atherosclerotic indication were screened for FH. The prospective study continued from July 2021 to July 2022 and was conducted in seven department in three hospitals of the Bulgarian Cardiac Institute - two multi-specialty hospitals, including cardiology, cardiac surgery, neurology and vascular surgery clinics and one specialized cardiology hospital from three major cities in Bulgaria - Pleven, Varna, Burgas with a large patient flow.
Our primary outcome is to use AI to detect and analyses patients with probable and definite FH. Secondary objectives were to optimize the therapy of patients with DLCN ≥6 points, according to ESC dyslipidemia guideline from 2019 and to demonstrate whether the AI method would improve early recognition of patients with suspected FH.
Of the 438 patients signaled by AI, the largest number of electronic files was analyzed in the Cardiology Clinic of "Heart and Brain", Pleven (174), followed by 149 patients in the Cardiology Clinic in Varna (table 5).
From 174 patients detected by AI in the Cardiology Clinic of "Heart and Brain"- Pleven, the average value of AI points was 6.21 (standard deviation - SD ± 1.59). Of the total number of patients detected by AI, an individually physician-calculated DLCN score in 153 patients. These patients for risk profile, sequence of atherosclerotic disease, family history for early cardiovascular events, physical status with targeted follow-up for presence of corneal arcus and xanthomas. A DLCN score ≥6 points were found in 79 patients (46%), i.e., probable FH. In all hospitalized patients, the therapy was optimized according to the latest recommendations for the treatment of hypercholesterolemia (ESC 2019), in 78 patients (45%) PCSK9 inhibitor was added to the standard therapy with a maximum tolerated dose of statin, with or without ezetimibe.
In the same hospital, in the Department of Cardiac Surgery, the AI-assisted FH algorithm flagged 59 patients with a mean score of 6.37 (SD 1.79), of which 44% (26 patients) had an individual DLCN
score calculated by the attending physician ≥ 6 points, and treatment with monoclonal antibodies was started in 10 patients (17%).
The smallest number of patients were recognized in the Clinic for Vascular Surgery (3), and two of them were suspected of possible FH and the therapy was optimized to reach target LDL-C values according to the profile of the specific patients.
At the Neurology Clinic of "Heart and Brain", Pleven, AI has not reported any patients. Our explanation was for a non-routine study of a lipid profile in hospitalized patients in this department.
In SHAT of Cardiology, Varna, from 149 patients signaled by AI as potential for FH, the system gave an average value of 6.25 points (SD 1.77), of which DLCN score was calculated by the attending physician in 50 patients, 22 patients (14%) were assessed as possible FH, and in 9 patients (6%) an PCSK9-inhibitor was added.
For "Heart and Brain" Medical Center, Burgas, despite the small number of patients in total for the Clinic of Cardiology and Cardiac Surgery (53), a score for FH was calculated by the attending physician for 50 patients, with 23 of them having possible FH (43%), in 21 patients (40%) a PCSK9-inhibitor was added, indicating a good working algorithm and follow-up by the attending physician.
For the previous year without an AI for Pleven region, twenty patients received treatment with a PCSK9 inhibitor, and compared to ninety patients after the screening program was started. For 2019 without the use of AI for the hospitals involved in Burgas and Varna, only ten patients received treatment for FH with the administration of a monoclonal antibody, compared to thirty patients after the program was started (Table 5).
| Clinic | Number of patients, signaled by AI | Number of points by AI (average value ± SD) | Actual number of patients with DLCN score calculated by physician | Patients with probable FH- number (%) | Patients with PCSK9 inhibitor included - number(%) |
| Clinic of Cardiology „Heart and Brain“, Pleven | 174 | 6,21 (1,59) | 153 | 79 (46%) | 78 (45%) |
Cardiac surgery “Heartand Brain“, Pleven | 59 | 6,37 (1,79) | 26 | 26 (44%) | 10 (17%) |
| Clinic of Vascular Surgery „Heart and Brain“, Pleven | 3 | 5,33 (1,15) | 3 | 2 (66%) | 2 (66%) |
| Clinic of Neurology „Heart and Brain“,Pleven | 0 | 0 | 0 | 0 | 0 |
| Clinic of Cardiology and Cardiac surgery,Heart and Brain“,Burgas | 53 | 6,5 (2,01) | 50 | 23 (43%) | 21 (40%) |
| SHAT of Cardiology-Varna | 149 | 6,25 (1,77) | 50 | 22 (14%) | 9 (6%) |
| Total | 438 | 6,13 | 282 (64%) | 152 (35%) | 120 (28%) |
Table 5. Potential patients for FH in Clinics of the Bulgarian Cardiac Institute for a period of 12 months.
Legend: SD-standard deviation, AI-artificial intelligence, PCSK9-inhibitor (proprotein convertase subtilisin- kexin type 9 inhibitor).
Regarding the demographic characteristics (table 6), most of the patients recognized by AI were male – 310 patients (71%)., the majority were in age group 3 (56-70 years), 30% of analyzed patients were smokers, 30% had concomitant type 2 diabetes, 20% with obesity, 66% of patients had accompanying arterial hypertension. A family history of an early atherosclerotic event was found in 215 patients (49%) (Table 6).
| Gender | N | % |
| F | 128 | 29 |
| M | 310 | 71 |
| Age | ||
| <40> | 22 | 5 |
Table 6. Distribution of followed patients by demographic and clinical characteristics.
In 141 patients (32%), the GCM database had information on prior hospitalizations related to an atherosclerotic event (Table 6). This fact gives us reason to believe that antilipemic therapy has not been optimized in these individuals. This was also confirmed when analyzing baseline lipid profile levels (Figure 4) as well as baseline lipid-lowering therapy (Figures 5, 6). As it turns out, only 1.5% of patients were taking combined therapy - statin with ezetimibe. In 15% of patients, lipid-lowering therapy was never given (Figure 6).
According to the available lipid profile, the patients were divided into three groups (Table 4). As can be seen, most patients (74%) had LDL-C levels of 2.05 to 3.95 mmol/l, far from the target values of 1.4 and 1.8 mmol/l for the persons with extremely high and high cardiovascular risk, respectively.
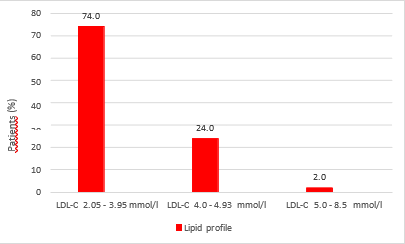
Figure 4: Distribution of patients by LDL-C levels at hospitalization, expressed as percentages:

Figure 5: Incoming lipid-lowering therapy by type of statin, expressed as a percentage.

Figure 6. Patients on ezetimibe monotherapy, combination therapy and no lipid-lowering therapy, expressed as a percentage:
In our prospective study, we demonstrated that with the help of artificial intelligence, the detection rate of patients with probable FH increased significantly and from 3 to 4.5 times patients were stared on PCSK9 inhibitor therapy.
It is noteworthy that in Cardiology clinics, the screening for FH is most successfully carried out. The reason for this may be due to the more frequent discussions of FH in the cardiology community and in cardiology departments compared to surgical specialties such as the Vascular Surgery and Cardiac Surgery Clinics. The non-analyzed patients in the Neurology Clinic appeared to be due to an unscreened lipid profile during hospitalization, which is a shortcoming of our analysis and perhaps needs to be changed as a strategy in this regard.
A disadvantage of our program that we find is that the dataset or AI algorithm is only available for use within our structure at the Hospitals of the Bulgarian Cardiology Institute and is limited to the hospital population level, making independent validation of the data not possible. Also, the presented analyses were conducted in a period when we did not monitor Lp a, as a more reliable marker for verifying patients with probable FH, as well as other markers for optimizing diagnosis. The role of the anti-aging gene, for example, Sirtuin 1, is crucial for the prevention of various chronic diseases such as diabetes and cardiovascular disease. It has been suggested that patients with FH should be evaluated for plasma levels of Sirtuin 1 in relation to insulin resistance and hepatic cholesterol metabolism. Sirtuin 1 activators versus Sirtuin 1 inhibitors could be evaluated in patients with FH (15).
The percentage of patients with concomitant diabetes mellitus type 2 (DM type 2) and hypercholesterolemia (30%) and arterial hypertension (66%) that we found were similar to those cited in the large study Da VINCI (38% for DM type 2 and 81% for arterial hypertension, respectively) associated with the use of lipid-lowering therapy in primary and secondary care in Central and Eastern Europe (CEE) (13). Da VINCI analyzed the proportion of patients from CEE who reached LDL-C targets based on individual cardiovascular risk recommended by the 2016 and 2019 ESC and European Atherosclerosis Society (EAS) guidelines. This study followed a total of 5,888 adults, of whom 2,154 were patients with dyslipidemia and lipid-lowering therapy in a CEE region believed to be undertreated, which is why this region of Europe has the highest cardiovascular mortality.
Patients from 18 European countries were included between June 21, 2017, and November 20, 2018, and for Eastern Europe, the Czech Republic (n=509), Hungary (n=319), Poland (n=460), Romania (n=259), Slovakia (n=123) and Ukraine (n=484). The researchers concluded that more than half of patients in CEE did not reach LDL-C target values, highlighting the significant gap between guidelines and clinical practice for dyslipidemias.
The results we achieved analyzing the patient profiles submitted by AI for FH screening are like those cited in Da VINCI. We also identified late-diagnosed FH patients with already overt atherosclerotic disease, who are untreated for dyslipidemia or insufficient therapy to effectively lower LDL-C (Figure 1, 2, 3). An additional impression, which we found in our work with patients with probable FH, is the lack of sufficient awareness on their part. Sometimes we saw an unjustified negative attitude of some patients and doctors towards the occurrence of side effects from taking statin therapy and the understanding of "adverse effects of high-dose statins". This was a frequent argument put forward by patients, why, despite an acute myocardial infarction, they are not optimal antilipemic therapy and why after optimizing LDL-C levels, they reduce the dose or even stop the drug. According to data from a retrospective study including patients with dyslipidemia followed for ≥3 years in a lipid clinic at a University Hospital in Greece, the frequency of clinically significant elevation of liver enzymes (>3× upper limit of normal (ULN) in 2) and statin-associated muscle symptoms (SAMS) expressed in muscle cramps, increased creatine kinase (CK) > 10 × ULN and rhabdomyolysis, during follow-up is low. Most of these patients were still able to tolerate statin treatment (14).
Unfortunately, in Bulgaria, a lack of criticality was also found among a significant number of doctors, mainly from outpatient practice and general practitioners, towards the pursuit of achieving target LDL-C levels and underestimation of patients with very high and high cardiovascular risk. Also, many patients stop taking statins and/or ezetimibe when treated with a PCSK9 inhibitor, which does not correspond to good clinical practice. These facts indicate the need for a broader discussion about FH, including the participation of both doctors and patients. Keeping a register for FH. We believe that the development of a family screening program for FH is necessary, as well as a rich informational awareness of patients. All this is related to the global change of the existing national strategy for patients with familial hypercholesterolemia.
Our ambition is to continue our research in this direction in the future. We are currently conducting a family screening program for patients identified by AI and treated for FH. We are working to expand the AI system to a larger number of healthcare facilities, with the aim of implementing integration with electronic health records, as well as application in primary care settings.
Unfortunately, potential obstacles that we would encounter are related to resource constraints and training requirements. Our goal is to continue using the program to identify patients with familial hypercholesterolemia in the future to achieve control of cardiovascular events. Our studies in this direction are ongoing. We have also added a routine serum Lp a test to the lipid panel. We are currently conducting a family screening program for patients identified by AI and treated for FH.
For our second outcomes – optimization of therapy, our conclusion is that the primary role is for the attending physician, to assess the patient's risk and follow the recommendations for behavior in dyslipidemias.
All these mentioned efforts, such as AI data analysis, screening, and proper treatment, will give us both an opportunity to recognize FH patients earlier and to implement cascade family screening. By reducing the rate of patients with cardiovascular events, the financial burden on health systems will be reduced and the quality of life of these patients will be improved, which is inextricably linked to a reduction in mortality in this population.
The development, implementation and use of AI for FH screening is workable in clinical practice and is easily applicable. The AI-based method identifies patients with probable FH. However, the role of the treating physician remains essential to make a correct diagnosis and initiate appropriate treatment, as well as to improve the patient's prognosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
