
Review | DOI: https://doi.org/10.31579/2693-4779/072
North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo. North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
Citation: Anthony K-G Venyo. (2022). Schistosomiasis of the testis and other intra-scrotal organs: A review and Update. Clinical Research and Clinical Trials. 5(2); DOI:10.31579/2693-4779/072
Copyright: © 2022 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 November 2021 | Accepted: 10 December 2021 | Published: 13 January 2022
Keywords: schistosomiasis of testis; schistosomiasis of epididymis; testicular mass, epididymal mass; epididymal cyst; hydrocele; testicular pain; scrotal pain; schistosoma; histopathology; excision; radical orchidectomy
Schistosomiasis of the testis and other intra-scrotal contents is a very rare condition which can be encountered within Schistosomiasis endemic areas of the world. Because of global travelling and swimming in rivers within Schistosomiasis endemic areas of the world, intra-scrotal Schistosomiasis tends to be sporadically reported in all areas of the world in male children and adults. Intra-scrotal Schistosomiasis may manifest as (a) testicular mass that may be painless and thus simulate testicular tumour, other intra-scrotal Schistosomiasis may present as hydrocele, epididymal cyst or solid/firm epididymal mass, a mass on the tunica or extra-testicular parts of the scrotum, testicular/intra-scrotal discomfort / pain. The lesion could mimic epididymo-orchitis on very rare occasions. There would tend to be a history of travel to or return from a Schistosomiasis endemic region in patients who normally dwell within the non-Schistosomiasis endemic areas of the world. There may also be a history of a previous episode of haematuria in some cases. The levels of serum Beta-Human Chorionic antigen, Alpha fetoprotein and Lactate Dehydrogenase usually tends to be normal. Some cases of Schistosomiasis of the testis had been mis-diagnosed as testicular cancer and the diagnosis of Schistosomiasis had been established based upon the histopathology examination findings of Schistosoma within the orchidectomy testis, but if there is a high-index of suspicion for Schistosomiasis of the scrotal content based upon a patient dwelling within or having travelled to a Schistosomiasis endemic area supported by a history of haematuria and the tumour or tumoral mass is completely excised for frozen section pathology examination, then the diagnosis of Schistosomiasis of the testis would be confirmed and the rest of the testis can be saved from excision. If all cases of excised epididymal cysts and Tunica from hydrocele operations are submitted for histopathology examination, then incidental cases of Schistosomiasis of scrotal contents would be made. Complete treatment of Schistosomiasis of testis and or scrotal contents does include excision / biopsy of the lesion for pathology examination confirmation and utilization of anti-Schistosomiasis medicaments. Schistosomiasis of intra-scrotal/testicular contents may be responsible for infertility and azoospermia and if this is properly investigated, diagnosed and treated this could be ensued by resolution of infertility with resulting pregnancy of the spouse and the production of a baby and because of this, individuals who have azoospermia and infertility in Schistosomiasis endemic areas, a high index of suspicion would be required in other to establish the cause as well as treat the cause of the infertility. Treatment of intra-scrotal content Schistosomiasis does entail excision / biopsy of the lesion plus utilization of anti-Schistosoma medicament and Praziquantel is a common medication that tends to be given and this tends to yield good outcome.
Schistosomiasis or Bilharziasis are terminologies that are utilized for a water-borne parasitic disease which does affect 200 million individuals as well as does pose a threat to 600 million individuals in more than 76 countries [1-4]. It has been iterated that Schistosomiasis is endemic within tropical as well as sub-tropical countries mainly within Africa and Eastern Mediterranean region. [5, 6]. It has additionally been iterated that cases of Schistosomiasis can be encountered nowadays within countries which are not within Schistosomiasis endemic zones of the world in view of the increase in global travels for tourism, business, as well as education [1]. Cases of Schistosomiasis of the testis and intra-scrotal contents are only rarely encountered in the world and in view of the rarity of cases of intra-scrotal content Schistosomiasis, majority of clinicians would not have encountered a case before and they may not be conversant with the diagnostic features of intra-scrotal Schistosomiasis. A number of cases of intra-scrotal / testicular Schistosomiasis had previously been provisionally diagnosed as malignant tumour of the testis and radical orchidectomy had been undertaken which would be regarded as unnecessary mutilating surgery. If clinicians can be thought to have a high-index of suspicion of intra-scrotal Schistosomiasis in individuals who dwell in Schistosomiasis endemic areas and individuals who have travelled to and returned from Schistosomiasis endemic areas who had swam in rivers in the Schistosomiasis endemic areas or in individuals who have a past history of haematuria and a previously history of having travelled to a Schistosomiasis endemic area, then in such patients when they manifest with intra-scrotal lesions such patients could be made to have frozen section histopathology examination of their completely excised intra-scrotal masses to confirm a diagnosis of Schistosomiasis in order to avoid radical orchidectomy. The ensuing article on Schistosomiasis of the testis and scrotal contents is divided into two parts: (A) Overview of Schistosomiasis in general and (B) Miscellaneous Narrations and Discussions from some Case Reports, Case Series and Studies Related to Schistosomiasis of the testis and intra-scrotal contents.
Internet data bases were searched including: Google, Google Scholar, Yahoo, Academia, and PUBMED. The search words that were used included: Schistosomiasis of testis; Schistosomiasis of epididymis, intra-scrotal Schistosomiasis, Bilharzia of testis, and intra-scrotal bilharziasis. ---Thirty eight references were identified which were used to write the article which has been divided into two parts: : (A) Overview of Schistosomiasis in general and (B) Miscellaneous Narrations and Discussions from some Case Reports, Case Series and Studies Related to Schistosomiasis of the testis and intra-scrotal contents.
[(A)] Overview
Definition / general
It has been iterated that Schistosomiasis or bilharziasis is one of the most important parasitic diseases globally, which does afflict 200 million to 300 million individuals [7].
It has been iterated that the adult male and female blood flukes tend to inhabit the veins of the mesentery or urinary bladder [7].
It has been iterated that the most important Schistosoma species that infect human beings include: Schistosoma mansoni, Schistosoma japonicum, Schistosoma mekongi, Schistosoma haematobium and Schistosoma intercalatum; as well as other Schistosoma species tend to infect human beings less frequently [7].
Epidemiology
It has been iterated that Schistosomiasis is an important cause of disease in many parts of the world, as well as Schistosomiasis is most commonly encountered within places of the world that have poor sanitation. [7].
It has additionally been documented that School age children who live within places in the world that have poor sanitation often tend to be most at risk for the development of Schistosomiasis in view of the fact that they tend to spend time swimming or bathing within water containing infectious cercariae [7].
The risk factors for the development of Schistosomiasis have been documented to include: living within or travelling to Schistosomiasis endemic areas of the world as well as exposure to contaminated freshwater [7].
Schistosoma mansoni is well known to be distributed throughout the entire Africa:
It has been iterated that Schistosoma mansoni tends to be found within freshwater in southern and sub-Saharan Africa, with the inclusion of the great lakes, rivers and smaller bodies of water in Africa [7].
It has also been documented that Schistosoma mansoni is also found within the valley of River Nile River within Sudan and Egypt, South America (Brazil, Suriname, Venezuela), Caribbean (low risk, as well as within the Dominican Republic, Guadeloupe, Martinique, Saint Lucia). [7].
Schistosoma haematobium is well known to be distributed throughout Africa: [7]
Schistosoma haematobium tends to be found within freshwater in southern and sub-Saharan Africa, with the inclusion of the great lakes, rivers and smaller bodies of water [7].
Schistosoma haematobium also tends to be found within the valley river Nile in Egypt, as well as the Mahgreb region of North Africa [7].
Found in areas of the Middle East [7].
Eggs hatch within 15 - 30 minutes [7].
Schistosoma japonicum is known to be found within Indonesia and parts of China as well as within Southeast Asia [7].
Schistosoma. Mekongi is said to be found in Cambodia and Laos [7].
Schistosoma. intercalatum tends to be found within parts of Central and West Africa [7].
Sites
Appendix [7].
Schistosomiasis affecting the appendix is common, but it usually doesn't cause acute appendicitis
Schistosoma may cause appendicitis in regions endemic for schistosomiasis
In Schistosomiasis there may be prominent eosinophilic infiltrate within appendix the appendix
Pathophysiology
Eggs are deposited in smallest venule that can accommodate the female worm, where they elicit a strong granulomatous response that results in extrusion of the egg into the intestinal lumen or the bladder [7].
Pathology is primarily related to sites of egg deposition, number of eggs deposited and host reaction to egg antigens [7].
Clinical features [7].
Symptoms of schistosomiasis result primarily from penetration of cercariae (cercarial dermatitis), from initiation of egg laying (acute schistosomiasis or Katayama fever) and as a late stage complication of tissue proliferation and repair (chronic schistosomiasis) [7].
Hours after cercarial penetration, a papular rash may develop, associated with pruritus [7].
This is a sensitization phenomenon resulting from prior exposure to cercarial antigens [7].
Most severe form of dermatitis occurs in individuals who are repeatedly exposed to cercariae of nonhuman (primarily avian) schistosomes [7].
Cercarial dermatitis or swimmer's itch occurs worldwide and is a well-recognized entity in the United States [7, 8].
Initiation of egg laying by mature worms 5 - 7 weeks after infection may result in acute schistosomiasis or Katayama fever, a serum sickness-like syndrome that occurs with heavy primary infection, especially that of Shistosoma. japonicum
Antigenic challenge to the host is thought to result in immune complex formation [7, 8].
Chronic infection results in continued deposition of eggs, many of which remain in the body [7].
Granulomas produced around these eggs in the intestine and bladder are gradually replaced by collagen, resulting in fibrosis and scarring [7].
Eggs trapped in the liver may induce pipe stem fibrosis with obstruction to portal blood flow [7].
Occasionally, eggs are deposited in ectopic sites, such as the spinal cord, lungs or brain [7].
Coinfection with Schistosoma mansoni and HIV1 may occur [7-9]
Life cycle
Eggs are fully embryonated when passed and readily hatch when deposited in fresh water [7].
Miracidia penetrate an appropriate species of snail host, where they undergo transformation and extensive asexual multiplication [7].
After about 4 weeks, large numbers of fork tailed cercariae emerge from the mollusk [7].
Cercariae swim actively about for hours and readily penetrate the skin of susceptible hosts, including humans [7].
After penetration, the cercariae, now called schistosomules, enter the circulation and pass through the lungs before reaching the mesenteric portal vessels [7].
Presentation
Some of the possible presentations of intra-scrotal / testicular Schistosomiasis do include the following:
Testicular mass
Nodule in testis
Intra-scrotal mass
Hydrocele
Pain in testis
Intra-scrotal pain,
Infertility
Azospermia
Epididymal cyst
There may be a past history of haematuria
With regard to patients in Schistosomiasis non-endemic area, a history of having travelled to a Schistosomiasis endemic area as well as swimming in a river may be obtained and possibly a history of haematuria could be elicited
Non-specific Intra-scrotal pain / testicular pain / discomfort.
Clinical examination
The general and systematic examination of individuals whether they are children or adults who have intra-testicular Schistosomiasis would generally tend to be normal and examination of the testis and scrotal contents would demonstrate features related to the organ involved as follows irrespective of the age of the patient:
A mass within the testis that could mimic a testicular tumour,
A hydrocele.
Epididymal cyst type of lesion.
A nodule within the testis
A nodule on the epididymis.
A mass within the scrotum.
Radiology imaging
Ultrasound scan of scrotal contents.
Ultrasound scan of scrotal contents would tend to demonstrate various types of lesions depending upon the intra-scrotal organ that has been affected including (a) solid lesion in an area of the testis, a solid lesion in the epididymis, a solid lesion on the spermatic cord, or within the scrotum, a cystic lesion in the testis, epididymis, spermatic cord, or any other intra-scrotal region. Evidence of a hydrocele could also be demonstrated as elaborated upon in the second part of the article.
Computed Tomography (CT) Scan of Scrotal contents
CT scan of scrotal contents would tend to demonstrate various types of lesions depending upon the intra-scrotal organ that has been affected including (a) solid lesion in an area of the testis, a solid lesion in the epididymis, a solid lesion on the spermatic cord, or within the scrotum, a cystic lesion in the testis, epididymis, spermatic cord, or any other intra-scrotal region. Evidence of a hydrocele could also be demonstrated as elaborated upon in the second part of the article.
Magnetic Resonance Imaging (MRI) Scan
MRI scan of scrotal contents would tend to demonstrate various types of lesions depending upon the intra-scrotal organ that has been affected including (a) solid lesion in an area of the testis, a solid lesion in the epididymis, a solid lesion on the spermatic cord, or within the scrotum, a cystic lesion in the testis, epididymis, spermatic cord, or any other intra-scrotal region. Evidence of a hydrocele could also be demonstrated as elaborated upon in the second part of the article.
Diagnosis
Diagnosis of Schistosomiasis of the testis and intra-scrotal contents need to be considered as a possibility if there is evidence Schistosomiasis based upon the following:
Diagnosis is established by demonstrating eggs in faeces or urine by direct wet mount or formalin ethyl acetate concentration methods [7].
Zinc sulphate concentration is not satisfactory for recovery of heavy schistosome eggs [7].
Eggs may be detected in biopsies of rectum, bladder or occasionally liver [7].
Egg hatching methods may occasionally be requested to determine viability or less commonly, to detect a limited infection [7].
Faeces mixed in distilled water is placed in a flask, covered with foil (to keep out light), with neck or a sidearm exposed to bright light
Miracidia, if present, actively swim to the light and can be detected using a hand lens
Confirmation of Schistosomiasis of the testis, epididymis, tunica, spermatic cord, and seminal vesicle or an intra-scrotal content organ can be confirmed based only upon pathology examination of an excised intra-scrotal organ evidence of Schistosoma within the scrotal content organ as illustrated a number of times in the second part of the article.
Laboratory
Serologic tests may be useful for screening travellers to endemic areas, at risk patients with negative urine / stool examinations, monitoring response to therapy [7].
Although not widely available, a limited number of reference laboratories and the CDC provide testing [7].
CDC uses the Falcon assay screening test in a kinetic enzyme linked immunosorbent assay (FAST ELISA); sera that are positive by screening test are evaluated by immunoblot to improve specificity [7].
Results vary based on antigens used and the test methods employed [7].
On the whole investigation and diagnosis of Schistosomiasis of the testis and scrotal contents would include the following: [10]
Full blood count: - Even though the results would not be diagnostic of Schistosomiasis, evidence of eosinophilia should remind clinicians to consider the possibility of a parasitic infection.
Increased alkaline phosphatase levels and increased gamma-glutamyl transferase (GGT) levels - these could be observed in hepatic Schistosomiasis granulomatosis but this would generally be rarely encountered in Schistosomiasis of the testis and this finding would not be diagnostic of Schistosomiasis of testis but a past history of this in association with a testicular mass subsequently should alert the clinician to consider the possibility of Schistosomiasis of testis.
Urine Microbiology test – To detect Schistosoma but this would not be diagnostic of Schistosomiasis of testis but should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Stool Microbiology test - To detect Schistosoma but this would not be diagnostic of Schistosomiasis of testis but should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Polymerase Chain Reaction (PCR) test – This test tends to be 94.4% sensitive and 99.9% specific for the diagnosis of Schistosomiasis but would not be diagnostic of Schistosomiasis of testis. The test is to detect Schistosomiasis but this would not be diagnostic of Schistosomiasis of testis but positive result should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Egg viability test - To detect Schistosoma but this would not be diagnostic of Schistosomiasis of testis but should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Serology test – To detect Schistosomiasis in general but it cannot be used to differentiate between active and past Schistosomiasis. Antibody detection to Schistosoma mansoni, Schistosoma haematobium, and Schistosoma Japonicum by undertaking the following:
Microsomal antigens for example.
Mansoni adult worm microsomal antigen (MAMA)
Haematobium adult worm microsomal antigen (HAMA).
Japonicum adult worm microsomal antigen (JAMA).
This can be done through the use of Falcon Assay screening test (FAST), enzyme-linked immunoassay (ELISA), and Immunoblot [11] To detect Schistosoma but this would not be diagnostic of Schistosomiasis of testis but should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Antigen test - The two proteoglycan, gut-associated antigens which do appear most promising include: circulating anodic antigen (CAA) and circulating cathodic antigen (CCA). It has been stated that CAA and CCA can be detected in urine or serum [10, 13].
These tests would detect Schistosoma but this would not be diagnostic of Schistosomiasis of testis but should alert the clinician to the possibility of Schistosomiasis of the testis so that a frozen section biopsy of the excised testicular mass / lesion / nodule could be taken to establish the diagnosis before procedure to undertake radical orchidectomy or limit the procedure to complete excision of the testicular mass thus saving some testicular tissue.
Diagnosis Confirmation
This is based upon histopathology examination finding of Schistosoma/eggs within the excised or biopsied intra-scrotal lesion.
Prognostic factors
Patients with coexisting HBV or HIV infections have worse prognoses [7].
Prevention
No vaccine is available to prevent schistosomiasis of the testis [7].
Recommendations:
It order to avoid Schistosomiasis infection individuals are advised to avoid swimming or wading in fresh-water within Schistosomiasis-endemic countries and it has been pointed out that ocean and chlorinated swimming pools are safe with regard to not being infested by Schistosoma organism. [7].
Individuals are advised to drink water which is adjudged which is safe for drinking purposes. [7].
Individuals have been advised to apply vigorous towel drying of their towels pursuant their accidental, very brief exposure to water in a Schistosomiasis endemic area in order to prevent penetration of their skin by the parasite; nevertheless, it has been pointed out that this measured tends to be associated with limited effectiveness [7].
Treatment
With regard to the treatment of schistosomiasis in general, it has been iterated that: [7]
Utilization of Praziquantel, which when taken for 1 day to 2 days, is safe and effective for urinary and intestinal infections by all Schistosoma species
Microscopic histological examination features [7].
It has been iterated that microscopy pathology examination of specimens that are infected by Schistosoma tend to demonstrate the following: [7].
Focal ulcers, eggs could be calcified and encompassed by fibrosis or granuloma
Schistosoma. haematobium: eggs tend to be 110 microns to 170 microns by 40 microns to 70 microns, oval with terminal spine
Schistosoma. Japonicum eggs tend to measure 70 microns to 100 microns by 55 microns to 65 microns, as well as they tend to be oval / round (more rounded than other types), minute subterminal or no spine
Schistosoma mansoni: eggs tend to measure 110 microns to 175 microns by 45 microns to- 70 microns with thin transparent shell and definite lateral spine
It has been iterated that adult female schistosomes tend to be slender, and they tend to measure up to 26 mm by 0.5 mm
It has also been documented that males, which tend to be slightly shorter, do enfold a female using the lateral margins of the body (the gynecophoral canal) in order to assist in the transfer of sperm.
It has been iterated that when schistosomes are examined in situ, they often tend to be found within copula [7].
Differential diagnoses
Some of the differential diagnoses of Schistosomiasis of the testis include:
It has been stated that Uric acid crystals are regarded as differential to the diagnosis of Schistosoma but Uric acid crystals tend to have variability of size as well as points on both end like a lemon and in contrast, Schistosoma. haematobium eggs tend to have a defined "pinched off" terminal spine and larval form (miradium) within [7, 14].
Malignant testicular tumour of testis
Hydrocele
Epididymo-orchitis / torsion on rare occasions
Other causes of infertility and azoospermia
Other differential diagnoses of intra-scrotal Schistosomiasis including Schistosomiasis of testis and tunica include:
Epididymal cyst
Epididymitis / epididymo-orchitis
[(B)] Miscellaneous Narrations And Discussions From Some Case Reports, Case Series, And Some Studies Related To Schistosomiasis In General With A Focus On Schistosomiasis Of The Testis.
Ihekwaba [15] stated that Schistosoma orchitis is still rare in many countries, and when Schistosoma orchitis manifests, it does present difficulties with regard to the correct diagnosis as well as Schistosoma orchitis does simulate testicular cancer, a misdiagnosis which invariably does lead to radical orchidectomy which does represent an unfortunate event in the young patient.
Ekenze et al. [16] reported a 13 year old boy who had manifested with a left hemi-scrotal swelling which had dated back to his infancy that was ensued by intermittent visible haematuria over the preceding 5 years. He had lived with his parents at Ishielu in Ebonyi state of Nigeria, which is one of the schistosomiasis-endemic areas within Nigeria. His scrotal swelling had been progressive and spontaneously reducible up until 2 years prior to his manifestation, when it became irreducible. He was asymptomatic otherwise. He described his haematuria as terminal and intermittent, but it had not necessitated blood transfusion. There was no history of haematuria among his siblings and his parents. His source of water was a stream. He was referred to the urology department following a failed herniotomy during which a ‘hard testis’ was found. Upon examination he was noted to be mildly pale and to have a non-tender, hard, non-reducible left hemi-scrotal swelling that measured 8 cm x 6 cm with an oblique inguinal scar. HIs left testis was not distinct from the mass and he did not have palpable inguinal nodes. There was evidence of a reducible right inguinoscrotal hernia. He had laboratory investigations including routine haematology and biochemistry blood tests as well as urine and stool tests which revealed haemoglobin level of 8.0 g/dl, serum alpha-feto-protein level of 3.0 ng/ml as well as absence of Schistosoma ova within his urine and stool specimen. He had ultrasound scan of his scrotal contents, abdomen and pelvis which demonstrated a left hemi-scrotal mass that measured 7.7 cm in its widest dimension and which had heterogenous echogenicity and intact margin. The right testis did measure 3.2 cm × 2.1 cm and it had a homogenous echotexture. There was no evidence of enlargement of his para-aortic nodes. He underwent exploration of his left scrotal mass through an inguinal approach. During the procedure, a 10 cm × 6 cm, hard and irregular mass was found with a scar from a previous surgery and significant fibrous tissues. The scrotal mass was completely excised. During the procedure, inspection of his right testis during his right herniotomy demonstrated a suspicious nodule that measured about 0.5 cm. The nodule was excised. His post-operative recovery was unremarkable, and he was discharged on the third post-operative day. Macroscopic examination of the cut scrotal mass demonstrated an outer surface which was well encapsulated and rough. The internal surface of the mass was greyish white with predominantly solid areas and few cystic areas which did contain jelly-like substance in their loci. Microscopy histopathology examination of the left scrotal mass and the nodule on the right testis did demonstrate total replacement of the normal testicular architecture by many non-caseating granulomas which were centred upon viable and degenerating Schistosoma ova; some of the Schistosoma ova were calcified. Many eosinophils and fibrous tissue were visualised around the granulomas. No atypical cells were found. Pursuant to the histopathology examination confirmation of Schistosomiasis he was commenced on praziquantel. He was followed up for 3 months and he had been scheduled to attend for regular clinical and ultrasound scan assessments of his scrotal contents. Some of the lessons that need to be learnt from this case report include: (a) Even though rare, Schistosomiasis of the testis can occur in Schistosoma endemic parts of the world as well as in Schistosomiasis non-endemic areas of the world in individuals who have travelled to Schistosomiasis endemic areas and hence clinicians should have a high-index of suspicion for the disease. (b) Schistosomiasis of the testis could manifest as an intra-testicular / scrotal mass for many years without any significant problem, (c) Schistosomiasis of the testis may be associated with episodes of visible haematuria, (d) Schistosomiasis of the testis tends to simulate testicular tumour, (e ) because of the possibility of Schistosomiasis of testis in Schistosomiasis endemic areas of the world that may simulate testicular tumour, all individuals in Schistosomiasis endemic areas who present with testicular mass and visible haematuria should be offered cystoscopy plus or minus biopsy of any intravesical lesion that may be found as well as they should have radiology imaging and when the pathology department is near-by then frozen section examination of the testicular mass should be undertaken during exploration of the testicular mass to ascertain if the mass is malignant or a case of Schistosomiasis in order to avoid unnecessary radical orchidectomy in cases of Schistosomiasis of the testis.
Dauda and Rafindadi. [17] reported a 16-year-old old male who had manifested with an 8-weeks history of painless and gradually increasing left hemi-scrotal swelling. He had manifested with terminal haematuria, six years earlier for which he was treated by a chemist. His clinical examination demonstrated a swelling of his testis that was spherical in shape and associated with normal overlying scrotal skin. The testis was firm in consistency and during examination, the clinician could not get above the swelling. The testicular swelling was non-tender and the spermatic cords were found to be normal during the examination. There was no evidence of inguinal lymph node enlargement during the examination. Examination of his abdomen was normal. A provisional diagnosis of testicular tumour was made. He had ultrasound scan of abdomen and pelvis as well as scrotal ultrasound scan. His ultrasound scan of abdomen and pelvis were normal and his ultrasound scan of his scrotal contents demonstrated a homogeneous solid mass which was considered to be probably seminoma of testis. His urinalysis was normal. He underwent a trans-inguinal left radical orchidectomy and during the procedure, when the testis was delivered, a 15 cm x 5 cm x 2 cm x 5 cm tumour was found. The tumour mass was hard in consistency and multi-nodular. Macroscopy examination showed that the tumour had weighed 40 grams and the cut section of the lesion demonstrated grey to yellow solid areas which had compressed the yellow testicular tissue. Microscopy histopathology examination of the specimen demonstrated almost total replacement of the testicular and para-testicular tissues by a large number of Schistosoma haematobium ova and some of these were viable whilst others were dead. The lesson to be learnt from this case summation is the fact that Schistosomiasis of the testis does simulate the features of a testicular tumour and in view of this clinicians who encounter patients in Schistosomiasis endemic areas who manifest with testicular mass and who have had a history of visible should be assessed for the possibility of Schistosomiasis of the testis so that during their surgical exploration of the testis to undertake radical orchidectomy, a frozen section pathology examination of the testicular lesion should be undertaken so that those who are found to have Schistosomiasis of the testis could be spared unwarranted radical orchidectomy so that the testis could be spared.
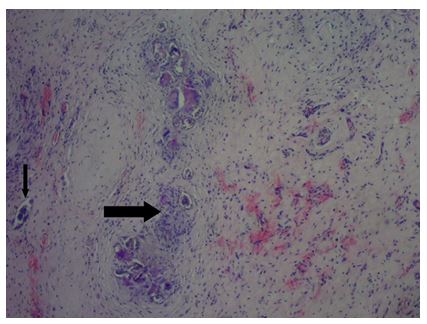
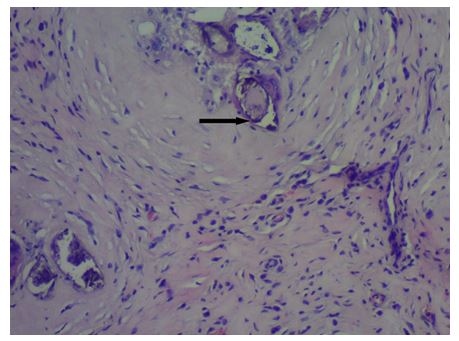
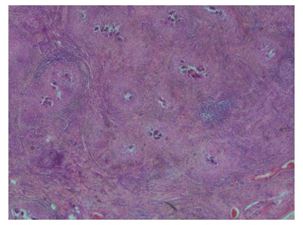
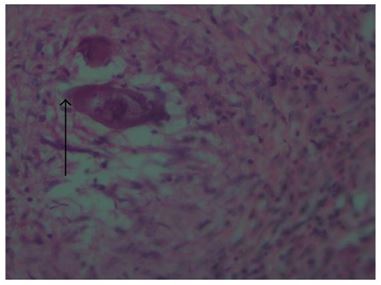
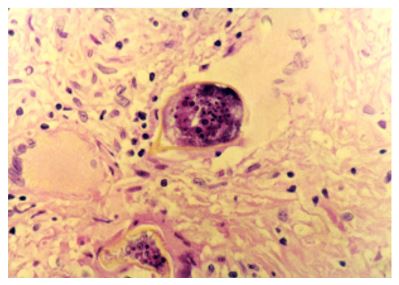
Oguntunde et al. [18] reported a 9 year old boy who was apparently well until about 10 months preceding his manifestation when he was noted to have developed a painless right hemi-scrotal swelling. The swelling had steadily increased with regard to its size and it never reduced. He was taken to a peripheral hospital where he was referred to the paediatric surgical unit of a secondary health care facility. He was born in Saki, a community within the south-western region of Nigeria where he grew up until approximately 3 years preceding his manifestation when he relocated with his family to Lagos metropolis. While in Saki, he often had swam in the local river. He did not have any history of haematuria in the past nor during the course of his illness. His clinical examination demonstrated a small for age boy who had an encysted, irreducible right hemi-scrotal mass that measured 10 cm x4.5cm, which was not tender and not warmer in comparison with the encompassing skin and it did trans-illuminate brilliantly to light. His left testis was unremarkable. A diagnosis of a right vaginal hydrocoele was made and the parent was counselled regarding surgery. His pre-operative laboratory investigations demonstrated a haematocrit level of 35%, HIV status (after obtaining consent from parents) was negative, HBsAg was positive, blood genotype AA, electrolyte, urea and creatinine values were essentially normal. He was next subsequently scheduled to undergo a day case routine herniotomy. During the surgical procedure, the findings included hydrocoele that had multiple cysts, flat testis and thickened spermatic cord (see figure 1). Biopsy was taken from the testis and spermatic cord. He was discharged home on same day. Histopathology examination of the biopsy specimens demonstrated fibro-collagenous tissue that contained many granulomata within a background of dense admixed eosinophilic rich inflammatory infiltrates (see figure 2). The histopathology examination also demonstrated many multinucleated giant cells and Schistosoma ova, some of which were calcified and they had terminal spine (see figure 3). The presence of terminal spine confirmed Schistosoma haematobium and a diagnosis of schistosomiasis was made. He was commenced on praziquantel 400mg stat pursuant to receiving the histology report and he had been undergoing followed up assessments in the outpatient clinic at the time of the report of his case. A lesson tom learn from this case report is that some cases of Schistosomiasis of the testis may simulate as well as manifest as hydroceles. In view of this clinicians who undertake surgical operations for hydroceles in patients who dwell in Schistosomiasis endemic areas should have a high index of suspicion for Schistosomiasis associated hydrocele so that they can undertake biopsies of the tunica or any abnormal looking tissues they encounter during their surgical procedures for histopathology examination which would confirm the diagnosis of Schistosomiasis.

Badmus et al. [19] reported a a case of testicular Schistosomiasis with a suspicion of testicular cancer. The hospital record of a 16 year old patient who had a histopathology confirmation of testicular Schistosomiasis was reviewed. The patient presented with painless testicular nodules and he had ultrasound scan of his scrotal contents which showed features of heterogenous echotexture and hypoechoic focus which was diagnosed as testicular cancer for which he underwent radical orchidectomy. Histopathology examination of the radical orchidectomy specimen confirmed Schistosomiasis of the testis and the patient had additional praziquantel therapy. The patient was followed-up for more than 26 months and remained well post-operatively. Badmus et al. [19] made the following conclusions:
Testicular Schistosomiasis of the test is, can simulate malignant testicular tumour.
Hard nodular mass in the testis in a patient who has a recent past history of schistosomiasis should arouse suspicion of Schistosomiasis of the testis.
Awareness and early presentation would prevent unwarranted orchidectomy.
Ze Ondo. et al. [20] stated that Bilharziomas are inflammatory pseudo-tumours, which often pose the problem of differential diagnosis of neoplastic processes. Using the keywords "testicular" and "schistosomiasis", Ze Ondo et al. [20] in 2014 found that the were only 14 cases of testicular bilharzioma which they identified upon PubMed search. Ze Ondo et al. [20] reported two new cases in a 6-year-old child and an adult of 38 years, which were collected over a period of 5 years. In both cases, orchidectomy was undertaken and histopathology examination of the orchidectomy specimens showed features of bilharzioma of testis which was caused by Schistosomia haematobium. Ze Ondo et al. [20] emphasized the need to evoke a bilharzioma before any testicular nodule in a patient living in an endemic area is treated by surgical means.
Hassan et al. [21] reported a case of testicular schistosomiasis.in a 26-year-old unmarried Egyptian man who had presented with slowly growing painless swelling within his right hemi-scrotum. He had various assessments including clinical examination, scrotal ultrasound scan, magnetic resonance imaging (MRI) scan, computerized tomography scan, urine and semen Zeihl-Neelsen stain, stool, serum alpha-fetoprotein, FSH, LH, PRL, E2, total testosterone (T), tests were undertaken and he underwent surgical exploration of the right testicular mass. His clinical examination demonstrated a large painless swelling within his right hemi-scrotum with two hard masses which were felt subcutaneously. His transillumination test was negative with no inguinal lymph node enlargement was found. His left hemi-scrotal contents were found to be normal. The results of his serum alpha-fetoprotein, FSH, LH, total T, E2, and PRL were within normal limits. His MRI scan showed no masses of abnormal signal intensity or enhancement. He underwent scrotal surgical exploration which did demonstrate a discharge of thick brownish red pus with presence of two hard extra-testicular scrotal masses. Histopathology examination of his right testis biopsy revealed reduced diameter of the seminiferous tubules with marked hypo-spermatogenesis where the interstitium was filled by multiple Schistosoma mansoni ova that was associated with granulomatous reaction compressing the tubules. Hassan et al. [21] concluded that scrotal involvement in schistosomiasis with its variable manifestations should be considered in diagnosing scrotal masses, especially in Schistosomiasis endemic areas.
Elbadawy et al [22] reported an eighty-eight-year-old Puerto Rican who had presented with painless enlargement of one testis which proven upon histopathology examination to be due to Schistosoma mansoni. Intratesticular ovum deposits were not associated with inflammation, granulomas, or infarction, but marked sclerosing peri orchitis was found. Elbadawi et al. [22] stated that their reported case had illustrated a very rare form of presentation of schistosomiasis which should be considered in the differential diagnosis of unilateral testicular enlargement in patients from a Schistosomiasis endemic area, despite the fact that orchidectomy would usually be necessary to establish a definitive histopathology diagnosis of Schistosomiasis of testis.
Ferreira et al. [23] stated that despite its infrequent occurrence, schistosomiasis of testis which form pseudo-tumours could be considered in the differential diagnosis of testicular tumours, especially within areas where the parasitic disease is endemic. Ferreira et al. [23] reported a case of testicular schistosomiasis which was caused by Schistosoma mansoni and which had mimicked a testicular neoplasm. Ferreira et al. [23] described the patterns of a testicular nodule which was demonstrated upon ultrasonography and magnetic resonance images in a 46-year-old man. The nodule was removed after a pre-operative diagnosis of a non-malignant lesion. Histology examination excised nodule demonstrated granulomas with epithelioid macrophages and eosinophils around S. mansoni eggs within a fibrous tissue that formed a nodular structure.
Periyasamy et al. [24] iterated the following:
Data which was obtained from the WHO has documented that up to 85% of cases of human schistosomiasis are from Africa.
The common sites of Schistosomiasis infection are the intestine and urinary bladder.
Schistosomiasis of the testis is extremely uncommon but the number of reported cases of Schistosomiasis of the testis worldwide has doubled over the preceding decade.
Periyasamy et al. [24] reported a case of schistosomiasis of the testis of a Myanmar immigrant in Malaysia who had manifested with a 6-month history of progressively enlarging left testicular swelling. The results of his biochemical markers and cultures were not suggestive of an ongoing infection. In view of this, a testicular malignancy was strongly suspected, for which, he underwent a left radical orchidectomy. Their clinical suspicion was proven wrong when the histopathology of the excised left testis demonstrated Schistosoma eggs with granulamatous tissue formation. Subsequently, the patient was treated with praziquantel.
Lopes et al. [25] stated that testicular schistosomiasis which is caused by Schistosoma mansoni is exceedingly rare, with only 11 cases in 2007 reported in PubMed. Lopes et al. [25] reported a new case from Brazil. They reported a 31-year-old man from the northeast region of the country who had presented with a 2 cm nodule within his right testis. He had ultrasound-scan of his scrotal contents which showed a well-delimited hypoechoic tumour, which was suggestive of a granulomatous lesion. Magnetic resonance imaging scan demonstrated an irregular tunica albuginea signal. A biopsy of the testicular lesion was undertaken and histopathology examination of the specimen showed interstitial tissue with schistosome ova and granuloma formation. The nodule was excised, and the patient was treated with oxamniquine. He had remained symptom free for 10 years. Lopes et al. [25] stated the following:
The finding of a testicular nodule should raise the suspicion of many pathologies, including schistosomiasis.
Treatment should include therapy with oxamniquine or praziquantel, and excision of the nodule should be undertaken whenever possible.
Al-Qahtani et al. [26] stated that schistosomiasis of the testis is extremely rare, with only 12 cases reported by 2012 and that reaching the diagnosis for this lesion which does mimic malignant tumour is a great dilemma for the radiologist as well as the urologist. Al-Qahtani et al. [26] reported a case of testicular schistosomiasis from France that was managed conservatively. Al-Qahtani et al. [26] reported a 31- year-old Egyptian man who had presented to the outpatient clinic with primary infertility over a period of 9 years. His clinical examination revealed a healthy man who did not have any congenital malformations. The results of his blood count and C-reactive protein level were normal. The results of his hormonal tests were normal. He had ultrasound scan of his scrotal contents which showed a small mass within his right testis. He underwent scrotal exploration and frozen section pathology examination of the testicular lesion confirmed a diagnosis of schistosomiasis. He was given medical treatment, and his further investigations were normal. Al-Qahtani et al. [26] stated the following:
A thorough evaluation must be undertaken, and testicular schistosomiasis should be considered in patients who dwell within Schistosomiasis endemic areas.
They would emphasize the lack of data to reach the diagnosis of Schistosomiasis of testis based upon radiological imaging.
Wedel et al. [27] reported a case of a 13-year-old boy who had schistosomiasis within his right testis, which simulated a malignant tumour. The tumour was excised, and in view of the fact that microscopy examination of frozen section excision biopsy specimen of the lesion showed granulomatosis without malignancy, the testis was saved. Wedel et al. [27] emphasized, that testicular involvement is rare and for this reason, a high-index of suspicion would be required to establish the diagnosis of Schistosomiasis of testis.
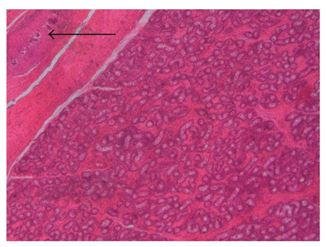
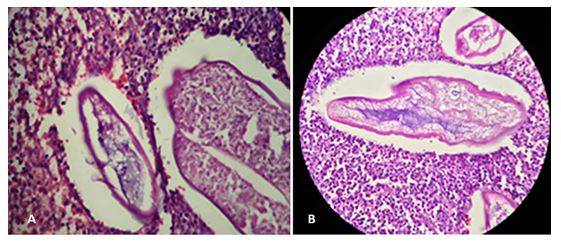
Rambau et al. [28] reported the cases of a 9-year-old boy who was referred from Magu district hospital to Bugando Medical centre with a history of left hemi-scrotal pain and swelling for one year. The swelling was reported to be progressive increasing in size, and this was accompanied by pain, and he did not have any history of fever, weight loss, or evening fevers. He did not have any history of haematuria in the past or during the course of his illness. The patient had been utilising local medicine of unknown nature without any improvement. At district hospital, he was given antibiotics and analgesic drugs without any improvement, and the patient was referred to Bugando Medical Centre. Upon examination, the boy was found to be well-nourished with no jaundice or pallor. His systematic examinations were all essentially normal. His local examination demonstrated a left hemi-scrotal swelling, which was slightly tender, cystic with regard to consistency, and the clinician could not get above it, and it was irreducible, and this gave an impression of hydrocele. It was planned that the patient should undergo hydrocelectomy. The results of his initial investigation revealed a haemoglobin of 11.5 gm/dL, blood group B Rh+, and urine and stool were found to be normal with no ova. The patient underwent surgery and the findings during the surgical included: a hydrocele, thickened tunica and small nodules on the surface of the testis which created suspicion for testicular tumour, and orchidectomy was undertaken. The patient had uneventful post-operative recovery and was discharged after seven days. Macroscopy pathology examination of the excised specimen showed a cystic wall of 4 cm × 4 cm × 3 cm, and a testis of 1 cm × 0. 5 cm, which looked atrophic and yellowish with firm nodules upon its surface. Histopathology examination of the specimen with haematoxylin and eosin stain (H and E) revealed an active chronic granulomatous inflammation with epithelioid macrophages and foreign body giant cells and many Schistosoma eggs within the thickened tunica albugenia with eosinophils infiltrate. The testis was not involved, and it demonstrated atrophic changes with fibrosis. Histopathology examination of the specimen also showed that the epididymis was also normal with only dilatation. Close examination of the specimen showed that the eggs did contain terminal spine that was consistent with Schistosoma. haematobium; and the eggs were not calcified (see figures 4, 5, and 6), which indicated active inflammation. The patient was followed-up in the outpatient department and it was noted that he did not have any further complaints, and the patient was given Praziquantel 400 mg start.
Kini et al. [29] iterated that azoospermia is an uncommon, and irreversible complication within the United Kingdom which results from heavy infection of schistosomiasis of the male genital tract and that adequate anti-bilharzial treatment as well as close follow-up with urological assessments should be able to reduce the risk of chronic ill health. Kini et a. [29] reported a man who had contracted schistosomiasis following his swimming in lakes in Uganda, Africa, which resulted in his development of azoospermia and reversible loss of libido. The patient and his spouse underwent treatment within the assisted conception programme of Kini et al. [29] with testicular sperm extraction and intracytoplasmic sperm injection (ICSI). The patient’s female partner conceived in her second stimulated ICSI cycle and had a spontaneous vaginal delivery at term. A lesson that has been learnt from this case summation is the fact that a patient who develops intra-scrotal/intra-testicular/epididymal schistosomiasis could develop azoospermia that would be ensued by infertility and that individuals who dwell in Schistosomiasis endemic areas and those who have travelled to and returned from Schistosomiasis endemic areas who are found to have azoospermia should be fully assessed for intra-scrotal/testicular/epididymal Schistosomiasis and when the diagnosis of intra-scrotal Schistosomiasis is made their problem of infertility could be treated by means of testicular sperm extraction and intracytoplasmic sperm injection in patients who are found to have obstructive azoospermia.
Abdel-Naser et al. [30] stated that congenital bilateral absence of vas deferens (CBAVD) does result in obstructive azoospermia in which testicular function, such as spermatogenesis, tends to be preserved. They also stated that bilateral biopsy of testis is not only diagnostic but also therapeutic in view of the fact that retrieved spermatozoa are usually cryopreserved for assisted reproduction. Abdel-Naser et al. [30] reported CBAVD which was confirmed in a 24-year-old man who had azoospermia upon the basis of persistent azoospermia that was associated with low semen volume, absent fructose and normal hormonal levels, He had ultra-sound of his scrotal contents which demonstrated absent seminal vesicles and histology examination of his testicular specimen demonstrated intact spermatogenesis. Interestingly and incidentally, only his right testicular biopsy showed ova of two parasitic species of Schistosoma, namely Schistosoma haematobium which does infest the genitourinary tract and Schistosoma mansoni which does infest the gastrointestinal tract. Abdel-Naser et al. [30] iterated that both Schistosoma species are rare causes of azoospermia, and the case should be further managed as CBAVD in which the left testicle is considered the preferred site of sperm retrieval for assisted reproduction.
Hassan et al. [21] reported a case of testicular schistosomiasis in a 26-year-old unmarried Egyptian man who had manifested with slowly growing painless swelling within his right hemi-scrotum. He had various assessments including: Clinical examination, ultrasound scan of his scrotal contents, magnetic resonance imaging (MRI) scan, computerized tomography (CT) scan, urine examination and semen Zeihl-Neelsen stain, stool examination, serum alpha-fetoprotein test, FSH test, LH test, PRL test, E2 test, total testosterone (T) test, and surgical exploration. Hassan et al. [21] reported the results as follows: During his clinical examination, there was a large painless swelling found within his right hemi-scrotum with two hard masses felt subcutaneously. His trans-illumination test was negative and there was no evidence inguinal lymph node enlargement. Examination of the contents of his left hemi-scrotum demonstrated normal findings. The results of his serum alpha-fetoprotein, FSH, LH, total T, E2, and PRL were within normal ranges. His MRI scan did not demonstrate any masses of abnormal signal intensity or contrast-enhancement. He underwent -scrotal surgical exploration which revealed discharge of thick brownish red pus with presence of two hard extra-testicular scrotal masses. Histopathology examination of his right testis biopsy showed reduced diameter of the seminiferous tubules with marked hypo-spermatogenesis where the interstitium was filled by multiple Schistosoma mansoni ova that was associated with granulomatous reaction which had compressed the tubules. Hassan et al. [21] concluded that scrotal involvement in schistosomiasis with its variable presentations should be considered with regard to the diagnosis of scrotal masses, especially in Schistosomiasis endemic areas of the world.
Mortati et al. [31] reported a forty-year-old white man who had attended the outpatient clinic of their hospital in May 2003, who had complained about a nodule within his right testis. His wife found the nodule during a coital activity. His clinical examination demonstrated a painless 2-cm solid nodule within his right testicle. The results of his laboratory tests including beta-human chorionic gonadotropin (beta-HCG), lactic dehydrogenase (LDH), and alpha-feto protein (AFP) were all within normal range. He had ultrasound scan of his scrotal contents which demonstrated a 1.8 cm hypoechoic nodule within his right testis. He underwent frozen section excisional biopsy of his right testicular nodule. Frozen section pathology examination of the excised testicular nodule revealed a granulomatous lesion which was associated with Schistosoma egg (see figure 7). He was additionally treated with 40 mg/kg of praziquantel at single dose and after 10 months of follow-up, there is no evidence of the disease recurrence.
Perivasamy et al. [24] iterated the following:
Data from the WHO had stated that up to 85% of cases of human schistosomiasis are from Africa.
The common sites of this parasitic infection tend to be the intestine and urinary bladder.
Schistosomiasis of the testis is extremely rare but the number of reported cases of Schistosomiasis throughout the world has doubled over the preceding decade.
Perivasamy et al. [24] reported a case of Schistosomiasis of the testis of a Myanmar immigrant in Malaysia who had manifested with a 6-month history of progressively enlarging left testicular swelling. The results of his biochemical markers and cultures were not suggestive of an ongoing infection. In view of this a testicular malignancy was strongly suspected, for which, he underwent a left radical orchidectomy. Perivasamy et al. [24] reported that their clinical suspicion was proven wrong when the histopathology examination of the radical orchidectomy specimen revealed Schistosoma eggs with granulamatous tissue formation within the testis. He was subsequently treated with praziquantel. This short case summation should remind clinicians to have a high-index of suspicion for the possibility of Schistosomiasis of the testis as a differential diagnosis of an intra-testicular mass in individuals who have dwelt in or travelled to and returned from Schistosomiasis endemic areas of the world so that in such individuals who present with testicular masses so that they can be fully assessed for Schistosomiasis as well as during surgical operation of the testicular masses complete excision of the masses should be undertaken for frozen section histopathology examination of the specimen and if Schistosomiasis of the testis in the absence of a malignant testicular tumour then the rest of the testis can be saved / spared but when a malignant testicular tumour is found upon the frozen section examination then radical orchidectomy can be undertaken.
Yakubu et al. [32] reported a 40-year-old Nigerian man who was married with four children, and who was admitted to the Emergency Surgical Unit of Aminu Kano Teaching Hospital, Kano, Nigeria, who had presented with a 2-hour history of bilateral scrotal pain. The pain had suddenly commenced and the pain was very severe and dull in nature but the pain was not affected by movement or change in his posture. The patient had an associated frequency of micturition, but he did not have any dysuria, fever or haematuria. The patient did not have any past history of urethritis or trauma to the scrotum and he had not noticed any swellings within his groin or genital areas. Over the preceding one year, he had experienced recurrent mild episodes of scrotal pain which had been treated with analgesia and antibiotics at various private clinics. During his presentation he was found to be afebrile with a temperature of 36.6 DC. He was not pale. His pulse rate was 92/minute, and his blood pressure was 130/80 mmHg as well as his respiratory rate was 18/minute. Clinical examination of his abdomen was unremarkable and his hernial orifices were intact. His scrotal skin was warm and his testes were bilaterally swollen and tender with thickened spermatic cords. His left testicle was also found to be hard in consistency A provisional diagnosis of acute scrotum due to acute epididymo-orchitis was made and testicular torsion was considered as a differential diagnosis. He had an urgent laboratory work up and he was prepared for emergency exploration of his scrotum. The results of his laboratory investigations were summarised as follows: (a) His haemoglobin was 13.4 g/dL, while his blood cell count was 9.0x1 0 gIL. (b) His serum urea and electrolytes were within normal reference ranges and his urine microscopy demonstrated 0-2 pus cells/hpf. During his operation, his testes were found to be slightly enlarged and the left testis was firmer in consistency. His spermatic cords were found to be normal and no features were found that were suggestive of torsion. Biopsies of both testes were undertaken and submitted for histopathology laboratory for examination. Macroscopic examination of the biopsy specimens revealed that the specimens had measured 0.8 cm x 0.5 cm and 0.9 cm x 0.5 cm from the left and right testis, respectively. The biopsy specimens looked greyish brown and fibrous. Microscopy histopathology examination of the biopsy specimens of the testes showed atrophy of the seminiferous tubules as well as several Schistosoma haematobium ova. Encompassing granulomatous inflammation that consisted of epithelioid celis, lymphocytes and giant cells was found as well as areas of fibrosis. The features of the biopsy specimens were more marked on the left side. The patient did have a good postoperative recovery and he was commenced on antibiotics and analgesics. He received Praziquantel (40mg/kg body weight) on the fourth postoperative day based upon the histopathological findings of his testicular biopsy specimens. The patient’s scrotal pain as well as his testicular swelling gradually resolved and he was discharged home on the seventh postoperative day. His subsequent follow up in the outpatient clinic did demonstrate a satisfactory recovery. During his one year follow up assessment. The patient was found to be fine with his wife expecting a new baby. The lesson that needs to be learnt from this case report, is that even though very rare, Schistosomiasis of the testis could bilateral as well as it could present as an acute intra-scrotal/intratesticular pain that may simulate epididymo-orchitis and / torsion of the testis.
Sinha et al. [33] reported a 32-year-old man who had been dwelling within Faridabad, in India, who had manifested with a painless swelling within his right hemi-scrotum for one week which had been increasing in size gradually. He had never travelled abroad before. His clinical examination demonstrated a swelling that measured about 3 cm x 2 cm within his right epididymis that was non-tender as well as cystic with regard to its consistency. He had ultrasound scan of his scrotal contents which demonstrated an ill-defined echogenic lesion that measured about 31 mm x 12 mm with a small, central hypo-echoic area that measured about 7.5 mm x 5 mm within the right spermatic cord just above the level of his right epididymis. He underwent excision of the epididymal cyst. Histopathology examination of the excised epididymal cyst demonstrated fibroadipose tissue with eggs of Schistosoma encompassed by an abundant inflammatory infiltrate which was composed of foamy cells, eosinophils, as well as polymorphs (see figure 8). His post-operative recovery was unremarkable and he was treated also with a single dose of praziquantel.
Sinha et al. [33] made the ensuing iterations:
At the time of their case report, only three cases of Schistosoma epididymitis and 12 cases of Schistosomiasis of the testis had been reported in the world [26, 34].
In 2004, Alves, Assis, and Rezende [35] had reported a case of Schistosomiasis of epididymis in a 32-year-old man. The patient had manifested with scrotal pain as well as a tender, hard left epididymis. He underwent left epididymectomy and pathology examination of the excised epididymis showed eggs of Schistosoma mansoni.
Okani et al. [36] did report a case of a 12-year-old boy who had a left testicular mass, which upon exploration was found to be a hard mass that was adherent to the epididymis. Pathology examination of the biopsy specimen of the mass demonstrated chronic granulomatous inflammation around calcified Schistosoma haematobium eggs.
Honare and Coleman, [34] did report a case of a 54-year-old Canadian man who had manifested with a painless swelling of his right testis. Pathology examination of biopsy specimen of the mass demonstrated features of Schistosomiasis caused by Schistosoma haematobium.
El-Hawany and Foda [37] had published five cases of Schistosomiasis in 2016 in which they had found Schistosoma eggs within the testis, prostate gland, and seminal vesicles.
Joshi [38] reported a 10-year-old boy who had presented with a slowly growing painless swelling of his right hemi-scrotum. Based upon a suspicion of a right-sided seminoma of testis, a right radical orchidectomy was undertaken. Pathology examination of the specimen showed ova of Schistosoma which was at different stages of degeneration and calcification.
Al-Qahtani and Droupy [26] did report a 31-year-old man who had primary infertility for nine years and who had a right-sided testicular mass. He underwent scrotal exploration and frozen section pathology examination of a specimen of the mass showed evidence of Schistosomiasis.
Praziquantel is the treatment option of choice for Schistosomiasis. A single dose of 40mg/kg is an efficacious treatment.
Other medicaments that could be utilized include: metrifonate, oxamniquine, and artemisinin-derivatives (artesunate and artemether).
Schistosomiasis of the epididymis is an uncommon disease.
Schistosomiasis could manifest as swelling of the epididymis which could be diagnosed following histological examination of resected specimen.
Praziquantel is the treatment of choice.
A lesson that needs to be learnt from this case report is the fact that it is important to submit all excised intra-scrotal specimens for histopathology examination otherwise important diagnoses could be missed if specimens of presumed epididymal cysts and other excised intra-scrotal excised specimens are not sent for histopathology examination.
Schistosomiasis of the testis and scrotal contents are very rare but they reported sporadically in different parts of the word including Schistosomiasis endemic as well as non-endemic parts of the world.
Schistosomiasis of the testis and scrotal contents do mimic more common lesions within the scrotum including malignant testicular tumour or tumour of the epididymis and because of this radical orchidectomy has been undertaken on a number of previous occasions based upon a provisional diagnosis of malignant testicular tumour only to realise pursuant to histopathology examination of the radical orchidectomy specimen only to find the lesion was Schistosomiasis which could have been treated by excision of the lesion only and preservation of the testis in association with utilization of anti-Schistosomiasis medicament.
If a high index of suspicion for Schistosomiasis of the testis is exercised with regard to cases of testicular and intra-scrotal masses that are found in children and adults who dwell in Schistosomiasis-endemic areas as well as in individuals who have travelled to and returned from Schistosomiasis-endemic areas of the world as well as if there is a history of visible haematuria, it would be advised that during surgery to excise the lesion within the scrotum, radical orchidectomy should not be undertaken straight away but instead, biopsy/complete excision of the lesion/mass should be undertaken for frozen section histopathology examination and if there is evidence of Schistosomiasis in the absence of a malignant lesion then a testis sparing surgery should be undertaken and an anti-Schistosoma medication be given. On the other hand if there is evidence of a malignant tumour within the testis or scrotum, then radical orchidectomy or radical excision of the intra-scrotal mass should be undertaken.
All excised intra-scrotal lesions inkling epididymal cysts, epididymal tumours, hydrocele tunica sacs as well as all other excised intra-scrotal masses should be sent for histopathology examinations so that an accurate diagnosis could be made which would help surgeons plan appropriate treatments for their patients and if Schistosomiasis is diagnosed, then anti-Schistosomiasis medicament can be given.
None
Acknowledgements to:
The Pan African Medical Journal for granting permission for reproduction of figures and contents of their Journal article under copyright Copyright © Olubanji Ajibola Oguntunde et al. The Pan African Medical Journal - ISSN 1937-8688. This is an Open Access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case Reports in Infectious Diseases and Hindawi Publishing for granting permission for reproduction of contents and figures from their journal articles under Copyright: Copyright © 2011 Peter F. Rambau et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Brazilian Journal of Urology and the Brazilian Society of Urology, for granting permission for reproduction of contents and figures from their journal articles under Creative Comments Attribution License provided the original authors and the source are properly cited.
Cureus for granting permission for reproduction of figures and contents of their Journal article under Copyright: Copyright © Copy right 2019 Sinha et al. This is an open access article distributed under the terms of the Creative Commons Attribution License CC-BY 3.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
