
Case Report | DOI: https://doi.org/10.31579/2690-4861/352
1 Pulmonology Service, La Princesa Research Institute (IIS Princesa), La Princesa University Hospital, Madrid, Spain.
2 Department of Medicine. Autonomous University of Madrid, Madrid, Spain.
3 Virology Unit, PharmaMar, SA, Madrid, Spain.
*Corresponding Author: Pedro Landete, Pulmonology Service, La Princesa Research Institute (IIS Princesa), La Princesa University Hospital, Madrid, Spain.
Citation: Landete P., Valenzuela C., Hevia M., Lloris R., María P. Pire, et al., (2023), SARS-CoV-2-Related Persistent Pulmonary Affection Case in A 55-Year-Old Gastric MALT Lymphoma Patient on Rituximab, International Journal of Clinical Case Reports and Reviews, 15(2); DOI:10.31579/2690-4861/352
Copyright: © 2023, Pedro Landete. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 November 2023 | Accepted: 29 November 2023 | Published: 05 December 2023
Keywords: plitidepsin; COVID-19; immunocompromised patients; MALT lymphoma; persistent viral SARS-CoV-2 replication; SARS-CoV-2
Following a mild symptomatic SARS-CoV-2 infection, a 55-year-old patient with gastric MALT lymphoma, currently treated with rituximab, experienced persistent symptoms. Over subsequent months, the patient exhibited low-grade fever, dyspnea, and progressive desaturation, leading to respiratory failure necessitating home oxygen therapy. A PCR test confirmed SARS-CoV-2 infection, prompting suspicion of persistent COVID-19. Imaging and biopsy results were consistent with cryptogenic organizing pneumonia (COP), but the patient showed no response to treatment, including corticosteroids and immunosuppressants. Remdesivir treatment yielded partial improvement but failed to achieve full resolution. Plitidepsin (2.5 mg/day for 3 days) under compassionate use led to negative PCR tests and normal respiratory function restoration within 3 days after treatment. SARS-CoV-2's impact on immunocompromised patients is concerning due to unique clinical features, challenges in viral clearance and immunization, and varied responses to approved treatments. A phase II clinical trial is underway to assess plitidepsin's efficacy in immunocompromised COVID-19 adults requiring hospital care.
adverse event (AE); computed tomography (CT); coronavirus disease 2019 (COVID-19); C-reactive protein (CRP); cryptogenic organizing pneumonia (COP); diffusing capacity of the lungs for carbon monoxide (DLCO); eukaryotic elongation factor 1A (eEF1A); half maximal inhibitory concentration (IC50); immunoglobulin G (IgG); left upper lobe (LUL); liters per minute (LPM); mucosa-associated lymphoid tissue (MALT); polymerase chain reaction (PCR); right upper lobe (RUL); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Hematological cancer patients face an elevated risk of clinical severity, and mortality upon contracting severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1-3]. Furthermore, hematological cancer patients exhibit prolonged viral shedding, sustained immune dysregulation, and diminished seroconversion compared to those with solid cancers [2,4].
The use of immunotherapy has also been linked to more severe outcomes and a higher cytokine storm risk [5,6]. Therefore, potent antivirals capable of clearing the viral infection are essential for managing hematological cancer patients [6]. Preclinical pharmacology studies demonstrate that plitidepsin, a marine-derived cyclic peptide targeting eukaryotic elongation factor 1A (eEF1A), is a potent inhibitor of SARS-CoV-2 growth in vitro, with half maximal inhibitory concentration (IC50) in the nanomolar range across different SARS-CoV-2 variants [7].
The safety and toxicological profile of three doses of plitidepsin (1.5, 2, and 2.5 mg/day for three days) were assessed in a multicenter, randomized clinical trial involving 46 hospitalized adult COVID-19 patients (APLICOV-PC, ClinicalTrials.gov Identifier: NCT04382066). Plitidepsin treatment was well-tolerated, with only two grade 3 treatment-related adverse events (AEs): hypersensitivity and diarrhea [8]. Plitidepsin's tolerability as a rescue treatment has also been demonstrated in 33 immunocompromised patients with persistent COVID-19 who were unsuitable for other antiviral treatments [9].
This case report provides a comprehensive clinical and evolutionary overview of an immunocompromised patient with persistent COVID-19, highlighting the treatment approach involving plitidepsin.
We present the case of a 55-year-old male with medical history of low-grade gastric mucosa-associated lymphoid tissue (MALT) B-cell lymphoma diagnosed in 2019 and treated with rituximab and bortezomib, achieving complete remission in 2020 and undergoing bimonthly rituximab maintenance treatment (last dose in June 2022). He was diagnosed with Waldenström macroglobulinemia, without a treatment indication.
In April 2022, mild SARS-CoV-2 infection was detected, which resolved spontaneously without hospitalization or further testing. In May 2022, the patient experienced intermittent low-grade fever and associated mild dyspnea, without additional symptoms. Due to suspected bacterial infection in the ear-nose-throat region, antibiotic treatment was initiated with no evident symptom resolution. In June 2022, persistent low-grade fever led to a medical consultation. A chest computed tomography (CT) scan revealed widespread bilateral lung infiltrates, particularly accentuated in both upper lobes and predominantly on the right side, consistent with cryptogenic organizing pneumonia (COP). Prednisone treatment at 60 mg/day was initiated [10]. After 10 days, fever and dyspnea subsided, and the prednisone dosage was reduced to 30 mg/day. Two days later, slightly elevated erythrocyte sedimentation rate and C-reactive protein (CRP) levels were observed without symptom recurrence, prompting further reduction to 20 mg/day.
In August 2022, the patient again presented with low-grade fever and exertion-induced dyspnea. Due to symptom recurrence upon prednisone dosage reduction, a repeat chest CT scan (August 2022) revealed worsening radiological findings, including significant infiltrates in the right upper lobe (RUL), patchy infiltrates bilaterally in mid and lower lung fields with peripheral and subpleural distribution, some showing air bronchograms, and one with a reversed halo sign in the anterior margin of the left upper lobe (LUL), still consistent with COP. Prednisone dosage was increased again to 60 mg, but the patient's clinical condition progressively worsened to dyspnea at minimal exertion. Another chest CT scan (October 2022) displayed worsening radiological results, including extensive infiltrates in the RUL, scattered infiltrates seen bilaterally in mid and lower lung fields with peripheral and subpleural distribution, some tending to alveolar coalescence, especially in RUL, and laminar atelectasis in the LUL, middle lobe, and lingula.
Despite high-dose corticosteroid treatment, clinical and radiological deterioration prompted a core needle biopsy in November 2022. Pathological findings indicated alveolar septal thickening with mild fibrosis and moderate chronic inflammation, consistent with COP within the context of corticosteroid treatment. An echocardiogram yielded no significant abnormalities, while a positron emission tomography-CT indicated the presence of inflammatory pathology. A bronchoscopy with cryobiopsy led to an organized pneumonia diagnosis. Following consultation with the Diffuse Interstitial Lung Disease Committee, mycophenolate mofetil (500 mg/12 h) was added to the ongoing 60 mg prednisone treatment [10]. Spirometry —diffusing capacity of the lungs for carbon monoxide (DLCO) 42%, forced expiratory volume in 1 second (FEV1) 68%, forced vital capacity (FVC) 73%— indicated a restrictive pattern with impaired diffusion. A 6-minute walk test revealed initial oxygen saturation of 87 percentage decreasing to 74%. Nocturnal home oxygen therapy was initiated due to baseline saturations around 75%.
On December 26th, 2022, the patient presented to the Emergency Department with worsening symptoms, including a basal saturation of 84%, tachypnea, and labored speech. Fine crackles up to bilateral mid-lung fields were observed upon examination, while the patient remained afebrile. Laboratory results indicated leukocytosis (13.17 x103/mm3) with neutrophilia (12.20x103/mm3), lymphopenia (0.46x103/mm3), and elevated CRP (3.95 mg/dL). Suspecting persistent SARS-CoV-2 infection, a nasopharyngeal PCR test was performed, yielding a positive result (CT Less than 30), while SARS-CoV-2 immunoglobulin G (IgG) serology testing was negative (Table 1). A repeat CT scan demonstrated a deterioration compared to previous scans (Figure 1).
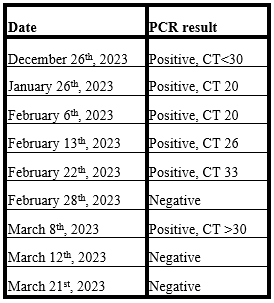
Table 1: PCR results and dates.

Figure 1: High-resolution Computed Tomography (December 27th, 2022).
Given the active infection, mycophenolate was discontinued, and the patient received five-day course of remdesivir (December 26th-30th, 2022) followed by another five days of remdesivir along with a single sotrovimab infusion (January 2nd-7th, 2023) [11]. This treatment led to clinical improvement, with increased resting and exertion saturations and alleviation of low-grade fever. However, the need for 16-hour daily home oxygen therapy persisted, particularly during ambulation. Mindful of ongoing respiratory insufficiency —saturations at 93-94% with effort and nasal cannula at 3 liters per minute (LPM)—, a PCR test was repeated eight weeks post-treatment (March 8th, 2023), yielding a positive result (CT >30, see Table 1).
No lymphadenopathy or other significant findings are observed in the mediastinum or lung hilum, while there is extensive bilateral involvement in the lung parenchyma (red arrows). Predominant areas of ground-glass opacities, both centrally and peripherally located can be observed (blue arrows). Scattered alveolar infiltrates and linear images forming arches parallel to the pleural surface (yellow arrow). No pleural effusion is detected.
Considering the persistent positive PCR result and the lack of clinical improvement, compassionate use of plitidepsin was requested and administered for three days at a dose of 2.5 mg, along with appropriate premedication (March 8th-10th, 2023). A follow-up PCR on March 21st indicated a negative result, prompting a reevaluation (Table 1). The patient's basal oxygen saturations normalized without desaturation during exertion, leading to the discontinuation of home oxygen therapy. Plitidepsin was well tolerated with no AEs reported. Prednisone treatment was tapered off. A subsequent chest X-ray displayed no significant findings, and a control CT scan is scheduled for December 2023. Subsequently, the patient remained asymptomatic, free of oxygen therapy, with no new COVID-19 episodes, consistently testing negative by nasopharyngeal swab PCR (7 months follow-up). Regular check-ups for the underlying disease have been conducted without further complications.
Contributors to prolonged viral replication and inadequate clearance in patients with hematological neoplasms are inherent immune defects related to their primary disease and/or resulting from antitumoral therapies [12,13]. Additionally, subacute, or chronic COVID-19 pneumonia can lead to persistent lung damage and viral escape phenomena [14].
Suppression of viral replication in hematological cancer patients is crucial not only due to their elevated risk of complications but also to prevent de novo mutations resulting from persistent viral replication, coupled with the emergence of resistance to available antivirals [15].
There are currently no established clinical guidelines for managing persistent SARS-CoV-2 viral replication in rituximab-treated patients. Moreover, this patient population is underrepresented in COVID-19 clinical trials, resulting in varying treatments reported in the literature [16-22].
Despite the obvious limitation of describing only one patient, our case highlights the potential utility of plitidepsin as a promising antiviral therapy for immunocompromised patients with persistent SARS-CoV-2 infection, particularly those with hematological malignancies. Further research in larger cohorts and controlled clinical trials are essential to establish the efficacy, safety, and optimal usage of plitidepsin in this patient population. A phase II study assessing the efficacy of plitidepsin in immunocompromised COVID-19 adult patients requiring hospital care (NEREIDA, ClinicalTrials.gov Identifier: NCT05705167) is ongoing.
In patients with compromised immune systems, clinical manifestations of SARS-CoV-2 infection can mimic pulmonary interstitial diseases, with the virus persisting for months, sometimes despite antiviral treatments. In such cases, it is crucial to suspect and rule out the presence of SARS-CoV-2 in the respiratory tract and achieve viral clearance to prevent viral reactivations in high-risk patients. The compassionate use of plitidepsin in a high-risk patient with prolonged SARS-CoV-2 infection was well-tolerated and associated with PCR negativity, along with sustained symptomatic resolution. The development of new antivirals for COVID-19 in high-risk patients is imperative.
We thank the patient, and his relatives, for their generosity in allowing the publication of the patient’s data as a case report.
We obtained institutional written consent from the patient for publication of his data under anonymized format.
PL conceived the initial study concept, formulated the case report, conducted the diagnosis, oversaw patient care and ongoing monitoring, collected patient data, and played a pivotal role in both drafting and critically reviewing the article for its intellectual content.
CV; MH performed the diagnosis, management and regular follow-up of the patient.
RL; MPP analyzed patient data, undertook the writing and editing processes, and contributed scientific guidance along with a thorough review of the article's intellectual content.
XELE provided scientific, administrative, and logistic support.
ES gathered and analyzed patient data, conducted the writing and editing tasks and contributed scientific assistance, including a meticulous review of the article’s intellectual content.
The current manuscript has been reviewed and agreed upon by all authors.
ES and MPP are full-time employees of PharmaMar, S.A (Madrid, Spain).
XELE and RL are full-time employees and shareholders of PharmaMar, S.A (Madrid, Spain).
All remaining authors have declared no conflicts of interest.
This study has been funded by Pharmamar, SA (Madrid, Spain).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
