
Research Article | DOI: https://doi.org/10.31579/2639-4162/247
Retired Urologist and Clinician, Reviewer of Articles for Journals, Medical Examiner Member of Royal College of Pathologists, London. United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, Retired Urologist and Clinician, Reviewer of Articles for Journals, Medical Examiner Member of Royal College of Pathologists, London. United Kingdom.
Citation: Grey Venyo AK (2025), Sarcoidosis of Urinary Bladder an Update, J. General Medicine and Clinical Practice, 8(1); DOI:10.31579/2639-4162/247
Copyright: © 2025, Anthony Kodzo-Grey Venyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 December 2024 | Accepted: 17 January 2025 | Published: 28 January 2025
Keywords: sarcoidosis of urinary bladder; vesical sarcoidosis; sarcoidosis of the spine; biopsy; cystoscopy; high index of suspicion; neurogenic bladder; computed tomography scan; contrast-enhancement; urodynamics
Sarcoidosis is a multi-system granulomatous disease that is characterized by non-caseating epithelioid granulomas in association with clinical and radiological findings. The cause of sarcoidosis disease is still not certain. Recent findings had indicated that sarcoidosis is related to a chronic immune response which is caused by exposure to common environmental factors such as Propionibacterium or airborne organic or inorganic material, as well as most probably a sum of several immune system and environmental factors. Sarcoidosis affects all races and genders; nevertheless, women are 30% more likely to be affected in comparison to men and African-Americans (36/100.000) are more commonly affected than Caucasians (11/100.000) Within Europe the incidence of sarcoidosis is higher in northern countries, 20-40/100.000 at general, up to 121/100.00 in Sweden and lower in southern countries like England (5/100.000) and Spain (1.36/100.000). Japan had a reported prevalence of 0.3-1.7/100.000. It has been iterated that genetic propensity might explain the heterogeneity at appearance and the severity of the cases in different ethnic groups and races. Sarcoidosis, is usually not regarded to be a urological disease, in that sarcoidosis afflicts mostly the lungs and lymph nodes. For that reason, sarcoidosis may be overlooked when it afflicts the urinary tract. Nevertheless, urinary impairment of the disease is not rare and may lead to conditions treated by the urologist such as nephrolithiasis, lower urinary tract symptoms and urinary retention as well as recurrent urinary tract infections and haematuria. Moreover, sarcoidosis of the urinary bladder and sarcoidosis of other urinary tract organs may also produce clinical manifestations that could simulate urological disorders such as testicular nodules, renal masses, or even PET positive lymphadenopathy, leading to misinterpretations of early-stage urological malignancies, including urinary bladder cancer and urothelial tumour of the ureter causing ureteric obstruction. Sarcoidosis could affect the urinary bladder alone and cause various non-specific symptoms that simulate the manifestations of more common conditions affecting structures and organs that encompass the urinary bladder or sarcoidosis of the urinary bladder may be part of systemic sarcoidosis. Sometimes a patient may have urinary bladder symptoms that emanate from affections of nerves that supply the urinary bladder even though the urinary bladder may be found to be normal upon cystoscopy and radiology imaging but the symptoms would be proven on urodynamics studies to be related to detrusor-sphincter dyssynergia emanating from neuro-sarcoidosis and sarcoidosis of the spine. Diagnosis of sarcoidosis of the urinary bladder can be established based upon the histopathology examination features of biopsy specimens of the urinary bladder lesion.
It has been iterated that sarcoidosis had traditionally been regarded as a pulmonary disease, which primarily afflicts young African-American females. [1] It has been pointed out that contemporary epidemiology evidence had indicated that, in fact, African-Americans have 3 to 4 times increased risk of developing sarcoidosis, which is considerably <10>
It has been iterated that sarcoidosis was first described and named by Boeck in 1899 and that the name was chosen because of its close appearance, both on a gross and histopathology level, to that of sarcoma. [1] [6] It has also been iterated that since its early description, concepts of the sarcoidosis disease had broadened from those of a primary dermatology disorder to those of a systemic disease that afflicts all organ systems. It has been stated that one review had demonstrated that 16.6% of sarcoidosis patients had extrapulmonary presentations of the disease.[1] [7] It had also been pointed out that in another review, which had evaluated 1254 cases of histologically-proven sarcoidosis, Mayock et al. [8] found one case of adrenal involvement, 54 (4.3%) cases of renal involvement, and six (1%) cases of epididymal involvement. Other involved GU organs were not delineated. They also found that the patients were 37% male and 63
Internet databases were searched including: Google; google scholar; yahoo; and PUBMED. The search words that were used included: Sarcoidosis of the bladder; urinary bladder sarcoidosis; and vesical sarcoidosis. Fifty-four (54) references were identified which were used to write the chapter on sarcoidosis of the urinary bladder which has been divided into two parts: (A) Overview, and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to sarcoidosis of the urinary bladder.
Results
[A] Overview
Definition, General statements, Practice Essentials. [11]
Sarcoidosis has been defined as a multi-system inflammatory disease of unknown aetiology which predominantly affects the lungs and intrathoracic lymph nodes and is manifested by the presence of non-caseating granulomas (NCGs) within afflicted organ tissues of the body. [11]
Signs and symptoms
The presenting signs and symptoms in sarcoidosis are stated to vary depending upon the extent and severity of the organ which is involved by sarcoidosis as follows: [11] [12]
The pulmonary findings on physical examination of patients affected by sarcoidosis had been summarized as follows: [11]
It has been stated that dermatology manifestations of sarcoidosis may include the following: [11]
It has been iterated that ocular involvement, in cases of sarcoidosis which may lead to blindness if untreated, may present as follows: [11]
Other possible presentations of sarcoidosis do include the ensuing: [11]
Diagnosis
The radiology-image studies for sarcoidosis had been summarized as follows: [11]
Staging of sarcoidosis had been summated as follows: [11]
It has been stated that pulmonary function tests and a carbon monoxide diffusion capacity test of the lungs for carbon monoxide (DLCO) are used routinely in evaluation and follow-up of individuals afflicted by sarcoidosis, [11] and that some of the possible findings of the tests do include the following: [11]
Routine laboratory evaluation is stated to be often unrevealing, but possible abnormalities include the following: [11]
Management
The management of sarcoidosis has been summarized as follows: [11]
It has been iterated that non-steroidal anti-inflammatory drugs (NSAIDs) are indicated for the treatment of arthralgias and other rheumatic complaints. [11] It has also been stated that patients with stage I sarcoidosis often do require only occasional treatment with NSAIDs. [11]
Treatment in sarcoidosis patients with pulmonary involvement has been summated as follows:
For extrapulmonary sarcoidosis involving such critical organs such as the heart, liver, eyes, kidneys, or central nervous system, corticosteroid therapy is stated to be indicated. [11] It has been iterated that topical corticosteroids are effective for ocular disease. [11] For pulmonary sarcoidosis disease, it has been iterated that prednisone is generally given daily and then tapered over a 6-month course. It has also been stated that high-dose inhaled corticosteroids could be an option, particularly in sarcoidosis patients with endobronchial disease.
Common indications for non-corticosteroid agents in cases of sarcoidosis had been stated to include the ensuing: [11]
Non-corticosteroid agents that tend to be used in sarcoidosis include the ensuing: [11]
It had also been iterated that for sarcoidosis patients with advanced pulmonary fibrosis from sarcoidosis, lung transplantation remains the only hope for long-term survival and that indications for transplantation include either or both of the following. [28]:
[B] Miscellaneous Narrations and Discussions from Sarcoidosis of The Urinary Bladder
Droessler et al. [29] reported a 33-year-old African American female, who was a former smoker, who had presented in the emergency room (ER) with a 1-month history of recurrent urinary tract infections (UTI), severe dysuria, visible haematuria, a painful vagina, and increasing difficulty emptying the bladder. She had been seen by an outpatient gynaecologist in the previous month and she was diagnosed with a UTI, which was confirmed by dipstick urinalysis and microanalysis, and which was treated with ciprofloxacin. It was noted during that visit that there was an abnormal palpable mass of the urethra, and she was referred to a urologist. She did not follow up with a urologist, and over the next month the periurethral pain gradually worsened, despite antibiotic treatment, which prompted her to go to the ER. She had a history of sarcoidosis, which was diagnosed 4 months earlier via the undertaking of bronchoscopy and mediastinal lymph node biopsy, but she was not undergoing treatment and was being monitored by a respiratory physician and nephrologist. Her family history was significant for sarcoidosis in her sister and breast cancer in her maternal aunt.
Hayashida, et al. [30] made the ensuing iterations:
Hayashida, et al. [30] reported a 60-year-old man, who presented with anorexia and weight loss. His blood tests showed renal dysfunction and hypercalcemia. He had computed tomography scan which showed left hydronephrosis which was associated with left lower ureteral wall thickening, which demonstrated high signal intensity upon diffusion-weighted magnetic resonance imaging. Similarly, Hayashida, et al. [30] identified a urinary bladder tumour during cystoscopy, and a 2-cm-long stenosis which was demonstrated by retrograde ureterogram; therefore, ureteral cancer was suspected. Meanwhile, taking into consideration the clinical implication of hypercalcemia, a differential diagnosis of sarcoidosis was established based upon elevated levels of sarcoidosis markers. Fluorodeoxyglucose positron emission tomography demonstrated fluorodeoxyglucose accumulation in the left lower ureter, skin, and muscles, indictive of ureteric sarcoidosis with systemic sarcoid nodules. For a definitive diagnosis, transurethral resection of the bladder tumour (TURBT) and ureteroscopy biopsy were undertaken. Histopathology examination of the specimens revealed ureteric sarcoidosis with bladder urothelial carcinoma. Following an oral administration of prednisolone, his hypercalcemia instantly resolved, the renal function immediately improved, and the left ureteral lesion showed complete resolution with no recurrence.
Hayashida, et al. [30] made the ensuing conclusions
La Rochelle et al. [31] described the urological manifestations of sarcoidosis and how the disease may affect the management of multiple urological conditions. La Rochelle et al. [31] undertook a PubMed® search using the query sarcoidosis and multiple urological terms. La Rochelle et al. [31] reported the ensuing results:
La Rochelle et al. [31] made the ensuing conclusion and advise:
Tammela et al. [32] reported a case of sarcoidosis of the urinary bladder in a woman with a known systemic involvement. The sarcoidosis lesion improved and her ureteral obstruction was relieved after transurethral resection and systemic corticosteroid treatment. Tammela et al. [32] concluded that sarcoidosis and malacoplakia are believed to represent distinct disease processes in the bladder.
Fukutani et al. [33] reported a 75-year-old woman with transitional cell carcinoma of the renal pelvis, who was revealed to have sarcoid granulomas within the kidney as well as in the renal pedicle lymph nodes. In addition, non-caseating granulomas had been found within the pelvic lymph nodes in a histological study following previous total cystectomy for urinary bladder cancer.
Sakakibara et al. [34] reported a case of neuro-sarcoidosis in which urodynamic studies had demonstrated neurogenic bladder dysfunction. Sakakibara et al. [34] reported a 30-year-old man, who began to have slowly progressive gait ataxia of vestibular origin, deafness, and hallucination, which developed into seizure and stupor. He had computed tomography scan of his brain and magnetic resonance imaging scan which demonstrated an anteromedial frontal lobe lesion with mild ventricular enlargement. His cerebrospinal fluid examination revealed pleocytosis with raised total protein and angiotensin-converting enzyme levels. He had endoscopic lung biopsy and pathology examination of the biopsy specimen demonstrated epithelioid granuloma. He took oral prednisolone (60 mg/day) medication, which ameliorated his symptoms. After tapering his steroids, however, he developed urinary urgency, frequency, urge urinary incontinence, and a relapse of gait ataxia. He had urodynamic study which demonstrated detrusor hyperreflexia. Prednisolone treatment again improved his urinary and neurological symptoms. Sakakibara et al. [34] concluded that:
Chouaib et al. [35] reported a case of spinal cord sarcoidosis in which urodynamic studies had demonstrated neurogenic bladder dysfunction. Chouaib et al. [35] reported a 56-year-old Caucasian woman, who developed progressive weakness of both lower extremities causing walking disturbance. Two months subsequently, she became unable to walk, and she gradually developed urinary urgency, nocturnal urinary frequency, and urge urinary incontinence. She had spinal MRI scan, which disclosed dorsal lesion, with atrophy of the cervical cord; she also had brain MRI scan which was normal. Her cerebrospinal fluid (CSF) upon analysis demonstrated elevated proteins. Her level of serum angiotensin-converting enzyme (ACE) level was moderately high. Her tuberculin skin test was negative. She had a scan of her thorax and abdomen and pelvis which demonstrated showed a suspicious lesion within her liver. She had draining-biopsy of the liver lesion and pathology examination of the specimen demonstrated non-caseating epithelioid granuloma. It was adjudged that the aforementioned finding had confirmed the diagnosis of spinal cord sarcoidosis. She urodynamic study which demonstrated detrusor hyperreflexia. She received prednisolone treatment, which improved her urinary and neurological symptoms. Chouaib et al. [35] concluded that:
Osanami et al. [36] made the ensuing iterations:
Osanami et al. [36] reported a 66-year-old man, who developed sudden urinary retention and fever. He was diagnosed with prostatitis and admitted to the hospital of Osanami et al. [36] An indwelling urethral catheter was inserted, and antimicrobial therapy was commenced; nevertheless, the prostatitis was refractory. He had computed tomography scan, which showed enlarged mediastinal lymph nodes. Analysis of trans-bronchoscopy lymph node and prostate biopsies demonstrated epithelioid cell granulomas, indicating systemic sarcoidosis. During the clinical course, his serum creatinine level rapidly increased to 2.36 mg/dL without oliguria. A kidney biopsy was undertaken and pathology examination of the biopsy specimen showed tubulointerstitial injury with moderate lympho-histiocytic infiltration and small-vessel vasculitis within the interstitium. Following oral administration of 60 mg/day prednisolone, the patient’s renal function immediately improved, and his urinary retention did not recur.
Osanami et al. [36] made the ensuing conclusions:
Upon reflection, a lesson that needs to be appreciated or learnt from this case report, is that a patient may at times be afflicted by sarcoidosis affecting a different organ and not the urinary bladder directly but the patient may manifest with lower urinary tract symptoms including urinary retention.
Hanif et al. [37] made the ensuing iterations:
Hanif et al. [37] reported a 55-year-old African American male, who had a medical history of substance use, cerebrovascular accident, hepatitis B, and who was recently diagnosed with right lower extremity deep venous thrombosis on anticoagulation and who had presented to the hospital with complaints of dizziness, blurry vision and left-sided weakness of one-day duration. It was noted that the patient had had many emergency department visits within the preceding one month for similar left-sided leg pain and falls. He had been treated for cellulitis and pain. This time he underwent computed tomography (CT) scan of the brain which demonstrated large areas of white matter hypodensities in bifrontal lobes as well as small areas of cortical hypodensities in the right anterior-inferior frontal lobe (see figure 1).

Figure 1:
CT scan of the brain (axial view), on arrival, demonstrating large areas of white matter hypodensities in the bifrontal lobes as well as small areas of cortical hypodensities in the right anteroinferior frontal lobe (arrows). Reproduced from: [37] under the Creative Commons Attribution License.
This was initially concerning for acute infarct versus subacute post-traumatic changes, which were the differential diagnose. Other possible differentials included: reversible posterior leukoencephalopathy or neoplastic process given the local mass effect. His neurological examination was non-focal and his cranial nerves II-XII were intact. A painful range of motion was identified in his lower extremity; nevertheless, his muscle strength was found to be 5/5. Additional findings upon his clinical examination included bilateral lower
extremity oedema left more than right, oral thrush and right axillary lymphadenopathy. The stroke protocol was commenced, and he was admitted to the hospital. Neurology and Haematology Oncology services were consulted for further assessment. He had magnetic resonance imaging (MRI) scan of the brain with contrast, which demonstrated extensive contrast-enhancing dural nodularity along bilateral frontal convexities and anterior falx associated with extensive nodular leptomeningeal enhancement along the bilateral frontal lobes, suprasellar cistern, right sylvian fissure, and right basal ganglia with associated extensive bilateral frontal vasogenic oedema and mass effect on lateral ventricles (see figures 2, and 3).
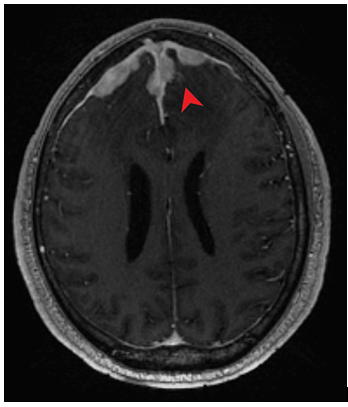
Figure 2:
Axial T1-weighted MRI of the brain with contrast showing extensive enhancing dural nodularity along bilateral frontal convexities and anterior falx (red arrow). Reproduced from: [37] under the Creative Commons Attribution License.
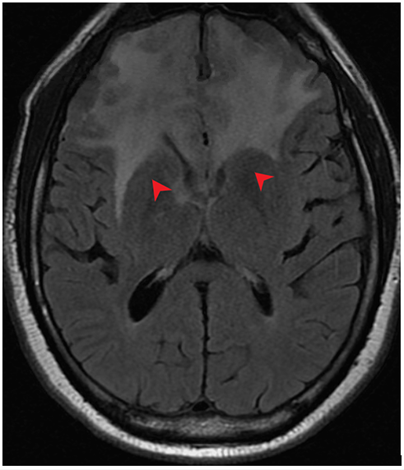
Figure 3:
Axial T1-weighted MRI of the brain with contrast revealing extensive nodular leptomeningeal enhancement along the bilateral frontal lobes, suprasellar cistern, right Sylvian fissure, and right basal ganglia with associated extensive vasogenic oedema extending to the lateral ventricles (red arrows). Reproduced from: [37] under the Creative Commons Attribution License.
The differential diagnoses were narrowed down to central nervous system (CNS) lymphoma versus neuro-sarcoidosis. In view of concerns of CNS
lymphoma, steroids were initially withheld pending the results of his cerebrospinal fluid (CSF) analysis. He underwent CT scan of the thorax without contrast which demonstrated sub-centimetre mediastinal, bilateral hilar, and right axillary lymphadenopathy (see figure 4). A core needle biopsy of the largest axillary lymph node was undertaken and pathology examination of the biopsy specimen demonstrated benign and reactive areas. There was an insufficient sample for flow cytometry to be undertaken.
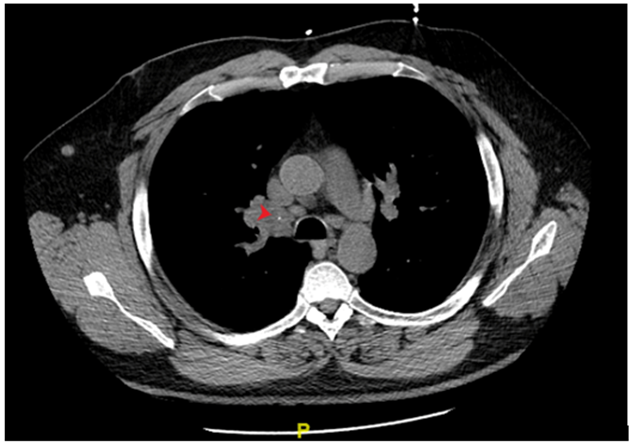
Figure 4:
Axial view of chest CT without contrast showing calcified right hilar adenopathy (arrow). Reproduced from: [37] under the Creative Commons Attribution License.
He underwent CT scan of the abdomen and pelvis with contrast for further assessment of lymphadenopathy which identified a 2.6-cm urinary bladder wall tumour, which was concerning for neoplasm. There was also bilateral iliac chain and retroperitoneal adenopathy which was suspicious for metastatic disease. He underwent trans-urethral resection of the urinary bladder tumour (TURBT). The pathology examination demonstrated revealed non-caseating granulomas (see figures 5 and 6).
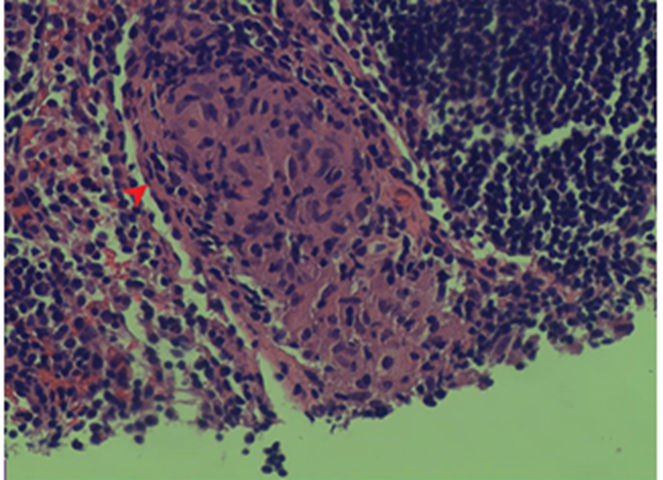
Figure 5:
Pathology of the bladder mass showing noncaseating granulomas (arrow). Reproduced from: [37] under the Creative Commons Attribution License.
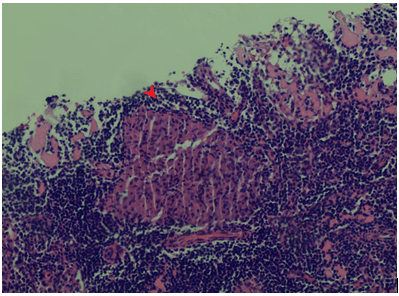
Figure 6:
Pathology of the bladder mass showing noncaseating granulomas (arrow). Reproduced from: [37] under the Creative Commons Attribution License.
On hospital day 7, he developed new-onset left-sided weakness including reduced grip strength and left-sided facial droop. He had brain radiology-imaging which showed persistent vasogenic oedema. After a discussion with all the specialists, the decision was taken to commence steroids preceding his CSF analysis. Acid-fast bacilli (AFB) stains from the axillary lymph node as well as the urinary bladder tumour upon examination were reported to be negative. At that time, a lumbar puncture was undertaken which was negative for infection or malignancy. His CSF angiotensin-converting enzyme (ACE) levels were noted to be within normal limits (see Tables 1 and 2).
| Laboratory test | Result | Reference values |
| Treponemal-specific enzyme immunoassay | <0> | 0.0-0.9 |
| Neisseria gonorrhoeae DNA amplification | Negative | Negative |
| Chlamydia trachomatis DNA amplification | Negative | Negative |
| EBV DNA (PCR) | Negative | Negative |
| CMV DNA qual (PCR) | Negative | Negative |
| Hepatitis Bs Ag | Positive | Negative |
| Hepatitis Bs Ab | 0 mIU/mL | >12.0 mIU/mL |
| Hepatitis Bc IgM Ab | Negative | Negative |
| Hepatitis Be Ag | Positive | Negative |
| HIV 1 and 2 Ag/Ab | Nonreactive | Nonreactive |
Table 1: Infectious workup.
PCR: polymerase chain reaction; Ab: antibody; Ag: antigen; EBV: Ebstein-Barr virus; CMV: cytomegalovirus; HIV: human immunodeficiency virus. Reproduced from: [37] under the Creative Commons Attribution License.
| CSF analysis | Result | Reference values |
| Appearance | Clear | Clear |
| WBC | 3 | 0-10/CMM |
| RBC | 0 | 0-3/CMM |
| Neutrophils % | 0 | 0-6% |
| Lymphocytes % | 55 | 40-80% |
| Monocytes % | 45 | 15-45% |
| Glucose | 66 | 40-70 mg/dL |
| Total protein | 62.5 | 15-45 mg/dL |
| Angiotensin-converting enzyme | <1> | 0.0-3.1 U/L |
| IgG* | 7.7 | 0.0-10.3 |
| Serum analysis | ||
| IgG (serum) | 2535 | 603-1613 mg/dL |
| IgA (serum) | 104.1 | 70-400 mg/dL |
| IgM (serum) | <25> | 40-230 mg/dL |
| IgE (serum) | 159 | <100> |
| Free kappa light chain, quantitative | 208.7 | 3.3-19.4 mg/L |
| Free lambda light chain, quantitative | 11.2 | 5.7-26.3 mg/L |
| ANA screen | Negative | Negative |
Table 2: CSF and serum analysis
WBC: white blood cell; RBC: red blood cell; CSF: cerebrospinal fluid; ANA: antinuclear antibody. *IgG index was 0.4 (normal reference value 0.0-0.7). Reproduced from: [37] under the Creative Commons Attribution License.
He clinically improved after the commencement of steroids and he had a repeat MRI scan of the brain, which demonstrated moderate interval improvement with persistent leptomeningeal enhancement and resolution of the previously present mass effect on frontal horns. The diagnosis of neuro-sarcoidosis was favoured given bilateral hilar adenopathy on the CT scan of thorax, improvement in his radiology-imaging findings following steroid administration, and non-caseating granulomas that were found within the urinary bladder lesion. Neurosurgery and Oncology did not favour brain biopsy at that time. He was discharged home on dexamethasone with instructions to follow up with Rheumatology as an outpatient.
Hanif et al. [37] made the ensuing educative iterations:
| Diagnosis | Criteria |
| Probable | Non-neural pathology confirming systemic sarcoidosis. |
| Possible | The clinical picture is suggestive of neuro-sarcoidosis, but alternate diagnoses have not been ruled out and there is no systemic confirmation of sarcoidosis. |
| Definitive | Neural tissue showing noncaseating granulomas. |
Table 3: Diagnostic criteria
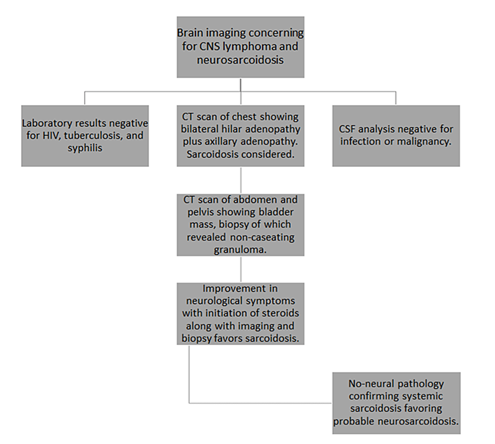
Figure 7: Diagnostic algorithm
CNS: central nervous system; CSF: cerebrospinal fluid. Reproduced from: [37] under the Creative Commons Attribution License.
Hanif et al. [37] made the ensuing conclusions:
Conflict Of Interest – Nil
Acknowledgements
Acknowledgements to:
Cureus for granting permission for figures and contents of their journal article to be reproduced under the Creative Commons Attribution License, under copyright: © Copyright 2023 Hanif et al. This is an open access article distributed under the terms of the Creative Commons Attribution License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
