
Research Article | DOI: https://doi.org/10.31579/2639-4162/248
Retired Urologist and Clinician, Reviewer of Articles for Journals, Medical Examiner Member of Royal College of Pathologists, London. United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, Retired Urologist and Clinician, Reviewer of Articles for Journals, Medical Examiner Member of Royal College of Pathologists, London. United Kingdom.
Citation: Anthony Kodzo-Grey Venyo (2025), Sarcoidosis of the Penis, J. General Medicine and Clinical Practice, 8(2); DOI:10.31579/2639-4162/248
Copyright: © 2025, Anthony Kodzo-Grey Venyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 December 2024 | Accepted: 20 January 2025 | Published: 30 January 2025
Keywords: sarcoidosis of penis; rare; biopsy; histopathology
Sarcoidosis is a systemic disease of unknown etiology whnich affects multiple organs of the body and which is characterized by the presence of non-caseating granulomas. It is very rare for patients who are afflicted by sarcoidosis of the penis to initially manifest with a lesion of the penis only. Sarcoidosis of the penis manifests with non-specific symptoms that simulate the manifestation more common afflictions of the penis and hence without the clinician having a high-index of suspicion for sarcoidosis of the penis, the diagnosis could be either missed easily or there would be a delay in the diagnosis of sarcoidosis of the penis. Diagnosis of sarcoidosis of the penis is made based upon pathology examination of biopsy specimens or excised specimens of the penile lesion.
Sarcoidosis is a terminology which is used for a systemic disease of unknown aetiology which affects multiple organs and is characterized by the presence of non-caseating granulomas. [1] Even though the aetiology of sarcoidosis is not known, the evidence has been iterated to point to an exaggerated immune response to an unidentified antigen as the most likely cause. [2] Confirmatory evidence of the presence of non-caseating granuloma within the specimen of the penile lesion is required in order to establish the diagnosis of sarcoidosis. In addition, other causes of granulomatous disease need to be excluded before the diagnosis of sarcoidosis of the penis is established or confirmed.[3] Sarcoidosis is known to mainly affect the lungs, lymphoid system, liver, and skin. [3] While sarcoidosis of the male reproductive system, including: the testis, epididymis, and prostate, had been reported sporadically in the literature, sarcoidosis of the penis is rare, and only a few case reports had been reported in the literature. [4] [5] [6] [7] [8] [9] [10] [11]
Aim
To provide an update on sarcoidosis.
[A] Overview
Definition, General statements, Practice Essentials. [12]
Signs and symptoms
The presenting signs and symptoms in sarcoidosis are stated to vary depending upon the extent and severity of the organ which is involved by sarcoidosis as follows: [13]
The pulmonary findings on physical examination of patients affected by sarcoidosis had been summarized as follows: [12]
It has been stated that dermatology manifestations of sarcoidosis may include the following: [12]
It has been iterated that ocular involvement, in cases of sarcoidosis which may lead to blindness if untreated, may present as follows: [12]
Other possible presentations of sarcoidosis do include the ensuing: [12]
Diagnosis
The radiology-image studies for sarcoidosis had been summarized as follows: [12]
Staging of sarcoidosis had been summated as follows: [12]
It has been stated that pulmonary function tests and a carbon monoxide diffusion capacity test of the lungs for carbon monoxide (DLCO) are used routinely in evaluation and follow-up of individuals afflicted by sarcoidosis. [12] and that some of the possible findings of the tests do include the following: [12]
Routine laboratory evaluation is stated to be often unrevealing, but possible abnormalities include the following: [12]
Management
The management of sarcoidosis has been summarized as follows: [12]
It has been iterated that non-steroidal anti-inflammatory drugs (NSAIDs) are indicated for the treatment of arthralgias and other rheumatic complaints. [12] It has also been stated that patients with stage I sarcoidosis often do require only occasional treatment with NSAIDs. [12]
Treatment in sarcoidosis patients with pulmonary involvement has been summated as follows:
For extrapulmonary sarcoidosis involving such critical organs such as the heart, liver, eyes, kidneys, or central nervous system, corticosteroid therapy is stated to be indicated. [12] It has been iterated that topical corticosteroids are effective for ocular disease. [12] For pulmonary sarcoidosis disease, it has been iterated that prednisone is generally given daily and then tapered over a 6-month course. It has also been stated that high-dose inhaled corticosteroids could be an option, particularly in sarcoidosis patients with endobronchial disease.
Common indications for non-corticosteroid agents in cases of sarcoidosis had been stated to include the ensuing: [12]
Non-corticosteroid agents that tend to be used in sarcoidosis include the ensuing: [12]
It had also been iterated that for sarcoidosis patients with advanced pulmonary fibrosis from sarcoidosis, lung transplantation remains the only hope for long-term survival and that indications for transplantation include either or both of the following. [29]:
[B] Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Studies Related to Sarcoidosis of The Penis.
Al-Riyami et al. [11] reported a 63-year-old African man, who presented to the University Health Centre of Sultan Qaboos University, Muscat, Oman with a six-month history of painless swelling of his penis. He denied having any history of genital trauma, urethral discharge, or any other urinary tract symptom. He did not have any other skin lesions. He was married and he did not have any extra-marital relationships. His clinical examination showed a 1 cm × 2 cm firm and non-tender nodule within the ventral part of his penis. He was referred to the urology clinic where he had an excisional biopsy of the swelling. Histopathology examination of the lesion revealed epithelioid histiocytes palisading around a nuclear dermis with mucin deposition, which was indicative of granuloma annulare (see figure 1)

Figure 1
Histological section of the penile lesion showing granuloma annulare. Localized necrotic collagen surrounded by lymphocytes. Magnification = 10 ×. Reproduced from: [11] under the Creative Commons Attribution License.
One year subsequently, he re-presented with similar painless skin nodules, but over his right upper limb. These skin nodules had subsequently spread to involve his thorax and trunk. He did not have any respiratory symptoms, fever, or joint pain. His family history was unremarkable, particularly for any similar manifestations or malignancies. Upon examination, he was noted to be well-built, and he looked comfortable. He did not have any palpable
cervical or axillary lymph nodes. He was found to have multiple 1 cm × 2 cm, firm and non-tender subcutaneous nodules over his right arm, chest, and trunk. His chest was clear, and his cardiovascular examination was normal. The results of his laboratory tests, which included complete blood count, fasting blood glucose, and liver function tests, were all normal. His renal function tests demonstrated features indicative of an acute kidney injury with high creatinine level and low glomerular filtration rate (GFR). The levels of his potassium and bicarbonate were within the normal range. A summary of the results of his laboratory tests is illustrated in table 1.
| Tests | Results | Normal range |
|---|---|---|
| Hemoglobin | 13.1 | 12.1–16.3 g/dL |
| WBC | 8 | 4.0–11.1 × 109/L |
| Platelet count | 316 | 150–400 × 109/L |
| BUN | 8.8 | 2.8–8.1 mmol/L |
| Creatinine | 205 | 59–104 umol/L |
| GFR | 28 | 1.73 mL/min/m2 |
| K | 4.8 | 3.5–5.1 mmol/L |
| Bicarbonate | 25 | 22–29 mmol/L |
| ESR | 37 | 0–22 mm/hr |
| ALT | 23 | 0–41 U/L |
| AST | 87 | 0–40 U/L |
| Calcium | 3.35 | 2.15–2.55 mmol/L |
| PTH | 0.4 | 1.6–9.3 pmol/L |
| Albumin | 45 | 35–52 g/L |
| CRP | <1> | 0–5 mg/L |
| ACE | 243 | 12–68 ACEU |
Table 1: Summary of laboratory test results in a 68-year-old male with a history of penile swelling.
WBC: white blood count; BUN: blood urea nitrogen; GFR: glomerular filtration rate; K: potassium; ESR: erythrocyte sedimentation rate; ALT: alanine aminotransferase; AST: aspartate aminotransferase; PTH: parathyroid hormone; CRP: C-reactive protein; ACE: angiotensin-converting enzyme. Reproduced from: [11] under the Creative Commons Attribution License. His chest radiography demonstrated a superior mediastinal mass with a bilateral hilar enlargement (see figure 2). He had computed tomography of his thorax, which demonstrated multiple enlarged mediastinal and hilar lymph nodes with no parenchymal infiltrations (see figure 3). He underwent a repeated excisional biopsy of one of the nodules upon his right arm which upon histopathology examination was noted to show non-caseating discrete granulomata with minimal lymphocytic cuff without vasculitis or panniculitis (see figure 4). Based upon the clinical features of the lesions and the results of the investigations, a diagnosis of sarcoidosis was made
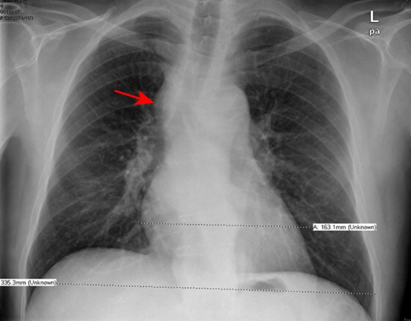
Figure 2: Chest X-ray showing superior mediastinal mass (red arrow). Reproduced from: [11] under the Creative Commons Attribution License.
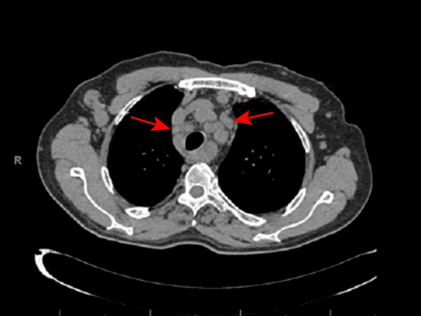
Figure 3: Axial computed tomography scan showing lymphadenopathy at the mediastinal area (red arrows) with clear lung parenchyma. Reproduced from: [11] under the Creative Commons Attribution License.
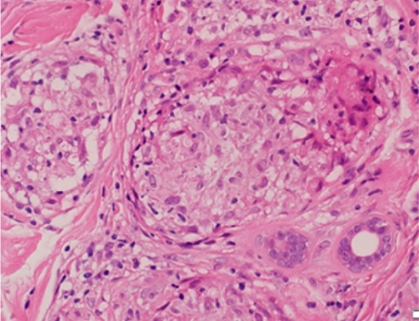
Figure 4
Histological section of right arm nodule showing a collection of epithelioid histiocytes surrounded by a thin cuff of lymphocytes, which composes non-caseating discrete granulomata. Magnification = 20 ×. Reproduced from: [11] under the Creative Commons Attribution License. Given the patient’s acute kidney injury and hypercalcemia, he was admitted to the hospital for hydration and treatment with calcitonin, following which he improved, and
his renal function test results became better. He was commenced on prednisolone 35 mg/day (0.4 mg/kg) and this was tapered down later once his clinical and biochemical parameters had improved. During his follow-up assessment after four weeks, he was asymptomatic. His serum calcium level and renal function tests had normalized. He had a repeat chest radiograph, which was undertaken three months subsequently, which demonstrated regression in the size of the mediastinal and hilar lymphadenopathy (see figure 5). The dose of his steroids was reduced gradually until a maintenance dose of 10 mg daily was reached. He had been seen regularly at the outpatient clinic and had remained in good condition since his discharge from hospital.
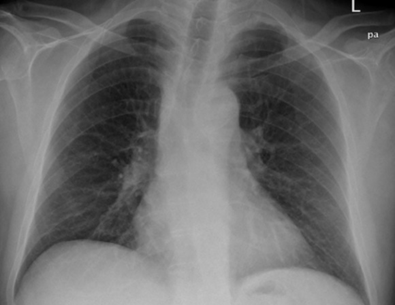
Figure 5: Chest X-ray showing regression of the superior mediastinal mass after treatment with steroid. Reproduced from: [11] under the Creative Commons Attribution License.
Al-Riyami et al. [11] made the ensuing educative discussions and iterations:
Al-Riyami et al. [11] made the ensuing conclusions:
Herodotou et al. [36] reported the case of a man, who manifested with several months’ history of distal penile swelling and progressive inability to retract the foreskin. Firm, non-tender subcutaneous nodules were palpated near the base of his penis during his examination. He ultimately underwent penile skin resection, partial scrotal resection, and split thickness skin graft to the penis after failure of multiple conservative treatments. Pathology examination of the specimen showed non-caseating granulomatous lesions which in addition to his computed tomography (CT) scan of thorax findings of bilateral hilar adenopathy suggested a diagnosis of sarcoidosis of the penis.
Semiz and Kobak. [36] stated the following:
Semiz and Kobak. [36] reported a patient with penile mass who was diagnosed with sarcoidosis on the basis of the laboratory, radiological, and pathological investigations. Semiz and Kobak. [36] made the ensuing conclusions:
Rubinstein et al. [37] reported a case of sarcoidosis which was identified histologically as the cause of chronic painful erythematous induration of the penis with several subcutaneous nodules and cutaneous ulceration in a 37-year-old African-American man, who presented with a 3-month history of an extensive, pruritic, eczematous eruption upon his scrotum with associated oedema and tenderness. Clusters of dark papules and plaques had developed upon his face over the preceding one month. He also reported having recent fevers, intermittent nausea and vomiting, difficulty in voiding, and occasional wheezing but he did not have any shortness of breath. Pathology examination of biopsy specimens of his lesions demonstrated features indicative of sarcoidosis. The lesions improved in response to topically applied corticosteroids but they reappeared later and persisted despite treatment. Rubinstein et al. [37] suggested that sarcoidosis, even though rare, should be considered in the differential diagnosis of any chronic lesion involving the penis in adults.
Algoet et al. [38] stated that sarcoidosis is a systemic disease of unknown origin affecting patients who are aged between 25 years and 40 years, and it has a higher incidence in women and in patients of African descent. Algoet et al. [39] reported the first case of sarcoidosis of the glans penis and penis, without systemic manifestations, in a patient of North African descent. Local treatment was commenced for the treatment of the sarcoidosis. Algoet et al. [38] advised that regular monitoring should be undertaken to assess for the possibility of systematization.
Wei et al. [39] reported a 31-year-old African-American man, who presented with cutaneous lesions upon his penis and scrotum over the preceding 2 years. The genital lesions were so prominent as to interfere with his coital life. Sarcoidosis was demonstrated upon pathology examination of biopsy specimens of his lesions on the penis and scrotum. Wei et al. [39] made the ensuing conclusions:
Conflict of Interest – none
Acknowledgements
Acknowledgements to:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
