
Case Report | DOI: https://doi.org/10.31579/2641-0419/009
1 Department of Cardiology, City of Health and Science of Turin, Turin, Italy
2 Villa Maria Hospital, Turin, Italy.
*Corresponding Author: Gianluca Alunni
Citation: Gianluca Alunni , Salvatore D'amico , Dario Celentani, Carlo Alberto Biolè , Alessandro Andreis , Marra Sebastiano. (2018) Safety of Extracorporeal shockwave myocardial revascularization (ESMR) in patient with a mechanical prosthetic valve: a case report. JClinical Cardiology and Cardiovascular Interventions, 1(2); Doi:10.31579/2641-0419/009
Copyright: © 2018. Gianluca Alunni. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 July 2018 | Accepted: 03 August 2018 | Published: 08 August 2018
Keywords: refractory angina; shock wave therapy; myocardial hypoperfusion
The number of patients with refractory angina without revascularization options is increasing. The prognosis and the quality of life in these patients is poor and maximal medical therapy is not enough for symptoms relieve.
64-years-old male patient with coronary artery disease debuted in 2002 with an anterior ST-elevation myocardial infarction (STEMI) treated by percutaneous coronary intervention (PCI) on medial left anterior descending artery (LAD) with implantation of a Bare Metal Stent (BMS).
In 2004, for the evidence of the stenosis of the bicuspid aortic valve and an ascending aorta aneurysm, substitution of the aortic valve and the ascending aorta with a mechanical valve attached to a Dacron tube graft (St. Jude 25mm + 28 mm) was performed.
In 2011, for new evidence of stress angina, PCI with a drug eluting stent (DES) implantation of the proximal RCA was performed.
In 2013, for stress angina recurrence, a myocardial single-photon emission computed tomography (SPECT) with pharmacological stress (Dipyridamole) was performed, with the evidence of modest inducible ischemia in inferior cardiac wall (SRS 3, SSS 9, SDS 6), without CAD progression at the coronary angiography.
For this reason, in 2014, we decided to treat the patient with shockwaves therapy.
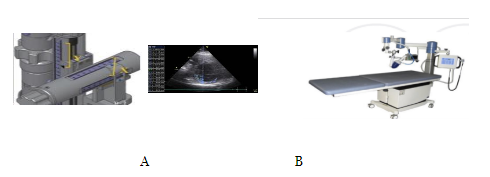
We locate the area to treat by documenting inducible ischemia at the stress myocardial SPECT. The ESMR were applicated with a commercially available cardiac shock wave generator system (Cardiospect TM, Medispec, Germantown, MD) under echocardiographic guidance (Figure 1.A and B): through a cardiac ultrasound imaging system, we look at this area and these measurements are calibrated into the shockwave applicator head to ensure the position of the focal treatment zone, so using an electrocardiographic R-wave gating, shockwaves are delivered through the applicator to the sub-endocardial myocardium of the ischemic area. We applied a low energy of shockwaves (0.09 mJ/mm2, ≈10% of the energy for the lithotripsy treatment).
The ischemic area was divided into 3 zones, corresponding to the three sessions of treatments. The treatment was divided into three sessions with 3 treatments for week every 4 weeks. 100 pulses gated by R wave trigger was performed for each target spotted (up to a total of 1000 pulses) at each individual session. Each session lasted about 20 minutes. During the treatment, symptoms and vital signs were continuously monitored.
A regular echocardiographic follow-up was performed, without evidence of malfunction or complications about the mechanical prosthetic aortic valve and tube:
In 2013, before ESMR therapy, prosthetic valve had a normal function and position, pressure gradient (PG) was 13/6 mmHg, Aortic Valve Area (AVA) measured by Velocity Time integral (VTi) was 2.3 cm2 and Doppler Velocity index (DVi) was 0.56. Prosthetic tub was regular without dehiscence.
-In 2014 prosthetic valve had a normal function and position, PG was 15/8 mmHg, V max was 2 m/sec and DVi was 0.30. Prosthetic tub was regular without dehiscence (Figure 2).

Last echocardiographic study was performed in January 2018 and showed a prosthetic valve with a normal function and position, PG was 12/8 mmHg, V max was 1.7 m/sec. Prosthetic tub was regular without dehiscence (Figure 3).

The number of patients with refractory angina without revascularization options is increasing. The prognosis and the quality of life in these patients is poor and maximal medical therapy is not enough for symptoms relieve.
According to the last American College of Cardiology/American Heart Association (ACC/AHA) guidelines on the management of chronic stable angina, the objective of the treatment should be the resolution of angina attacks, the reduction of the numbers of hospitalizations and the carrying out of normal daily activities without symptoms [1-6].
Extracorporeal Shockwave Myocardial Revascularization therapy (ESMR) is a non-invasive treatment and several studies have demonstrated its safety and its efficacy in patients with refractory angina (RA) to improve myocardial perfusion and exercise capacity reducing symptoms by the application shockwaves (SW) on the culprit ischemic area of the heart under echocardiographic guidance [7-26]. Shockwaves consist of low-intensive acoustic energy artificially generated by discharging of a high voltage spark under water by a generator designed to address the clinical anatomical requirements of the chest cavity. Several treatment sessions are required. The aim of this treatment is former to induce vasodilatation and latter to induce neovascularization from the healthy area to the ischemic area [27-37].
But, actually, there are no data about the safety of ESMR in patients with a mechanical prosthetic valve.
We would report about a 64-year-old man with coronary artery disease (CAD) and refractory angina pectoris despite maximally tolerated medical therapy and after percutaneous coronary intervention (PCI) and with a prosthetic aortic valve and aortic tube.
The patient received extracorporeal shockwave myocardial revascularization therapy without any complication during or after treatment.
We locate the area to treat by documenting inducible ischemia at the stress myocardial SPECT. The ESMR were applicated with a commercially available cardiac shock wave generator system (Cardiospect TM, Medispec, Germantown, MD) under echocardiographic guidance (Figure 1.A and B): through a cardiac ultrasound imaging system, we look at this area and these measurements are calibrated into the shockwave applicator head to ensure the position of the focal treatment zone, so using an electrocardiographic R-wave gating, shockwaves are delivered through the applicator to the sub-endocardial myocardium of the ischemic area. We applied a low energy of shockwaves (0.09 mJ/mm2, ≈10% of the energy for the lithotripsy treatment).
In conclusion, we treated by ESMR a patient with refractory angina and with mechanical prosthetic aortic valve and tube, without any sign of complication or malfunction of the cardiac device in acute or in further years.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
