
Review Article | DOI: https://doi.org/10.31579/2642-973X/123
1University of South Wales, UK.
2California Institute of Neuroscience, USA.
*Corresponding Author: Abba M Abdullahi. University of South Wales, UK.
Citation: Abba M Abdullahi, Shah T Sarmast, (2024), Safety and Efficacy of Mannitol in Treatment of Cerebral Malaria: A Systematic Review of Randomized Control Trials, J. Brain and Neurological Disorders, 7(4): DOI:10.31579/2642-973X/123
Copyright: © 2024, Abba M Abdullahi. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 October 2024 | Accepted: 21 October 2024 | Published: 31 October 2024
Keywords: ovale, vivax; malaria and knowlesi; anti-malarial
Cerebral malaria is one of the leading causes of death and disability in Sub-Saharan Africa. It is characterized by convulsion, sustained coma due to brain swelling, debilitating neurological complications, behavioral and cognitive disturbances. It is associated with a high morbidity and mortality especially in children, posing high demand for highly effective, curative, and long-lasting therapies. Cerebral malaria is a medical emergency that requires urgent treatment to prevent related mortality and disabilities. It is primarily treated with artesunate as par current WHO recommendation; however, other form of parenteral anti-malarials like quinine can be used. Additionally, many adjunctive therapies were used, especially in countries where the disease is endemic. One of these therapies is the mannitol, which is an osmotically active drug that can lower intracranial pressure by absorbing extracellular fluid into the vascular compartment. Therefore, to determine the safety and efficacy of mannitol in the treatment of cerebral malaria, we systematically searched published data from main databases including PubMed, PubMed Central, Google Scholar, ScienceDirect, and Medline. Two research registries were also searched: the Cochrane Registry and clinicaltrial.gov. Data was collected after applying inclusion and exclusion criteria and studies were appraised critically. Both Medical Subject Headings (MeSH) and regular keyword search strategies were employed. The review findings indicated that mannitol therapy is safe and relative effective when used early in children less than five years, but comparably harmful when used in older adults especially when co-associated with other factors like hypertension, hypocholesterolemia, smoking and excessive alcohol consumption.
Malaria is a vector-borne parasitic disease caused by plasmodium species and transmitted by the bite of female anopheles’ mosquito. There are currently five recognized plasmodium species that can cause malaria: plasmodium falciparum, ovale, vivax, malaria and knowlesi (Ashley, Pyae Phyo, & Woodrow, 2018). Malaria is more common and endemic in tropical and subtropical countries with devastating consequences on health and economy. An estimated 212 million malaria cases occurred globally in the year 2015 with over 90% of the cases occurring in African countries, 7% of the cases in South East Asia and less than 2% of the cases occurred in Eastern Mediterranean Region. As of 2015, the malaria related mortality was estimated to be 429,000 cases globally, 92% of which occurred in African region and virtually all the deaths (99%) were plasmodium falciparum related (WHO, 2016). Based on clinical features, malaria is classified into two main types: uncomplicated and complicated
or severe malaria. The former present with non-specific signs and symptoms including fever, myalgia, headache, and diarrhea or vomiting. Whereas the later presents with serious clinical syndromes including hyperpyrexia, convulsion, confusion, abnormal breathing, jaundice, anuria or features of cerebral impairment (Ashley et al., 2018).
Cerebral malaria is the most serious and fatal form of severe malaria which has high morbidity and mortality, almost 100
2.1. Study Design and Protocol
A systematic review of published literatures on mannitol use in the treatment of cerebral malaria. The protocol used for this study was based on the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)’.
2.2. Data Collection
Major electronic databases were searched for relevant information which include PubMed, PubMed Central, Medline, ScienceDirect and Google Scholar. Two research registry comprising of Cochrane central register (Cochrane library 2020 issue 4) and clinicaltrial.gov (www.clinicaltrials.gov) were searched for relevant clinical trials. A search of the reference lists of the included articles for related articles was conducted and effort was made to search unpublished literatures by contacting experts. The following key words were used as search content for identification of relevant data: “mannitol” AND “cerebral malaria” AND “randomized trials”, “cerebral malaria” AND “adjunctive therapy” AND “randomized trials”, “randomized trials” AND “cerebral malaria” AND “treatment”.
2.3. Inclusion and Exclusion Criteria
The following inclusion criteria were used: 1) any randomized trials on mannitol treatment in cerebral malaria 2) studies done exclusively on cerebral malaria 3) studies done exclusively on humans 4) studies done in English or translated into English. Any study that combine mannitol and any other adjunctive therapy were excluded.
2.4. Population
We included patients with cerebral malaria as defined by WHO regardless of their age, sex or country of origin.
2.5. Intervention
The intervention we included is the use of mannitol as adjunctive therapy for cerebral malaria in addition to the standard antimalaria therapy.
2.6. Comparison
Patients with cerebral malaria who received mannitol as adjunctive therapy were compared with control groups who received only standard antimalarial treatment with or without placebo.
2.7. Outcome
We aimed to assess the following primary outcomes: mortality, systemic complications and neurologic sequelae. The secondary outcomes of interest include regain of consciousness, duration of hospitalization, ability to take orally, and cardiopulmonary compromise.
2.8. Data Extraction
A standard data extraction form was used for data extraction from the included studies in which the following information were extracted from both the intervention and control group: authors’ details, publication year, sample size, demography of the study population, dose of the mannitol, type of the antimalarial used and dose, route of administration, outcomes data and follow up period.
2.9. Risk of Bias Assessment
The risk of bias was determined based on the following domains: random sequence generation, allocation concealment, patient blind and care provider blind, intention to treat analysis, outcome assessor blind, incomplete outcome data and selective outcome reporting (Estellat C, Torgerson DJ, 2009). Each domain is graded as high, moderate or low with information from the study paper justifying our judgment.
2.10. Quality Assessment
CASP Checklist (2018) for Randomized Controlled Trials was used for assessing the validity of the included randomized control trial studies(CASP Checklist RCT, 2018) which contain 11 questions that assess the validity and effectiveness of the study results. A score of >7 was considered as a high-quality paper, 5-7 a moderate quality and <5>
3.1. Literature Search
A search of multiple electronic databases yielded 513 articles. 16 articles from PubMed, 144 from PubMed Central, 122 from Medline, 155 from Google Scholar, 71 from ScienceDirect, 3 from Cochrane database registry and 2 from clinicaltrial.gov registry. Nine articles were selected for possible inclusion after review of abstracts and the remaining 504 articles were found to be irrelevant to the study and therefore discarded. After full text review of the 9 articles, only 2 articles were found to have met the inclusion/exclusion criteria and thus included in the meta-analysis with the remained 7 articles been removed. The 2 articles were subjected to critical appraisal and were found to be assessed as high-quality papers. Therefore, only two articles were included in the meta-analysis (figure 1).
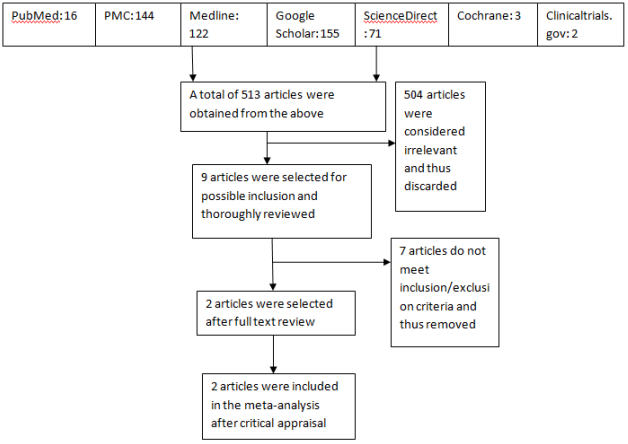
Figure 1: Flowchart of the study selection
3.2. Study Characteristics
Only two studies were identified to have met the criteria for inclusion in this review. The first paper (Namutangula, Ndeezi, Byarugaba, & Tumwine, 2007) was a randomized double blind placebo clinical trial on children between 6 month to five years, while the second paper (Mohanty et al., 2011) is a randomized open label non-placebo clinical trial on individuals who are 16 yrs old or older. Both studies were done on patients with cerebral malaria as par WHO definition of cerebral malaria. In the first study, the total sample size was 156 subjects: 80 subjects in the controlled group and 76 in the intervention group. The total male and female subjects were 80 and 76 subjects respectively. The minimum age of the participants in the first study was 6 months and the maximum age was 5yr. The total sample size of the second study was 61 subjects: 31 subjects in the controlled group and 30 in the intervention group. There are 30 male subjects and 31 female subjects entirely. The minimum age of the participants in the second study was 16 yr and the maximum age was 36yr.
3.3. Dosing
In both studies, all patients received quinine as the malaria treatment which was given intravenously at the dose of 10mg salt/kg body weight in 10mls/kg of 5
Both papers have low risk of bias as the methods of randomization were clearly mentioned. The adequate allocation concealment in the study eliminated selection bias which indicates good quality. In this review, it is apparent that there were clear differences in the themes and variables reported across the two studies. In the first study, which involved patients aged between 6 months to five years, the use of mannitol in the treatment of cerebral malaria was relatively safe and effective. This finding was also reported in study by Sekarningrum and colleagues, where early mannitol administration was shown to have improved outcomes in pediatric patient with cerebral edema, though cause of the edema was not categorically described in the study (Sekarningrum et al., 2018). However, in the second study, which involved adult patients aged ≥ 16yr, the use of mannitol in the treatment of cerebral malaria was generally unsafe and can be considered as harmful due to modest increase in mortality and prolong duration of coma among intervention group as compared to controlled group. Many reasons could be accounted for the effect dichotomy between the two studies.
Firstly, the age differences between the subjects in the two studies could be an important factor in determining the safety and efficacy of mannitol therapy in cerebral malaria. In many preclinical studies, increasing age has been identified to be associated with increased size of cerebral infarction that may subsequently result in cerebral edema (Idro, Jenkins, & Newton, 2005). This could explain the observed effects in the second study that showed a trend of increased mortality and longer duration of coma in the intervention group than control group. Additionally, the coma of cerebral malaria is more likely to develop from multiple etiologies in adults than in children (Newton & Warrell, 1998). For example, cerebral edema and raised intracranial pressure may occur concomitantly which may result into coma. In this case, for example, the mannitol would handle the cerebral edema but might not have effect on the raised intracranial pressure and therefore leading to prolong coma duration. Also, the double blinding in the first study eliminated outcomes bias, whose absence in the second paper increased risk of the bias which could be attributed to the effects observed in the second study.
Secondly, intracerebral hemorrhages and lacunar infarctions have been described in the pathophysiology of cerebral malaria which could lead to microvascular obstruction. Thus, introduction of hyperosmolar solution like mannitol could further exacerbate the fluid exchange in the already compromised microcirculation (Newton & Warrell, 1998). The risk factors for these pathologic findings include old age, hypertension, smoking, excessive alcohol consumption, hypocholesterolemia and drugs (Pongponratn et al., 2003). These factors are more common in adults than in children further explaining the differences in the safety and efficacy of the mannitol across the two studies. Thirdly, the dose used in the second study (1.5g/kg start followed by 0.5g/kg 8hrly) is actually low to observe the beneficial effects of mannitol in adults, which can be compared with the dose used in the first study (1g/kg 8hrly). The doses of mannitol used in many studies ranges between 0.25g/kg to 2.5 g/kg, and studies that uses higher doses showed relative higher efficacy of using mannitol as adjunctive therapy in the treatment of cerebral malaria. However, higher doses of mannitol could significantly affect renal function and therefore, care has to be taken when prescribing high dose by monitoring renal function (Mohanty, Patel, Pati, & Mishra, 2006).
The safety and efficacy of mannitol as adjunctive therapy in the treatment of cerebral malaria has shown different therapeutic profile in this review. Based on the findings, it can be hypothesized that use of mannitol in patients with cerebral malaria is relatively safe and effective when used in children less than five years due to the trend of improvement observed in the first study among the intervention group more than the controlled group. However, it is comparatively harmful and ineffective when used in older patients due to the increased mortality rate and longer duration of coma recovery period observed in the second study among the intervention group more than in the controlled group. Therefore, we hypothesized that early use of mannitol as adjunctive therapy in the treatment of cerebral malaria in children less than five years is relative safe and can improve patient outcome, reduce duration of coma, decrease rate of neurologic complications and facilitate early discharge from the hospital. We also hypothesized that mannitol should not routinely be used in older patients and when necessary, certain risk factors should be rule out first including advancing age, hypertension, hypocholesterolemia, drug abuse, smoking and excessive alcohol consumption. However, more randomized clinitical trial studies are needed to ascertain the safety and efficacy of the drug in cerebral malaria treatment in any age group.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
