
Case Report | DOI: https://doi.org/10.31579/cotc/2020/011
1Departement of Orthopeadics, Sahloul Hospital, Faculty of Medecine of Sousse, Tunisia.
2Departement of Internal Medicine, Mohamed Taher Maamouri Hospital, 8000 Nabeul, Tunisia.
*Corresponding Author: Dr. Zeineb Alaya, Departement of Internal Medicine, Mohamed Taher Maamouri Hospital, 8000 Nabeul, Tunisia.
Citation: L. Hassini, MA. Khalifa, Z. Alaya, A. Siala, W. Osman, K, et al. (2020) Sacral osteoid osteoma: a rare cause of back pain in childhood. Clinical Orthopaedics and Trauma Care. 2(2); DOI:10.31579/cotc/2020/011
Copyright: ©2020 Zeineb Alaya, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 October 2020 | Accepted: 13 November 2020 | Published: 17 November 2020
Keywords: osteoid; osteoma; sacrum; bone
Involvement of the sacrum is extremely rare, and it has also been reported that the diagnosis of osteoid osteoma in the sacrum can be delayed compared to other skeletal locations. We report the case of a six-year-old girl student who complained of chronic back pain for several months and with some relief with non-steroid anti-inflammatory drugs (NSAID). Further investigations, which included bone and CT scan, revealed the presence of an osteoid osteoma at the second sacral vertebra (S2 vertebra). The patient made an excellent recovery after surgical excision.
The spine is a rare localization of osteoid osteoma and the sacrum is even more exceptional. Only 2% of spinal osteoid osteomas are found in the sacrum [2]. The majority of osteoid osteomas occur below the age of 20 [7]. We report a rare case of a six-year-old girl student who complained of chronic back pain for several months, and who felt some relief with non-steroid anti-inflammatory drugs (NSAID). Further investigations, which included bone and CT scan, uncovered the presence of an osteoid osteoma at the second sacral vertebra (S2 vertebra). The patient obtained favorable results after surgical excision.
Observation:
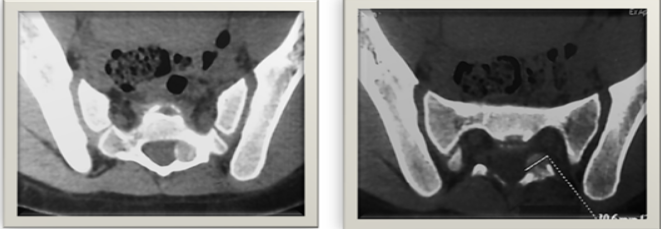
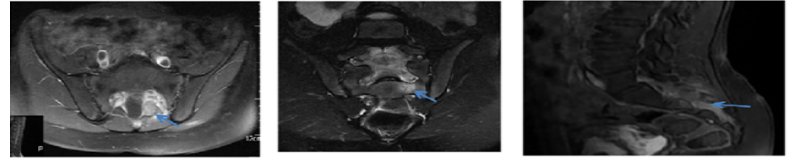
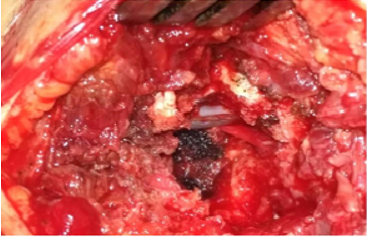
A six-year-old girl Student presented to our outpatient clinic with a chronic back pain evolving for several months and alleviated with non-steroid anti-inflammatory drugs (NSAID). On physical examination, there was pain at palpation of the sacrum but no signs of neurological deficits. Biology tests and plain radiographs of the pelvis were normal (figure 1). A sacral computerized tomography (CT) was performed to confirm the diagnosis, depicting a well- demarcated hyper dense sclerotic nodular lesion of about 10.6 mm in size, with its hypodense peripheral rim on the left lamina of S2 vertebra(Figures 2 and 3). A 0.3 cm nidus was also detected at the center of the reactive bone sclerosis on the CT scan. The lesion was compressing the left S2 root. A magnetic resonance imaging study was performed revealing subtle signal intensity changes in the sacral region in T1 and T2 images (Figures 4 and 5). The lesion was enhanced after gadolinium administration (Figure 6). The patient underwent surgery and the lesion was completely excised (Figure 7). The histopathological exam reported it as osteoid osteoma (Figure 8). At three-year follow-up, the patient was asymptomatic with no signs of recurrence.


Osteoid osteoma is a benign bone-forming neoplasm, first described by Jaffe in 1935 [1]. Approximately 10% of all benign bone tumors are osteoid osteomas [2, 3]. Any portion of the skeleton may be involved, but it is often found (50–60% of cases) in the long bones of the lower extremity [3] and (between 19 and 31% of the cases) upper extremity [4, 5], whereas about 20% occur in the spine [6]. 2% of spinal osteoid osteomas are found in the sacrum [2], and only 19 cases have been reported to date in the English-language literature [7]. Barei et al have noticed that the majority of osteoid osteomas occur in patients less than 20 years of age [8]. Its pathogenesis is controversial [9]. In fact, it is characterized by a highly innerved and hypervascularized central nidus, surrounded by a reactive peripheric osteogenesis. In the nidus, an important prostaglandin production is observed, causing the pain and explaining the regression under Acetyl-salicylic acid and other NSAID. Osteoid osteoma clinically manifests with a localized paroxystic night time pain. This pain regresses with acetyl-salicylic acid and other NSAID. In our case, the patient complained of chronic back pain of several months duration and with some relief with non-steroid anti inflammatory drugs (NSAID). In the sacrum, when S 1 is involved a marked spinal stiffness is usually present (60 %); in contrast, spinal stiffness is rare when the lesion spares S-1 (20 %). Neurological symptoms are rare (30 %), they are usually found in lesions more than 2 cm in diameter [10]. Scoliosis is usually present in lesions eccentrically involving either the body or the posterior elements of S-1. When the lesion is located centrally in S-1 or spares it, scoliosis is rare [11]. Plain radiographs rarely allow diagnosis and give poor information about the lesion. The central nidus is rarely seen. However, in case of scoliosis, the lesion could be found in the top of the curve and even on the adjacent ribs. CT is particularly useful for characterizing spinal osteoid osteomas. These lesions typically manifest as low-density nidus in the posterior elements. Many studies have cited the superiority of CT over MRI in both diagnosing and characterizing osteoid osteomas [12]. Technetium-99– labeled bone scintigraphy may prove useful for confirming the diagnosis with a 100% virtual sensitivity for detection [13]. The management depends on the location, size and the symptoms of the patient. There are various treatment options for this entity and radiofrequency ablation remains the treatment of choice in selected cases with the appropriate setting [14]. The lesion should not be near to the thecal sac and there should be enough cortical bone in the surrounding region. Air in the region can be of benefit being non-conductive of heat. If these conditions are not present, surgical excision becomes the most viable treatment option (reference). Likewise, in our patient the lesion was in close proximity to the left S2 root, which justified a surgical excision.
Conclusion:
Osteoid osteoma is a relatively frequent benign bone tumor of osteoblastic origin. Multicentric, intra- or juxta-articular, medullary and sub-periosteal lesions are called atypical osteoid osteoma. The diagnosis should be referred to as having a low back pain in an infant. CT scan and/or MRI allow to visualize the lesion and its extent to the neural elements. Surgical excision is an effective technique for the obtaining of good clinical results.
Conflict of Interest
The authors declare that they have no competing interests.
Authors’ contributions: All authors have read and agreed to the final version of this manuscript and have equally contributed to its content and to the management of the case.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
