
Research Article | DOI: https://doi.org/10.31579/2690-1919/411
1 Postgraduate Dental Student, Restorative and Esthetic Dentistry Department, Faculty of Dentistry, Sana’a University, Sana’a, Yemen.
2 Associate professor of Restorative Dentistry. Fixed Prosthodontics, Restorative and Esthetic Dentistry Department, Faculty of Dentistry, Thamar University, Yemen.
3 Assistant Professor of Endodontic, Restorative and Esthetic Dentistry Department, Faculty of Dentistry, Sana’a University, Yemen.
4 Professor of Restorative Dentistry, Dental Implant Consultant, Restorative and Esthetic Dentistry Department, Faculty of Dentistry, Sana’a University, Yemen.
*Corresponding Author: Abdulwahab Ismail Al-kholani, Professor of Restorative Dentistry, Dental Implant Consultant, Restorative and Esthetic Dentistry Department, Faculty of Dentistry, Sana’a University, Sana’a, Yemen.
Citation: Redha Mohammed Saleh Al-Nosra, Mohsen Ali Al-Hamzi, Basheer Hamed Al-Shameri, Abdulwahab Ismail Al-kholani, (2024), Root and Canal Morphology of Maxillary Incisors Teeth in a Sample of Yemeni Population Using Two Classification Systems: A CBCT Study, J Clinical Research and Reports, 16(5); DOI:10.31579/2690-1919/411
Copyright: © 2024, Abdulwahab Ismail Al-kholani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 September 2024 | Accepted: 27 September 2024 | Published: 07 October 2024
Keywords: maxillary incisors; root canal morphology; cbct, yemeni population; endodontics; vertucci's classification; ahmed's classification
Objective: To determine the root and canal morphology of permanent maxillary central and lateral incisors in a sample of Yemeni population using cone-beam computed tomography (CBCT).
Materials and Methods: A retrospective CBCT analysis of 400 maxillary anterior teeth from a Yemeni adults (18-50 years) was conducted. Image evaluation in sagittal, axial, and coronal planes using Ez3D-i software assessed root number, canal orifice number, canal number, and canal configuration based on Vertucci's and Ahmed's classifications. Descriptive statistics and Chi-square test were employed (p < 0.05).
Results: All incisors exhibited a single root and canal with a single orifice. The predominant canal configuration was Type 1 according to both Vertucci's (93.5%) and Ahmed's (93.8%) classifications. Type 5 (bifurcation at the apex) was observed in 6.25% (Vertucci) and 6.0% (Ahmed) of cases, while Type 3 (canal division and reunion) was rare (0.25% Vertucci, 0.2% Ahmed).
Conclusion: Permanent maxillary central and lateral incisors in the Yemeni population primarily demonstrate a single root and canal. Although variations in canal configuration exist, they are infrequent.
A comprehensive understanding of root canal morphology is crucial for successful endodontic treatment. While clinicians are generally familiar with typical canal configurations, variations are common and can significantly impact treatment outcomes. Inadequate knowledge of root canal anatomy is a major contributing factor to treatment failures. Accurate identification, cleaning, shaping, and obturation of all existing canals are essential for optimal results.
Previous studies have reported that maxillary anterior teeth typically have a single root and canal, while mandibular anterior teeth often exhibit double canals (da Silva et al., 2016; Rankine-Wilson and Henry, 1965). Additionally, variations in canal morphology can be influenced by ethnic background (Karobari et al., 2021). Successful endodontic therapy requires a thorough knowledge of tooth anatomy and root canal morphology, which can vary significantly. Anomalies or deviations from the usual shape and root number in the adult human dentition may also occur. When an anomalous form of the tooth or root anatomy is relatively common in a specific population or ethnic group, it should be considered a variant form and recognized (Ilan Rotstein and John I. Ingle, 2019; Torabinejad and Walton, 2009).
Imaging technology has become an essential diagnostic tool in dentistry. Conventional or digital panoramic, intraoral periapical, and bitewing radiographs are commonly used. While these techniques are user-friendly, quick to perform, and relatively inexpensive, they have limitations, such as geometric distortion, superimposition of anatomical structures, and dependence on observer interpretation (Martins et al., 2014).
The advent of three-dimensional imaging techniques, particularly cone-beam computed tomography (CBCT), has revolutionized the study of root canal morphology. CBCT provides detailed, non-invasive visualizations of root canal systems, surpassing the limitations of conventional radiography. It allows for accurate assessment of canal configurations, including complex intercanal communications, lateral canals, and apical ramifications.
Various classification systems have been proposed to categorize root canal morphology, with Vertucci's classification being widely recognized. However, this system has limitations, particularly its inability to account for the number of roots present. The new classification system proposed by Ahmed et al. addresses this limitation, providing a comprehensive code that encompasses tooth number, number of roots, and canal configuration, leading to improved communication and documentation among dentists.
This study aims to evaluate the root and canal morphology of permanent maxillary anterior teeth in a Yemeni population using CBCT, employing both Vertucci's classification and the new classification system by Ahmed et al. This investigation seeks to provide detailed insights into the prevalence of different canal configurations and their implications for endodontic treatment.
Study Design and Participants
This retrospective cross-sectional study analyzed cone-beam computed tomography (CBCT) images of maxillary anterior teeth from a Yemeni population. A total of 400 teeth (200 from males and 200 from females) were included, with participants aged 18-50 years. The images were obtained from the database of Al-Waleed Digital Radiology Center in Sana'a, Yemen.
Inclusion and Exclusion Criteria
Teeth were included if they met the following criteria: fully erupted, sound without any damage or disease, complete root formation, and bilateral symmetry. Teeth were excluded if they had caries, restorations, periapical lesions, periodontal problems, orthodontic history, generalized bone loss, implants, fixed prostheses, developmental anomalies, trauma, or poor image quality.
CBCT Acquisition
CBCT images were acquired using a Pax-Flex3D (PHT-60CFO) imaging system (VATECH Global, Korea) with the following settings: 60 kVp, 4 mA, 9-15 seconds exposure time, and a voxel size of 80-120 μm. A medium field of view (FOV) was selected to capture the maxillary anterior teeth.
Image Analysis
Image analysis was conducted using Ez3D-i software (VATECH Global, Korea) in a dimmed room with a calibrated diagnostic display. The researcher was blinded to patient information during the evaluation. Axial, coronal, and sagittal slices were examined for each tooth, with image contrast and brightness adjusted as needed.
The following parameters were evaluated:
Statistical Analysis
Data were analyzed using SPSS (Version 27.0; SPSS Inc., Chicago, IL, USA). Descriptive statistics (frequencies and percentages) were calculated for all parameters. The Chi-square test was used to compare canal configurations between males and females, with a significance level set at p < 0>
External Root Morphology of maxillary anterior teeth
An analysis of 400 maxillary anterior teeth revealed a consistent single-root morphology. This finding suggests that a single root is a characteristic feature of these teeth, regardless of their position or the patient's gender. This information is crucial for understanding the anatomy of maxillary anterior teeth and has implications for clinical procedures, such as root canal treatments and orthodontic interventions.
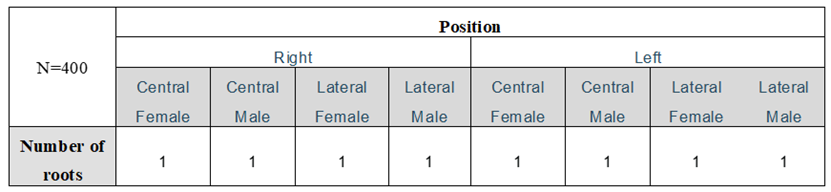
Table 1: Root Number in the Maxillary anterior teeth for both male and female, right and left.
The distribution of root counts in maxillary anterior teeth, based on the tooth's position (left or right), location (central or lateral), and participant gender (female or male), as shown in Table 1 The table reveals that, in this sample of 400 teeth, a single root (n=1) was found in every case across all conditions. This finding indicates that the maxillary anterior teeth in this study sample consistently exhibit a single root morphology.
Internal Root Morphology of Incisors:
1.Number of Canal Orifices: A single canal orifice was observed in 100% of the teeth.
A thorough examination of 400 incisors (200 central and 200 lateral, from both sides of the mouth) consistently found a single canal orifice as shown in figure 1. This pattern was consistent across all genders and tooth types. The high prevalence of single canal orifices (100%) see figure 1 in incisors simplifies endodontic treatment by reducing the complexity of canal identification and negotiation. Dental professionals can confidently approach these teeth with the knowledge that they are primarily dealing with a single root canal system
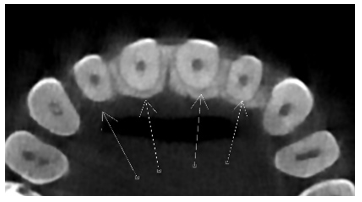
Figure 1: axial view number of Canal Orifices: A single canal orifice was observed in 100% of the anterior incisors teeth.
| N=400 | Position | ||||||||
| Left | Right | ||||||||
| Central Female | Central male | Lateral Female | Lateral male | Central Female | Central male | Lateral Female | Lateral male | ||
Number of canal orifices
| Count | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Percentage | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | |
Table 2: Count and Percentage of Canal Orifices in Central and Lateral Incisors for Male and Female Subjects (N=400)
Table 2 a comprehensive analysis of 400 incisors revealed that all teeth, regardless of gender, position, or tooth type, consistently had a single canal orifice. This high percentage of single-canal orifices has significant implications for endodontic treatment, as dentists can approach these teeth with a simplified treatment plan, reducing the complexity of canal identification and negotiation.
1.Number of Canals: All maxillary anterior teeth (100%) presented with a single canal.
| N=400 | Position | ||||||||
| Left | Right | ||||||||
| Central Female | Central male | Lateral Female | Lateral male | Central Female | Central male | Lateral Female | Lateral male | ||
| Number of canals | Count | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| % | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | |
Table 3: Number of Canals in Maxillary Anterior Teeth by Position and Gender.
The table 3 presents data on the number of canals in 400 individuals categorized by position (left, right, central, or lateral) and gender (male or female). Everyone has exactly one canal, regardless of their position or gender. The data shows no variation in canal count among the individuals in the sample, suggesting that these factors do not influence the number of canals. However, a larger sample size and consideration of additional variables would be necessary to draw more definitive conclusions.
Canal Count
All tooth types (central and lateral incisors) and positions (left and right) exhibited a uniform count of one canal per tooth, regardless of gender. This uniformity was confirmed by the percentages, showing that 100% of the teeth sampled in each category had a single canal.
Canal Configurations
Vertucci's Classification:
| N=400 | Position | Frequency | % | |||||||||||||||
| Left | Right | |||||||||||||||||
| Central Female | Central male | Lateral Female | Lateral male | Central Female | Central male | Lateral Female | Lateral male | |||||||||||
| Canal configurations Vertucci’s Classification | T1a | Count | 44 | 47 | 49 | 47 | 46 | 46 | 50 | 45 | 374 | 93.5% | ||||||
| T3b | Count | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0.25% | |||||||
| T5c | Count | 6 | 3 | 1 | 3 | 4 | 4 | 0 | 4 | 25 | 6.25% | |||||||
| Total | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 400 | 100% | ||||||||
a. Type one (single canal from the pulp chamber to the root apex.) b. Type three (one canal leaves the pulp chamber and divides into two smaller canals which later merge again to exit through one canal.) c. Type five (single canal exiting the pulp chamber which divides into two canals with separate apical foramina.) | ||||||||||||||||||
Table 4: Canal Configurations (Vertucci’s Classification) in Maxillary Anterior Teeth by Position and Gender.
Table 4 provides a detailed breakdown of canal configurations in maxillary anterior teeth, categorized by position (left and right) and gender. According to Vertucci's classification, Type 1 configuration (single canal from the pulp chamber to the root apex) is the most prevalent, observed in 93.5% of the sample. Type 5 configuration (single canal exiting the pulp chamber and dividing into two canals with separate apical foramina) accounts for 6.25% of cases, while Type 3 (one canal leaving the pulp chamber and dividing into two smaller canals which later merge) is scarce, seen in only 0.25% of the sample. This information is crucial for endodontic treatment planning and highlights the importance of thorough diagnostic imaging. See Figures (2 and 3).
Vertucci's Classification of Root Canal Morphology in Maxillary Anterior Teeth
A comprehensive analysis of root canal configurations in maxillary anterior teeth, categorized by position and gender, revealed a predominance of Type 1 morphology, as per Vertucci's classification. This configuration, characterized by a single canal extending from the pulp chamber to the root apex, was observed in 93.5% of the sample.
While Type 5 morphology, involving a single canal dividing into two with separate apical foramina, accounted for 6.25% of cases, type 3 morphology, where a single canal splits into two and later merges, was exceedingly rare, occurring in only 0.25% of the sample.
These findings underscore the importance of thorough diagnostic imaging for effective endodontic treatment planning, as variations in root canal anatomy can significantly influence treatment outcomes.
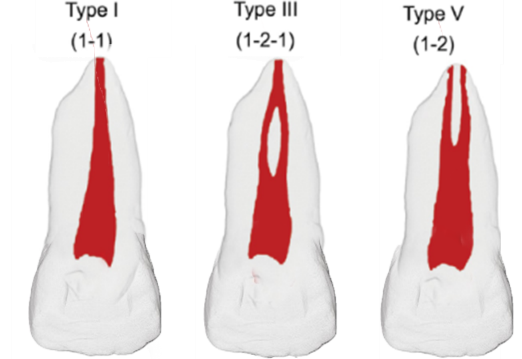
Figure 2: Vertucci's classification of root canal morphology from type I, type III, and type V.
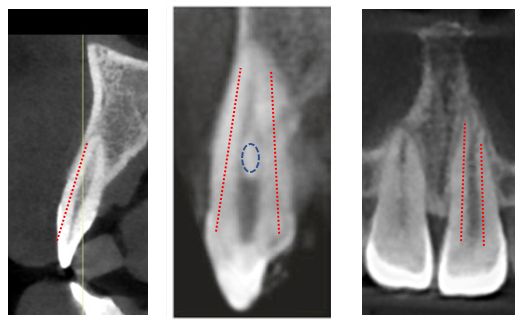
Figure 3: Canal configurations in Vertucci's classification type I, III, and type III and type V.
Ahmed's classification, utilizing the notation "O" for orifice, "C" for canal, and "F" for foramen, corroborated Vertucci's findings. The most common configuration was O1C1F1 (single canal from pulp chamber to root apex), observed in 93.8% of cases.
O1C1F2 (single canal dividing into two with separate apical foramina) was present in 6.0% of cases, and O1C2F1 (one canal dividing into two and merging again) was found in only 0.2% of cases.
These results further emphasize the prevalence of Type 1 morphology and the relatively infrequent occurrence of Type 3 and Type 5 configurations in maxillary anterior teeth.
| N=400 | Position | Frequency | % | |||||||||
| Left | Right | |||||||||||
| Central Female | Central male | Lateral Female | Lateral male | Central Female | Central male | Lateral Female | Lateral male | |||||
| Canal configurations (Ahmed Classification) | O1C1F1 | Count | 45 | 48 | 49 | 47 | 46 | 45 | 50 | 45 | 375 | 93.8% |
| O1C1F2 | Count | 5 | 2 | 1 | 3 | 4 | 5 | 0 | 4 | 24 | 6% | |
| O1C2F1 | Count | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0.2% | |
| Total | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 400 | 100% | ||
| O=orifice, C=canal, F=foramen | ||||||||||||
Table 5. Canal Configurations (Ahmed Classification) in Maxillary Anterior Teeth by Position and Gender.
Table 5 presents a comprehensive analysis of canal configurations in maxillary anterior teeth, classified according to Ahmed's system. The data is categorized by position (left and right) and gender.
The most prevalent configuration, O1C1F1 (a single canal from the pulp chamber to the root apex), was observed in 93.8% of the sample (Figure 4a). While less common, the O1C1F2 configuration (6%, Figure 4b) and the rare O1C2F1 configuration (0.2%, Figure 4c) underscore the importance of thorough diagnostic imaging to identify these anatomical variations. This information is crucial for effective endodontic treatment planning and execution.
a= O1C1F1, b= O1C1F2, c= O1C2F1
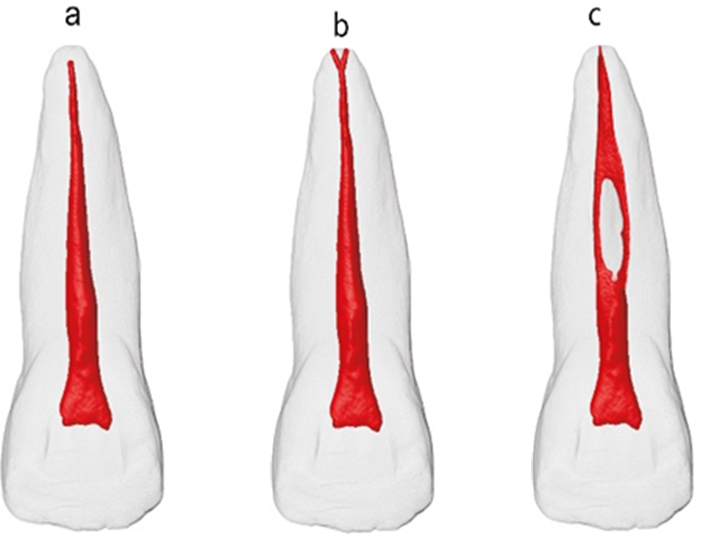
Figure 4: Ahmed classification of root canal morphology from.
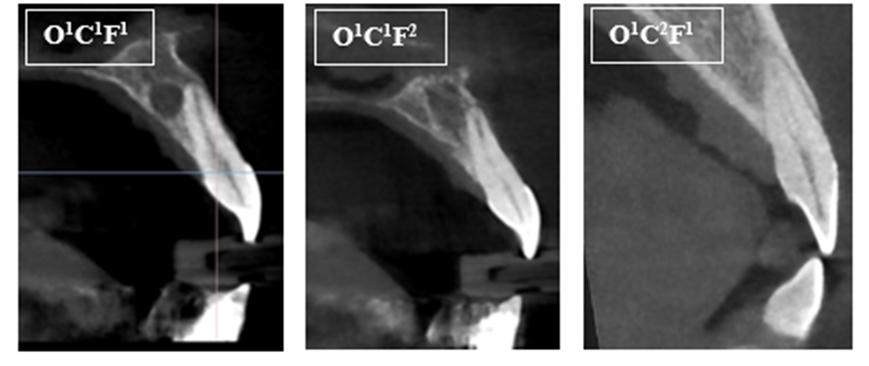
Figure 5: Canal configurations for maxillary anterior incisors teeth in Ahmed classification.
These findings suggest that the O1C1F1 configuration is the predominant type in maxillary anterior teeth. Although the O1C1F2 and O1C2F1 configurations are less frequent, their presence highlights the need for clinicians to be aware of these variations. Further research is required to investigate the underlying causes of these anatomical differences and their potential clinical implications.
No statistically significant differences were found in canal configuration based on gender (p > 0.05).
This study investigated the root and canal morphology of maxillary anterior teeth in a Yemeni population using cone-beam computed tomography (CBCT). The results revealed a high degree of consistency in these teeth, with a single root and a predominantly single canal configuration being the norm. These findings align with previous studies conducted in other populations, supporting the understanding that maxillary and mandibular incisors typically exhibit straightforward anatomy.
CBCT, a non-invasive radiographic tool, offers comprehensive external and internal features of the tooth and surrounding structures (Mozzo et al., 1998; Patel and Horner, 2009). It has a lower radiation dose and is cheaper than a CT scan. Additionally, CBCT voxels are isotropic, ensuring accurate measurements (Kaya et al., 2011; Patel and Horner, 2009). Previous investigations have demonstrated CBCT's reliability in visualizing root canal morphology and its suitability for cross-sectional studies with large sample sizes (Altunsoy et al., 2014; Blattner et al., 2010).
The utilization of CBCT imaging allowed for precise three-dimensional visualization and analysis of the root canal system, enabling accurate identification and categorization of different canal configurations. While variations were observed, the relatively infrequent occurrences of Type 3 and Type 5 configurations highlight the importance of acknowledging these possibilities while recognizing that the vast majority of these teeth present a simple canal morphology.
The new classification system by Ahmed et al. offers a valuable addition to existing systems. By combining the number of roots and canals into a single code, it provides a more comprehensive and informative description of root canal anatomy. This detailed classification can facilitate improved communication and documentation among dentists, ultimately contributing to enhanced treatment planning and outcomes.
The inclusion of two different classification systems in this study aimed to clarify aberrations and their specific regions of occurrence. The Vertucci classification system, while universal and widely known, may not provide exhaustive information about the tooth and its anomalies, and it does not classify the number of roots (Karobari et al., 2021). In contrast, the new classification system by Ahmed et al. offers a single code that classifies the tooth with the number of roots and canal morphology (Ahmed et al., 2017). Additionally, it helps us understand complex intercanal communications in teeth.
This CBCT study reveals that a majority of permanent maxillary anterior teeth in the Yemeni population exhibit a single root and a single root canal morphology. Although variations in canal configurations, as defined by Vertucci's and Ahmed's classifications, were observed, they were relatively uncommon. These findings emphasize the need for comprehensive diagnostic evaluations while recognizing that the majority of these teeth possess a simple canal anatomy. The novel classification system proposed by Ahmed et al., with its detailed coding system, offers a valuable tool for facilitating communication and documentation among dental professionals, ultimately contributing to enhanced endodontic treatment outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
