
Case Report | DOI: https://doi.org/10.31579/2692-9562/065
Assistant professor, Radio-diagnosis Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India-313001
*Corresponding Author: Rajaram Sharma, Assistant professor, Radio-diagnosis Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India-313001
Citation: Rajaram Sharma, (2023) Role of contrast enhanced computed tomographic evaluation in the management of Wharton’s duct calculus in older age group patients. Journal of Clinical Otorhinolaryngology 5(1); DOI: 10.31579/2692-9562/065
Copyright: © 2023, Rajaram Sharma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 November 2022 | Accepted: 14 December 2022 | Published: 05 January 2023
Keywords: tomographic evaluation; wharton’s duct calculus; group patients
The salivary glands are exocrine type of glands that produce saliva which help in digestion, produce moisture to mouth and protect teeths to decay. The most common disease of the salivary glands is formation of stones i.e. known as sialolithiasis, affecting 12 in 1000 of the adult population. Males are much more affected than females and children are rarely affected.
A 64 years old male presented to ENT department with progressive, painless swelling in right submandibular region. On physical examination the swelling is nontender and fixed, overlying skin was normal. He had a history of calculus in right submandibular gland few years back, for which he underwent surgery for removal of calculus. Keeping the past history in mind, ultrasonography of right neck was advised. The right submandigular gland was bulky and hypoechoic with increased internal vascularity. Parenchyma demonstrated multiple tiny hyperechoic calculi. A fairly large calculus (approx.20 mm ) in the duct of the submandibular gland in right floor of mouth region.[Figure 1A,1B & 1C] Considering the age of the patient, recurrence of the disease and painless progressive swelling, contrast enhanced CT neck was done to rule out any neoplastic etiology or any intraparenchymal complication. CECT scan revealed enlarged (measuring approx 28 x 29 x 37 mm) and relatively altered CT attenuation and heterogenous enhancement of right mandibular gland with irregular margins and surrounding inflammatory fat stranding. A large calculus (approx 10.5 x 9 x 12.7 mm) with 800-900 HU value seen near posterior part of right mylohyoid muscle, confirmed the USG findings. Multiple, tiny intraductal calculi are seen throughout the parenchyma [Figure 2A,2B,2C & 2D]. CECT helped us to delineate the duct with intraductal contents, differentiate inflammatory etiology with neoplastic and also ruled out intraparenchymal abscess formation.
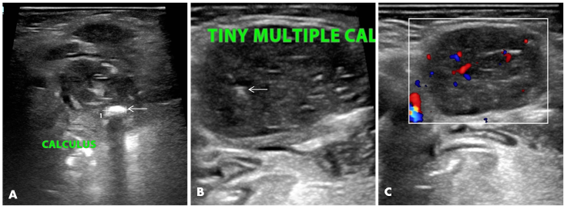
Figure 1. Ultrasonography images of the right submandibular gland. (A) The image demonstrates a large calculus in the duct of the submandibular gland duct (white arrow). (B) Right submandibular gland appears hypoechoic with multiple intraductal calculi in the parenchyma (white arrow). (C) Subtle increased vascularity in the right submandibular gland.

Figure 2. Contrast-enhanced computed tomography images of neck region at the level of both submandibular glands. (A) Axial plane at the level of the floor of the mouth showing a large calculus (white arrow) in the Wharton’s duct adjacent to the right submandibular gland (asterisk). (B) The axial plane demonstrates intraductal calculi in the parenchyma (white arrow) with fat strandings in the perisubmandibular region (black arrow).
The right submandibular gland appears relatively bulky and shows altered CT attenuation(C & D). coronal and sagittal plane respectively, demonstrate obstruction of right Wharton’s duct with proximal dilatation of the duct and periglandular inflammatory changes (black arrow).
Due to age of the patient, recurrence of the disease, inflammatory features on CECT without tenderness on examination, surgeon counseled the patient for complete excision of the gland. Excised submandibular gland specimen was sent for histopathological examination revealed features of
The most common gland involvement is submandibular gland (92%) then parotid gland (6%), sublingual gland (2%), in which ducts are being more frequently affected than the parenchyma. For evaluation of calculi non contrast computed tomography (NCCT) neck is recommended because of its sensitivity to detect calcification but there is a one drawback of NCCT is that it provides less information about duct dilatation and intraductal or glandular pathology than contrast enhanced CT (CECT). CECT neck has been used for the evaluation of complicated stone disease in an older age group, suspected inflammatory or neoplastic process after detection of calculi on NCCT [1,2,3]. The purpose of this study was to highlight role of CECT alone in the detection of salivary duct calculi and associated complications in older age group.
Unilateral, painless progressive neck swellings in older age group of patients needs detailed diagnostic work up to rule out neoplastic etiology. Contrast enhanced computed tomography not only tells about the presence or absence / number of the calculi but also delineate the duct status, neoplastic etiology causing recurrent intraparenchymal/intraductal calculi and intraparenchymal complications of the recurrent sialolithiasis. Open surgical procedures are preferred over laparoscopic stone removal in case of larger sized obstructed chronic intraductal/multiple intraparenchymal, intraductal calculi with diffuse inflammatory changes in the submandibular gland.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
