
Research Article | DOI: https://doi.org/10.31579/2641-0419/035
1 Faculty of Medicine, Tetovo Republic of North Macedonia.
2 Department of Internal Medicine Faculty of Medicine, Tetovo Republic of North Macedonia.
3 Department of Cardiology Faculty of Medicine"Ss Kiril and Metodij" University Skopje Republic of North Macedonia
4 Department of Cardiology Faculty of Medicine M. Teresa Tirana Republic of Albania.
6 Department of Cardiology Medical Center Dures Republic of Albania.
8 Private Health Institute of family medicine "Florenc "Tetovo Republic of North Macedonija.
10 Private Health Institute”Rostusha”Debar Republic of North Macedonia.
11 Faculty of Medicine, Tetovo Republic of North Macedonia.
*Corresponding Author: Ylber Jani, Faculty of Medicine,Tetovo Republic of North Macedonia.
Citation: ani Y., Rexhepi A., Pocesta B., Kamberi A., Ferati F., et al. (2020) Role of inflammation on the control of the arterial hypertension among patients with metabolic syndrome. J. Clinical Cardiology and Cardiovascular Interventions, 3(3); Doi:10.31579/2641-0419/035
Copyright: © 2020 Ylber Jani, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 January 2021 | Accepted: 03 February 2021 | Published: 07 February 2021
Keywords: C-reactive protein; control of BP in patient with Metabolic Syndrome.
BACKGROUND: It is widely accepted that hypertension is a pro-inflammatory disease and that the immune system plays a vital role in mediating hypertensive outcomes, end organ damages . and modulation of hypertensive pathology [2]. Patient with MetS usually present increased levels of C-reaktive protein (CRP) wich is a prototypic marker of inflammation [5], however the data of the influence of incresed levels of CRP on the control of the aterial hypertension in patients with MetS, are scarce.
OBJECTIVE: We sought to determine the incresed CRP levels influence on the control of the aterial hypertension in patients with MetS.
METHODS: We conducted a multicenter observational cross-sectional study. The study population recruited from a coule of outpatient clinic between june 2018 and june 2019. The population study consisted of 420 patients with MetS aged ≥ 18 years, divided in two groups:211 with level of CRP>3mg/l , and 209 participans with CRP level <3mg/l.
RESULTS: Among those with CRP level > 3mg/l(N=211) controlled BP according to evidence and current guidelines, was achieved in 23.6% of participans, whereas among those with CRP level <3mg/l(N=209) controlled BP was achived in 48.3%; p=0.000). There was independent association of CRP levels >3mg/l with uncontrolled BP (OR=3.1, 95%CI 2.06 - 4.75). There were signifiacant association of uncontrolled BP with: uncontrolled glycemia (OR =1.4,95%CI 0.97-1.84); increased BMI (OR=4.4; 95%CI 3.02-4.05) and five risk factors for MetS.(OR=2.3, 95%CI 1.93-2.81).
CONCLUSIONS: We think,we brought some good evidence,in our present study ,that patients with MetS and higher CRP level have a higher prevalence of unconrolled BP.
We conducted a multicenter observational cross-sectional study. The study population was recruited from our outpatient clinic between juni 2018 and juni 2019. Subjects who fulfilled the criteria for MetS according to the results of recent laboratory tests were prospectively evaluated.
The population consisted of 420 patients with MetS aged ≥ 18 years, divided in two groups: 211 participans (100 females and 111 males) with level of CRP>3mg/l, and 209 participans (104 females and 105 males) with level of CRP<3mg/l).
All participants underwent a comprehensive medical history and physical examination. Resting ECG, anthropometrics, measuring of blood pressure according to standard protocol (obtained after 10 min of rest in the sitting position, expressed as the average of 3 consecutive measurements), the mean systolic and diastolic blood pressure recording during the study period, were calculated. Hypertension was defined be current ESC/ESH guidelines for the management of arterial hypertension as office systolic blood pressure (SBP) values ≥140 mmHg, and/or diastolic blood pressure (DBP) values ≥90 mmHg and/or current anti-hypertensive therapy [6]. Uncontroled BP, was defined defined be current ESC/ESH guidelines for the management of arterial hypertension [5]. The blood pressure was considered to be controlled if the calculated mean systolic and diastolic blood pressure recording during the study period was found to be less than 140/90mmHg. Among adults younger than 60 years and less than 150/90mmHg.in general population aged ≥60 years. Diabetes mellitus was defined as a fasting serum glucose level ≥126 mg/dL and/ or current medical therapy with an oral hypoglycemic agent and/or insulin6.Body mass index (BMI) was calculated as weight (kg) divided by the square of the height (m2).Weight was measured with weight balance scales, and height with stadiometer. Waist circumferenceWCi, was reported in cm.
An overnight fasting blood sample, was drawn from each patient to determine: blood glucose, lipid profile tests total serum cholesterol (TC), serum High density lipoproteins cholesterol (HDL-C), serum triglycerides (TG).The sample analysis was performed using standard biochemical analytical methods. Plasma CRP levels was measured using latex particle-enhanced immunoassay with the mephelometry (Roche Swiss). Consistent with recommendations from Centers for Disease Control and Prevention[7] (a CRP cutpoint of 3.0mg/L), was used to differentiate high-risk and low-risk group.
Exclusion criteria, included a diagnosis of dementia senilis, secondary hypertension, serum creatinine level >2mg/dl, age under 18 years and over 79 years.
MetS was defined according to the harmonized definition of the International Diabetes Federation and other organizations [8], that three or more out of five following criteria are considered as MetS: (1) central adiposity {Waist circumference (WCi)} >102 cm in men and >88cm in women [9]); (2) serum HDL-C < 50 mg/dL in women or < 40 mg/dL in men; (3) serum triglyceride levels > 150 mg/dL; (4) SBP ≥ 140mmHg or DBP ≥ 90mmHg or use of antihypertensive drugs;(5) the presence of diabetes mellitus(DM) or use of anti-diabetic drugs. A standardized case report form was used to collect data from medical record and was send to the central data management unit.
The study is in compliance with the Declaration of Helsinki. All patient that participated in this study were written informed, consent was obtained from all participating patients before they were enrolled into the study.
Results are expressed as mean and ±SD, or as percentage. A simple descriptive analysis was performed for the general characterization of the sample and distribution of variables. The distribution of variables was tested for normality using the Kolmogorov-Smirnov test, and the heterogeneity of variances was evaluated by Levene's test. To compare baseline characteristics and echocardiographic findings between groups, we used Student,s unpaired t test for continuous data, Mann-Whithey U -test for continuous data with abnormal distribution, and X2-test for categorical data. The association between variables were analyzed using logistic regression. Odds ration (OR) and 95% confidence interval (CI) were estimated by logistic regression. A, p value <0.05 was considered statistically significant for a confidence interval of 95%.Data were coded, entered and analysed using SPSS software package (SPSS 19.0).
A total of 420 subjects with MetS enrolled in our study, stratified in two groups:209 participans (47.5% females and 50.2% males) with level of CRP < 3mg/l, and 211 participans (47% females and 53% males) with level of CRP > 3mg/l, completed the survey and had data for 1-year medical record review. A mean of 3.4 BP recordings were obtained for each participans.
Baseline demographic, anthropometric and laboratory, characteristics by group are displayed in (Table 1)
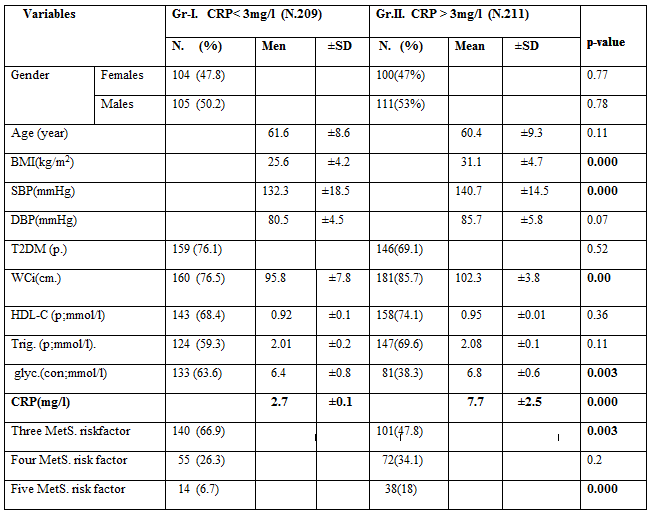
Values are mean ± SD;y=year; BMI:body mass index;SBP:systolic blood presure;DBP:diastolic blod presure;T2DM(p: presence of diabetes mellitus type 2;serumHDL-C(p)-high.density cholestero ppresence;serum Triglicerides;hs-CRP: C-reative protein;WCi:presence of increased weist circumference;BPH-presemnce od artrial hypertension;glic:glicemia controll;
No significant differences in: age, gender. Diastolic BP, were observed between groups. Participans with level of CRP >3mg/l had significantly higher means: SBP (140.7 ±14.5 vs. 132.3±18.5 p= 0.000), BMI( 31.1 ±4.7 vs. 25.6±4.2 p=0. 000), WCi (102.3 ±3.8 vs. 95.8 ±7.8 p=0.00); uncontrolled glycemia(6.8±0.6 vs. 6.4±0.8 p=0.003) and number of risk factors for MetS {frequency of presence five risk factor for MetS was higher among participans with level of CRP > 3mg/l (18 % vs. 6.7%; p= 0.000)}.
(Table 2), presens the frequency of controlled BP in participans with MetS and different level of CRP. Among those with level of CRP > 3mg/l (N=211) controlled BP according to evidence and current guidelines, was achieved in 23.6% of participans,whereas among those with level of CRP< 3mg/l(N=209) controlled BP was achived in 48.3%; p=0.000).The diference was found to be statistically significant.
Table 2. Frequency of controlled BP among patients with MetS stratified by CRP levels (No.420).
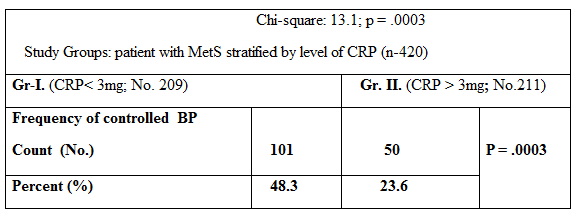
Over all frequency of controlled BP (in all participans enrolled in present study), was 38%.
In a logistic regression (Table. 3), there was independent association of CRP levels >3mg/l with uncontrolled BP (OR=3.1, 95%CI 2.06 - 4.75). There were signi-fiacant association of uncontrolled BP with: uncontrolled glycemia (OR =1.4,95%CI 0.97-1.84); increased BMI (OR=4.4; 95%CI 3.02-4.05) and five risk factors for MetS. (OR=2.3, 95%CI 1.93-2.81).
Table 3. Logistic Rgresion Model: Association of uncontrolled BP with: CRP levels (>3.0mg/L), uncontrolled glycemia, increased BMI and five risk factor for MetS.
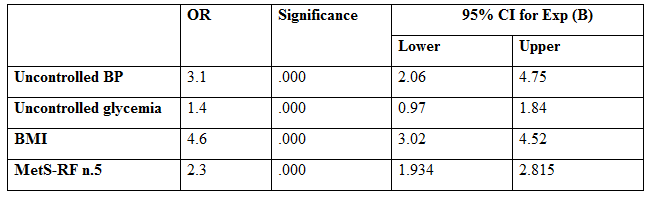
BP:blood presure;MetS-RF n.5-:five risk factors for MetS;DM:Diabetes Mellitus and BMI:Body mass index. OR* >1.
In this study we found that patients with MetS and higher levels of CRP had significantly higher prevalence of uncontrolled BP than did those with MetS and lower levels of CRP. Results that confirmed our hypothesis. Low-grade inflammation is now a recognized hallmark of hypertension, and ther is an expanding literature regarding the role of inflammation and inflammatory cells in hypertension, in particular T lynphocites are now thought to have a central role in the development of hypertension and related organ injury [10] Based on the cenral role played by the cytokine milieu in determining lymphocyte differentiation and activation, differences of cytokines levels likely contribute to observed difference on the prevalence of uncontrolled BP in present study, and will impact the overall physiological outcome of an inflammatory response. The CoLaus Study reported that serum CRP, interleukin-6 and THF-α levels were positively associated with BP [11,12] Also, Grundy SM et all, suggests a significant association among inflammation, hypertension, and the metabolic syndrome[13]. Nevertheless, despite an association between high CRP levels and hypertension, a causal relationship has not been demonstrated. In fact, Smith et al.used a Mendelian randomization approach to examine a possible causal relationship analyzing the association of the 1059G/C polymorphism in the human CRP gene with hypertension, the work failed to confirm a causal relationship between CRP and blood pressure [14].
In our study, BP was controlled at 38% patient only. This result is consistent with previous findings that patients with hypertension and MS have an elevated prevalence of uncontrolled BP [15,16]. The study results allow evaluating the effetivity of hypertension treatment as for drug choise, decrease of sBP and dBP associated with a certain drug, a drug combination, and therapeutic inertia in these patients.
We also found that BP control was worse among patients with MetS and higher CRP levels in the presence of more MetS risk factors. It appears that there is an interaction between hypertension and metabolic disorder factors, although the mechanisms that are involved in this interaction remain unclear. Results in present study are consistent with previous findings[17]. It has been suggested that metabolic disorder factors have additive effects on BP control and cardiovascular disease. Arcucci et al. have reported that BP control worsens in the presence of more metabolic disorder factors [17] These data sugest that presence of more metabolic disorder factors, decrease the probability of BP control. We found association of number of risk factors of MetS and higher levels of CRP. However, it is unknown whether the number of MetS risk factors can influence the levels of CRP. Previeous study demonstrated that number of risk factors did not influence the levels of CRP in patients with MetS [18]. Also in present study we found association of highe levels of CRP in patient with uncontrolled BP and elevated levels of triglycerides, low HDL levels, obesity and uncontrolled glycemia. Results in present study are consistent with previous findings [19-21].
The study employed a cross-sectional design, and as such, the results could show only factors associated with uncontrolled hypertension. Study design limited to make causal inferences regarding increased CRP levels and control of arterial hypertension in patient with MetS. A larger sample would certainly increase the statistical power of the study, and probably some differences would therefore become more expressive. Despite some methodological limitations, this study clearly demonstrated a relationship between increased CRP levels and control of BP in patient with MetS.
Clinical Implications
These data provide further evidence that poor BP control is common in patients with MetS, and further investigations on the immune reactivitiy in hypetension may result in the identification of new strategies for the treatment of the disease. Therapeutic interventions to reduce activity of immunity may prove beneficial in reducing consequences of hypertension including: myocardial infarction, heart failure, renal failure and stroke.
We think, we brought some good evidence, in our present study, that patients with MetS and higher CRP level have a higher prevalence of unconrolled BP. These results indicate that presence of an subclinical inflammatory process in the natural history of MetS, through presence of high CRP levels, negatively affect BP control in patients with MetS. Measurement of this inflammatory protein may help to determine individuals cardiovascular risk and activity of immune system, it might be a novel therapeutic target for the treatment of high blood pressure in these individuals.
Materials- Agim Zeqiri;Dali Lala, Fatmir Ferati;Arben Mirto;Data collection/pro-cessing-Sotiraq Xhunga;Artur Serani;Ylber Jani; Analysis/interpretation-Ylber Jani;Ahmet Kamberi;Atila Rexhepi; Bekim Pocesta;LiteratureSearch- Ylber Jani;Agin Zeqiri;Dali Lala; Fatmir Ferati;Artur Serani. Critical Reviews-Ahmet Kamberi.
All authors read and approved the final manuscript.
The authors reported no conflict of interest and no funding has been received on this work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
