
Case Report | DOI: https://doi.org/10.31579/2641-0419/525
1Sandwell and West Birmingham NHS Trust, Birmingham, United Kingdom.
2Aston University, United Kingdom.
3University of Birmingham, United Kingdom.
*Corresponding Author: Vinoda Sharma, Sandwell and West Birmingham NHS Trust, Birmingham, United Kingdom.
Citation: Vinoda Sharma, Fairoz Abdul, Ahmed Hassan, Keshav Kulkarni, Derek Connolly, (2025), Robust Computed Tomography Coronary Angiography (CTCA) Multi-Disciplinary Team (MDT) Meetings: Purpose, Process and Set-up, J Clinical Cardiology and Cardiovascular Interventions, 8(14); DOI:10.31579/2641-0419/525
Copyright: © 2025, Vinoda Sharma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2025 | Accepted: 30 September 2025 | Published: 16 October 2025
Keywords: computed tomography coronary angiography; multi-disciplinary team; percutaneous coronary intervention
Multi-disciplinary team (MDT) meetings form the heart of patient centred care. Defined standards also exist for Heart Team or Cardiac MDT meetings. Despite progress in the field of cardiovascular imaging especially Computed Tomography Coronary Angiography (CTCA), there does not appear to be either mandate or a quality standard for a CTCA MDT. In this article, we describe the purpose, process and set-up of a robust CTCA MDT and describe our experience of the same.
Multi-disciplinary team (MDT) meetings form the heart of patient centred care especially for those who have complex comorbidities. Published data on quality standards for MDTs is quite extensive [1-3]. Defined standards also exist for Heart Team or Cardiac MDT meetings [1, 2]. An MDT mandates a clear purpose, goal and a patient centric approach with management decided by diverse expertise and implemented by effective communication.
In 2016, the updated National Institute for Clinical Excellence (NICE) guidance advised that Computed Tomography Coronary Angiography (CTCA) as the first line investigation for patients with chest pain of suspected Cardiac origin [3]. As a consequence there was a veritable explosion in requests for CTCA for cardiac sounding chest pain and the demand continues to grow.
CTCA is also emerging as an imaging test to not only diagnose coronary artery disease (CAD) but also help in procedure planning when percutaneous coronary intervention (PCI) is considered.
Despite these developments there does not appear to be either mandate or a quality standard for a Computed Tomography Coronary Angiography (CTCA) MDT.
We perform over 2000 diagnostic CTCA scans annually, serving a population of over half a million residents in our catchment area. Our hospital is situated in the centre of the second biggest city in the United Kingdom (UK) with a multi-ethnic, socio-economically deprived population. Our CTCA reporting service involves two pathways: a novel “One Stop Cardio Radiology Integrated Service (OSCRIS)” and a Standard CT Patient Pathway (SCTPP) service [4]. The OSCRIS pathway, started in 2012, is performed jointly by a level 2 Radiologist and a level 2 Cardiologist who report the CTCA and initiate a management plan on the same day. The SCTPP pathway is performed by a solo level 3 Radiologist.
We describe how to establish a robust CTCA MDT and detail our experience of the MDT.
CTCA MDT caveats
Although the CTCA service was established in 2012, the bimonthly CTCA MDT was only formally started in August 2020.
Purpose:
The purpose of the CTCA MDT is to ensure quality of reporting and maintain standards including quality control (QC), as part of good governance. For QC, the CTCA images are discussed in a blinded, “no-blame” manner with agreement or disagreement of the findings ± corroboration with invasive angiography if this has been performed. Other categories of cases discussed include: interesting findings, clinical management of cases and corroboration of findings.
Process:
The CTCA MDT was set up as a virtual teams meeting and the quorate includes a chair (the CTCA lead- currently a Cardiologist), at least one Radiologist and one other Cardiologist. The chair is a senior clinician with at least level 2 CTCA accreditation and a minimum of 2 years’ experience at reporting CTCA. It is the chair’s responsibility to ensure that the MDT is quorate. The CTCA chair ensures the smooth and effective functioning of the MDT, ensures the CTCA images are available on the day of discussion and documents/communicates the consensus decision. The referring consultant is required to be present for discussion of their case to take place.
Set-up:
Cardiologists and Radiologists upload the required cases for discussion onto a secure, access-controlled folder on the Trust’s shared drive. The minimum dataset for the referral includes the reason the CTCA was requested, the patient’s comorbidities and the question to be answered.
Imaging software and requirements: Trust computers are required to be available for the MDT with the necessary imaging software (Syngovia@ software at our centre) installed for the MDT for ease of review. Cases are discussed in a step wise manner along with review of the CTCA images and any other imaging modality that might help with the discussion including invasive angiograms, intracoronary imaging, echocardiograms and cardiac magnetic resonance (CMR) imaging. Attendance is marked on the spread sheet and the outcome of the MDT is documented on the spread sheet. Participation is open to the entire Cardiology team.
Any actionable steps are taken by the referrer and communicated to the patient and the team managing the patient. The referring consultant is usually the operator who performed the CTCA.
Retrospective evaluation of our CTCA MDT:
We performed retrospective evaluation of the CTCA MDT cases and outcomes between August 2020 and May 2025,
The CTCA cases discussed were classified as follows (table 1):
1) Quality Control (QC)
2) Interesting CTCA
3) Clinical management
4) Corroboration of findings on CTCA ± management
Over a period of 53 working months, 298 CTCAs were discussed (~3 cases per MDT). Approximately 10% of the cases were for QC (others: Interesting CTCA: 6.4%; Clinical management: 55.0%; Corroboration of findings ± management: 29.5%). The number of QC cases discussed increased over the years. Clinical management queries formed over 50% of the cases discussed. Of those who were discussed for clinical management, nearly three fourths had a change in management -for example (figure2): those with chronic total occlusion (CTO) and the necessity to intervene, the need for non-invasive physiological assessment of a coronary lesion with FFR-CT, exotic cases which required urgent surgical discussion such as sinus of valsalva aneurysm causing coronary compression or aggravation of Kawasaki disease requiring urgent immunotherapy.
Quality Control
| Interesting CCT | Clinical management | Corroboration of findings ± management | |
| Number of CCTs discussed | 27 (9.1%)
| 19 (6.4%) | 164 (55.0%)
| 88 (29.5%)
|
| Total number of cases | 298 CCTs discussed over 53 working months | |||
Table 1: Reasons for CCT discussion at MDT
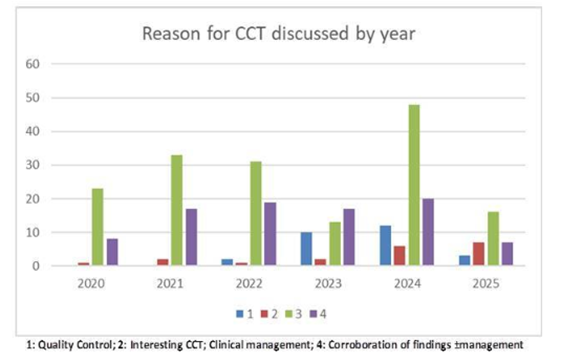
Figure 1: CTCA cases discussed over the individual years
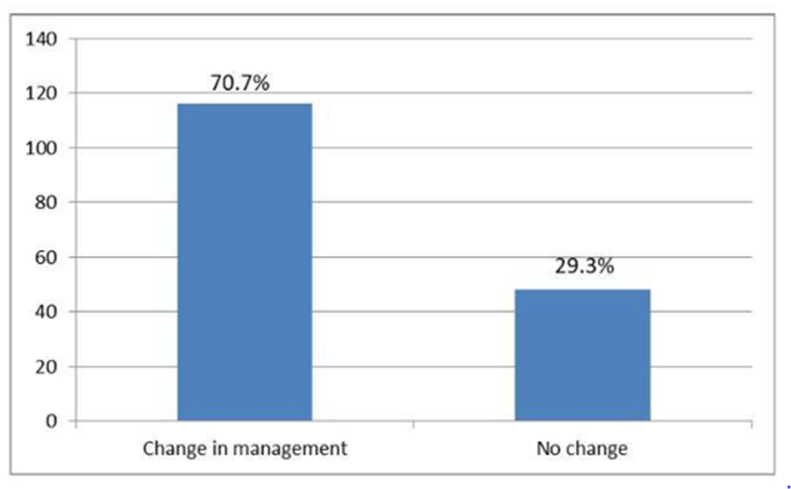
Figure 2: Change in clinical management due to CTCA MDT
Since the CTCA MDT was formally initiated, regular QC has improved the knowledge and reporting of both Cardiology and Radiology colleagues. Feedback from the wider Cardiology team indicates that CTCA reports are more coherent and accurate. Colleagues attending the CTCA MDT have expressed how the MDT has contributed to their improved understanding of the coronary and cardiac anatomy including differentiation of artefact from plaque or normal anatomy. Subsequent MDTs have resulted in reduced time to clinical decision making, enhanced patient care, learning and education. On many occasions, clinical perspective and opinions were added to the final CTCA report as an addendum, which ensured accurate evidence-based patient management. Regular discussion of a variety of cases has improved the confidence of the CTCA operators to present CTCA findings at other joint Heart MDT Discussions. Since initiation, the CTCA MDT has evolved to also be utilised as a forum for invited talks from national experts, discussion of guidelines/ CTCA-relevant publications and discussion of research ideas and concepts.
The authors recommend that all centres that perform CTCA have a dedicated and regular CTCA MDT with the caveats as discussed above for improvement of patient care.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
