
Research Article | DOI: https://doi.org/10.31579/2578-8965/162
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, NYU Langone Health, 550 First Ave., NBV 9N2, New York, NY 10016,
*Corresponding Author: Myah M. Griffin, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, NYU Langone Health, 550 First Ave., NBV 9N2, New York, NY 10016.
Citation: Myah M. Griffin, Alexis Engel, BA, Shilpi Mehta-Lee, Julie Nusbaum, Michael Golpanian, BS, (2023), Risk Assessment Model for Postpartum Venous Thromboembolism Prevention in Patients with Systemic Lupus Erythematosus, J. Obstetrics Gynecology and Reproductive Sciences, 7(3) DOI:10.31579/2578-8965/162
Copyright: © 2023, Myah M. Griffin. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 April 2023 | Accepted: 18 April 2023 | Published: 25 April 2023
Keywords: systemic lupus erythematosus; venous thromboembolism; postpartum
Background
Patients with Systemic Lupus Erythematosus (SLE) may be at increased risk for developing a venous thromboembolism (VTE), particularly in the postpartum period. The Royal College of Obstetricians and Gynaecologists (RCOG) guideline for postpartum VTE prophylaxis is often used to triage which patients should get VTE prophylaxis. In this RCOG guideline, a score ≥ 3 drives a formal recommendation for postpartum anticoagulation. RCOG is unique in its inclusion of “active SLE” as an actionable VTE risk factor (adding 3 points). We sought to determine if a cohort of postpartum patients with a known history of SLE a) qualify as having “active” SLE by standard rheumatologic criteria b) have other risk factors for VTE c) received the recommended prophylaxis based on RCOG VTE risk assessment scoring and d) had a postpartum VTE.
Objective
To assess the application of the RCOG venous thromboembolism (VTE) risk model on a cohort of postpartum patients with a history of Systemic Lupus Erythematosus (SLE).
Study Design
This is a secondary analysis of an ongoing patient registry of women with SLE from 2016-2022. There were 49 SLE patients with 55 pregnancies using Definitions of Remission in SLE (DORIS) criteria to determine SLE disease activity. RCOG risk assessment model scoring was calculated for each patient prior to and after delivery. The primary outcome was the qualification of “active SLE” by standard rheumatologic criteria and assessment of recommendations for VTE prophylaxis based on RCOG VTE risk assessment scoring. Data were analyzed using Fisher’s Exact test, chi-square test, and Mann-Whitney U test with significance defined as p<0.05.
Results
In the study cohort, 34 pregnancies (61.8%) were in DORIS remission at delivery. Twenty-one pregnancies (38.2%) were not and scored 3 points on the RCOG VTE risk model. Of these pregnancies, only 19% (n=4) were recommended for VTE prophylaxis by the obstetrical provider despite RCOG score ≥ 3. Only 35.7% (n=5) of pregnancies in DORIS remission, but with 3 points for non-SLE related VTE risk factors (n=14), were recommended for VTE prophylaxis. Of the 20 pregnancies in remission with an RCOG score < 3 after assessing all risk factors, 15% (n=3) were nevertheless recommended for VTE prophylaxis. No patients had a postpartum VTE regardless of therapy.
Conclusion
These data reveal a need to improve upon providing postpartum VTE prophylaxis to SLE patients not in remission while also recognizing a diagnosis of SLE alone should not equate with active disease. Moreover, SLE patients in remission may still warrant VTE prophylaxis if other non-SLE related risk factors are present.
Based on 2016-2018 Center for Disease Control (CDC) Pregnancy Mortality Surveillance System data, venous thromboembolisms (VTE) are responsible for 9.4% of pregnancy-related deaths, fifth behind hemorrhage [1,2]. The Nationwide Inpatient Sample (NIS) from 1998-2009 demonstrated that 60% of Pulmonary Embolism (PE)-related deaths occurred after delivery compared to 26% during pregnancy [3]. The postpartum period is the period of maximal thrombotic occurrence, with peak occurrence at 1-3 weeks postpartum [4]. Pregnant patients with Systemic Lupus Erythematosus (SLE) have an even higher incidence of VTE than the general pregnant population, 62 compared to 7.2 per 10,000.5 The 2003-2011 NIS Database was used to evaluate the risk of developing VTE among pregnant patients with selected autoimmune disease. This study included an analysis of 8,040 pregnant patients with SLE which demonstrated an increased risk of deep vein thrombosis (DVT) (42/10,000 vs. 5.34/10,000 among the pregnant patient cohort) and increased PE events (aOR 9.76, 95% CI 6.13-15.55) [5]. Patients with SLE who tested positive for antiphospholipid antibodies had an elevated VTE risk and recurrent VTE risk [6].
Many of the physiologic changes that occur in pregnancy, such as decreased venous outflow due to uterine compression of pelvic vasculature, hypercoagulability and vascular trauma, all influence the increased risk of VTE in pregnancy. In the postpartum period, the continued prothrombotic state along with dehydration due to reduced blood volume and breastfeeding are factors that increase the risk of VTE [7]. Concern for the consequences of postpartum hypercoagulability has driven recommendations for prevention of VTE in pregnancy and postpartum by the American College of Obstetricians and Gynecologists (ACOG) [8]. Various risk assessment models have been created to aid in stratifying the risk of developing VTE for individual patients. The absence of pregnant patients is one of the main criticisms of currently available VTE risk assessment models, such as the modified Caprini and Padua [9-11]. The Royal College of Obstetricians and Gynaecologists (RCOG) attempted to overcome this deficit by proposing a scoring system that includes obstetrical-related risk factors, like cesarean delivery and preeclampsia, which are known to increase the risk of VTE [12,13].
In accordance with ACOG’s recommendations, NYU Langone Health Department of Obstetrics and Gynecology adopted the use of the RCOG VTE risk assessment model to assess and prevent occurrence of VTE events in obstetrical patients admitted to the hospital based on risk factors, as well as to decrease the short-term morbidity and mortality associated with VTE events. This clinical screening tool has been incorporated into our electronic medical record for completion by the obstetrical healthcare provider upon hospital admission and repeated immediately after delivery. In the RCOG VTE risk assessment model, “active SLE” is listed as a highly relevant risk factor, scoring 3 points [12]. This is noteworthy since a cumulative score > 3 drives a formal recommendation for a 6-week heparin-based thromboprophylaxis course with enoxaparin or unfractionated heparin. Although active SLE is known as a risk factor for VTE, there is no clear definition of active SLE in the obstetrical community. Accordingly, this study was initiated to address whether pregnant patients with SLE a) qualified as having “active SLE,” b) had other risk factors listed in the RCOG VTE risk assessment model, c) received the recommended prophylaxis, and d) had a postpartum VTE.
This is a secondary analysis of an Institutional Review Board-approved, prospective cohort study of 49 pregnant individuals fulfilling sufficient criteria for classification of SLE based on the American College of Rheumatology (ACR), Systemic Lupus International Collaborating Clinics (SLICC), or recent European League Against Rheumatism (EULAR)/ACR definitions whom were all enrolled in a pregnancy registry and managed by the NYU Langone Health Department of Rheumatology from 2016-2022. These individuals obtained obstetrical care and delivered at NYU Langone Health and other New York City healthcare systems. Medical records were reviewed to obtain relevant information related to SLE management, pregnancy and postpartum outcome data that may have influenced their pregnancy and postpartum VTE risks. Study participants with incomplete records were excluded.
SLE disease activity at the time of delivery was assessed by the SLE-pregnancy disease activity index (SLEPDAI) using SELENA (proteinuria only counted if an increase of UPCR >0.5 from previous visit) and Hybrid SELENA (proteinuria always counted if UPCR > 0.5) definitions for scoring proteinuria [14-16]. In addition, remission was assigned by applying DORIS (Definitions of Remission in SLE) criteria. To meet the DORIS definition of remission, patients must have a clinical SLEPDAI score of 0 and Physician Global Assessment of p less than 0.05.Patients were included if they were using antimalarials, low-dose glucocorticoids (prednisolone ≤ 5 mg/day) and/or a stable dose of immunosuppressive medications including biologics. Of note, patients can meet the DORIS criteria for remission with a total SLEPDAI of 4 if points were awarded only for active serologies [17]. If not in remission, patients were considered to have active SLE, even if a low level of activity with only one clinical domain scored.
For this study, patients in DORIS remission were identified as having “inactive SLE”, and those in DORIS non-remission were identified as having “active SLE”. Utilizing the RCOG VTE risk assessment model, RCOG scores were calculated for each pregnancy based on the relevant clinical factors present at the time of delivery and postpartum by obstetrical healthcare providers only. For those in DORIS non-remission, 3 points were assigned for “active SLE” at the time of delivery. For those in DORIS remission, no points were assigned for SLE activity. As postpartum SLEPDAI scores were not available, SLE disease activity at the time of delivery was used to calculate postpartum RCOG scores.
Statistical data were analyzed using RStudio version 4.0.3 for descriptive and bivariate statistics. Categorical variables were assessed using Fisher’s Exact test and chi-square test as appropriate. Continuous variables were assessed using Mann-Whitney U test with statistical significance defined as p less than 0.05.
Of the 49 patients included in this study, a total of 55 pregnancies were evaluated. Of the total pregnancy cohort, the median age was 32 years (interquartile range [IQR], 29-36 years) and the median body mass index was 25.0 kg/m2 (IQR, 23.0-30.9 kg/m2). Twenty-two (40%) patients were nulliparous and 53 (96.4%) pregnancies were singleton gestations. The total study cohort was comprised of the following self-reported racial/ethnic groups: African-American (n=27, 49.1%), Asian (n=9, 16.4%), White (n=16, 29.1%), Other (n=3, 5.5%), and Hispanic (n=18, 32.7%). There were 34 pregnancies in DORIS remission and 21 pregnancies in DORIS non-remission. The study cohort demographics are listed in Table 1.

Table 1: Study cohort demographics Values are given as counts (percentages), unless otherwise specified. a Values given as median (interquartile range). B Race/ethnic groups were self-reported.
The median SLEPDAI score at the time of delivery was 2.0 (IQR, 0-6) (SELENA SLEPDAI) and 2.0 (IQR, 0-5) (Hybrid SELENA SLEPDAI). The components of the RCOG VTE risk assessment model, with each of the corresponding elements scored for the cohort, are detailed in Table 2. Of those in DORIS remission, 0 pregnancies had a mild-moderate or severe SLE flare just prior to delivery compared to those in DORIS non-remission where 6 (28.6%) had a mild-moderate and 2 (9.5%) had a severe SLE flare just prior to delivery (p less than 0.001.
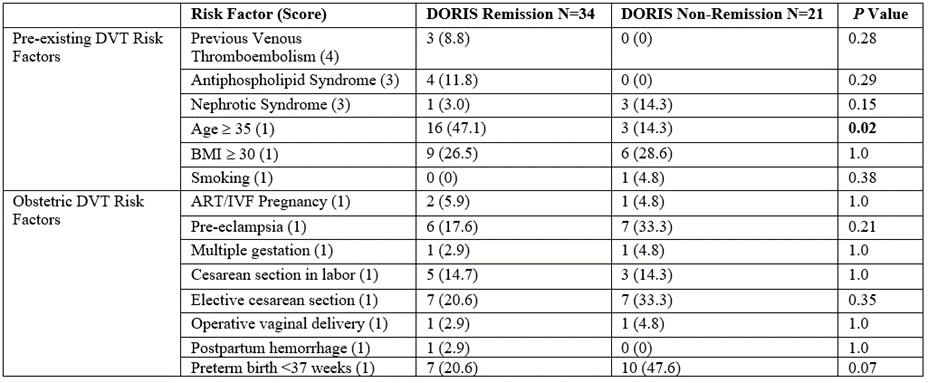
Table 2: RCOG VTE risk assessment model with scores Values are given as counts (percentages).
Of the pregnancies in DORIS remission, the median RCOG score at delivery was 1.0 (IQR, 1.0-2.0) and 2.0 (IQR, 1.0-3.0) in the postpartum period (p < 0.001) Table 3.

Table 3: DORIS remission RCOG VTE risk assessment model scoring Values are given as counts (percentages), unless otherwise specified. a Values given as median (interquartile range).
Thirty-four pregnancies (61.8%) were in DORIS remission throughout pregnancy. Only 41.2% (n=14) of pregnancies in DORIS remission scored 3 points for non-SLE related VTE risk factors. Of these pregnancies, 35.7% (n=5) were recommended for VTE prophylaxis by an obstetrical healthcare provider. Of the 20 pregnancies in DORIS remission with an RCOG score < 3 n=3)>
Twenty-one pregnancies (38.2%) were in DORIS non-remission and 100% (n=21) scored a minimum of 3 points on the RCOG VTE Risk Assessment model for “active SLE” alone. Of these pregnancies, only 19% (n=4) were recommended for VTE prophylaxis by an obstetrical healthcare provider despite RCOG score ≥ 3.
Importantly, of the pregnancies in DORIS remission, 41.2% (n=14) would still have scored at least 3 points for other obstetric, non-SLE related VTE risk factors in the postpartum period while 100% (n=21) of the pregnancies in DORIS non-remission had a postpartum RCOG score ≥3 (p less than 0.001.No patients in the study cohort had a postpartum VTE regardless of therapy.
Principal Findings
Utilizing DORIS criteria to define SLE disease activity, all pregnancies qualified as “active SLE” received a RCOG score of ≥3 with only 19% receiving recommendation for VTE prophylaxis compared to 35.7% of those in DORIS remission whom received a RCOG score ≥3 for non-SLE risk factors received recommendations for VTE prophylaxis by an obstetrical healthcare provider.
A strength of the study was the focus on determining SLE disease activity and the finding that a diagnosis of SLE should not automatically trigger thromboprophylaxis. Limitations of the study include the retrospective nature of the study, the assignment of “active SLE” in most cases by the obstetrical team, and the small sample size. Due to the small sample size, the results from this study are not generalizable as the study cohort was limited by those enrolled in our institution’s SLE pregnancy registry. Fortunately, there were no patients within the study cohort who experienced a postpartum VTE, but the study design and sample size were not conducive to determine the effectiveness and safety of this intervention to prevent adverse outcomes.
Established rheumatologic indices makes it helpful to determine which patients need VTE prophylaxis for having active SLE. The education and application of clinical indices to determine SLE disease activity for the RCOG VTE risk assessment model can direct obstetricians understanding of active SLE. Our data demonstrates that for SLE patients in disease remission at the time of delivery, points for having the diagnosis of SLE alone should not automatically be assigned on the RCOG VTE risk assessment model, however, they may still warrant VTE pharmacologic thromboprophylaxis postpartum if other non-SLE related risk factors are present.
Pharmacologic thromboprophylaxis has been instituted into obstetrical society guidelines to decrease the risk of pregnancy-related VTE and its consequences. Although no patient in the study cohort had a postpartum VTE, heparin-based thromboprophylaxis should be instituted when clinically appropriate, but with caution exercised by the healthcare team in broadly assigning disease activity for the diagnosis of SLE alone. As there is a national call to action to eliminate maternal morbidity and mortality in the United States, it is important to address and implement management interventions to decrease and eliminate pregnancy-related complications. In doing so one must always consider the risks and benefits of every decision and intervention. This study helps support recommendations for prophylaxis of VTE in pregnant patients with SLE and serves to educate treating obstetrical healthcare providers regarding what constitutes disease activity as well as identification of non-SLE related, but obstetrically related risk factors for VTE.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
