
Case Report | DOI: https://doi.org/10.31579/2693-2156/040
1 Radiology Department, Usmanu Danfodiyo University, Sokoto.
2 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
*Corresponding Author: Sule MB. Radiology Department, Usmanu Danfodiyo University, Sokoto.
Citation: Shamaki AMB, Sule MB, Dalha A, Ribah MM, Ezeh NC, Sarki H. (2022). Right pulmonary arterial thrombus in a patient with tuberculous destroyed lung syndrome: computed tomography angiographic findings and a case report., J. Thoracic Disease and Cardiothoracic Surgery, 3(2) DOI: 10.31579/2693-2156/040
Copyright: © 2022 Sule MB. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 April 2022 | Accepted: 24 March 2022 | Published: 04 June 2022
Keywords: pulmonary arterial thrombus; cta; tuberculosis; lung
Tuberculous destroyed lung syndrome (TDLS) is termed as total lung destruction from recurrent and chronic infections especially tuberculosis (TB). TDLS is almost an entity seen in adults and very rare in children. Pulmonary TB been a chronic infectious disease induces a systemic hypercoagulable state that causes pulmonary thromboembolism.
This is a forty-year-old man been managed for pulmonary TB, presented from a peripheral health facility and came for a chest computed tomography angiography (CTA) on account of suspected thromboembolism.
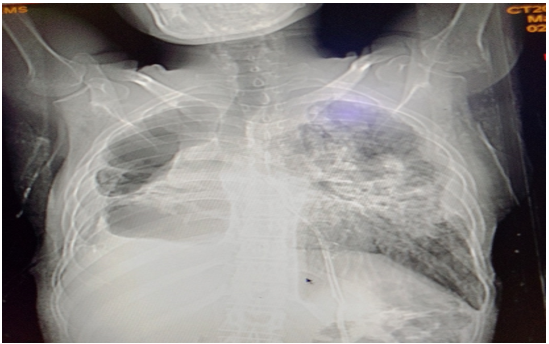
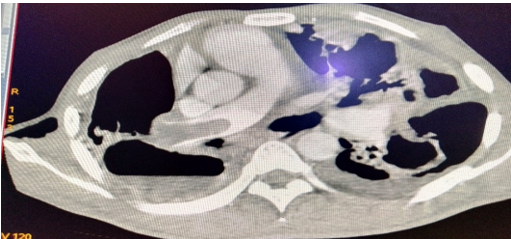
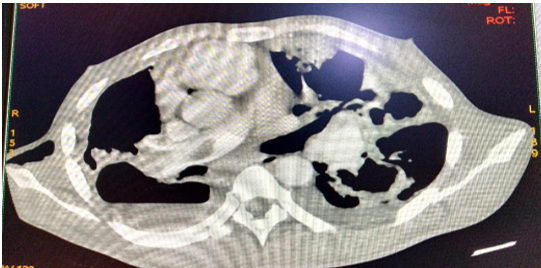
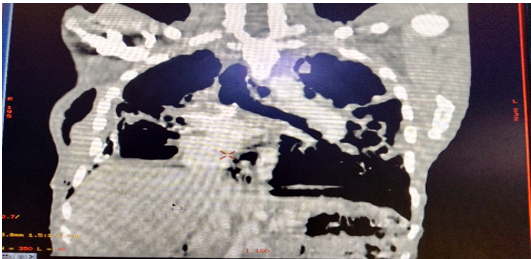
The CTA demonstrated a non-enhancing tubular structure/filling defect within the right pulmonary artery consistent with a thrombus. This measured about 51mm x 18mm in craniocaudal and mediolateral dimension. The thrombus is demonstrated to have caused dilatation and blockage of the right pulmonary artery. There is associated extensive destructive interstitial lung fibrosis bilaterally with air containing spaces consistent with the destroyed lung disease. Bilateral pleural thickening with turbid pleural effusion were also demonstrated bilaterally. A drainage tube was also noted within the right pleural space.
A diagnosis of right pulmonary artery thrombus in a patient with tuberculous destroyed lung syndrome was made. The patient is currently on combined multi-drug therapy for pulmonary tuberculosis (rifampicin, isoniazid, ethambutol and pyrazinamide) and anticoagulant therapy with heparin to achieve anticoagulation.
We present this case of pulmonary arterial thrombus coexisting with tuberculous destroyed lung syndrome due to its rare occurrence.
Pulmonary arterial thrombosis occurs in a setting of hypercoagulable states, intra-arterial tumorous conditions, and congenital heart disease accompanied by pulmonary hypertension [1].
Pulmonary tuberculosis (PTB) is a disease caused by Mycobacterium tuberculosis following inhalation of droplet nuclei laden with bacilli, his can either be pulmonary or extrapulmonary depending on the virulence of the organism or host defense mechanisms [2].
Venous thromboembolism (VTE) mainly comprises of deep vein thrombosis (DVT) and pulmonary thromboembolism (PTE), this can be classified further into provoked or unprovoked based on the presence or absence of a disease or condition that leads to VTE [3,5].
Pulmonary thromboembolism is the third most common cardiovascular disease after myocardial infarction and ischemic stroke, it is also the third leading cause of death related to cardiovascular diseases [6,7].
Pulmonary thromboembolism may be formed most times in the deep veins of the lower limbs, pelvis and right heart, or formed primarily within the pulmonary arteries. PTE arising from the deep veins are subsequently carried via systemic circulation to pulmonary vessels, causing sudden or recurrent blockage of the pulmonary arteries [3,6].
PTB is a chronic infectious disease and induces a systemic hypercoagulable state, and associated with PTE, those with active TB have an estimated prevalence of about 2.07% of developing venous thromboembolism [8,10].
In TB patients, three major factors are implicated in the formation of thrombosis, these are local lesion invasion, venous compression and hypercoagulability. The mycobacterium causes release of chemoattractant leading to vascular damage, the associated lymph nodes cause venous compression and increased serum fibrinogen level causes the hypercoagulable state [8,11,13].
Pulmonary TB, in active form of the disease, affects the pulmonary arteries and veins, this demonstrates vasculitis and thrombosis, other features may be hypertrophied bronchial arteries, Rasmussen aneurysm (5% of autopsy cases), pseudoaneurysms and vascular rupture [2,14,15].
Imaging plays a role in the diagnosis of PTE; these are mainly computed tomography angiography (CTA) and magnetic resonance angiography (MRA). CTA however is regarded the examination of choice in detecting PTE [1,15].
This is a forty-year-old man been managed for pulmonary TB, presented from a peripheral health facility and came for a chest computed tomography angiography (CTA) on account of suspected pulmonary thromboembolism (PTE).
The patient presented with chronic cough, fever, and poor appetite, weight loss and night sweats for more than one year.
On examination, the patient had a drainage tube in the right chest wall, difficulty in breathing, pale, appeared wasted, had mild fever, icteric, and appeared dehydrated. The pulse rate was 90 beats/min, blood pressure was 120/70mmHg. The patient had a positive Acid-fast bacillus staining for sputum. He is negative for the human immunodeficiency virus (HIV)infection.
The CTA demonstrated bilateral extensive streaky and patchy opacities with loss of lung volume and pleural effusion on the scout film (see figure 1). The serial images demonstrated a non-enhancing tubular structure/filling defect within the right pulmonary artery consistent with a thrombus. This measured about 51mm x 18mm in craniocaudal and mediolateral dimension. The thrombus is demonstrated to have caused dilatation and blockage of the right pulmonary artery. (see figures 2-4). There is associated extensive destructive interstitial lung fibrosis bilaterally with air containing spaces consistent with the destroyed lung disease (figures 2-4). Bilateral pleural thickening with turbid pleural effusion were also demonstrated bilaterally (figures 2 and 3). A drainage tube was also noted within the right pleural space (Figure 1).
A diagnosis of a large thrombus within the right pulmonary artery in a patient with bilateral destroyed tuberculous lungs was made.
The patient had commenced the combination therapy for tuberculosis: rifampicin, isoniazid, pyrazinamide and ethambutol. The patient also commenced anticoagulation with low-molecular-weight heparin for adequate anticoagulation.
We present this case of pulmonary arterial thrombus coexisting with tuberculous destroyed syndrome due to its rare occurrence.
Pulmonary arterial thrombosis occurs in a setting of hypercoagulable states, intra-arterial tumorous conditions, and congenital heart disease accompanied by pulmonary hypertension [1]. The case under review is a confirmed case of PTB, this is also a hypercoagulable state conforming to this literature.
Pulmonary thromboembolism is more prevalent in the male gender with about 3.2-fold increased risk of occurrence in the male than the female gender [16,17]. The index case happens to be a male, thereby conforming to these literatures.
Pulmonary tuberculosis (PTB) is a disease caused by Mycobacterium tuberculosis following inhalation of droplet nuclei laden with bacilli, his can either be pulmonary or extrapulmonary depending on the virulence of the organism or host defense mechanisms [2]. The case under review also tested positive for the Mycobacterium tuberculosis, and presented with features of pulmonary tuberculosis, thereby conforming to this literature.
Pulmonary thromboembolism may be formed most times in the deep veins of the lower limbs, pelvis and right heart, or formed primarily within the pulmonary arteries [3,6]. The index case is most likely formed primarily within the right pulmonary artery, and causing insidious symptoms of blockage of the pulmonary artery, thereby conforming to these literatures.
Three major factors are implicated in the formation of thrombosis, in patients with PTB, these are local lesion invasion, venous compression and hypercoagulability. The mycobacterium causes release of chemoattractant leading to vascular damage, the associated lymph nodes cause venous compression and increased serum fibrinogen level causes the hypercoagulable state [8,11,13]. The index case is a confirmed case of PTB with mycobacterium infection, similar factors are also likely to have caused the thrombus within the right pulmonary artery, thereby conforming to these literatures.
In TB infection, there is a tendency of causing enlargement of lymph nodes that may result in compression of pulmonary veins, this in combination of bed rest often leads to stagnation of blood as a predisposing factor to formation of PTE [16,18]. Enlarged lymph nodes were also demonstrated within the mediastinum of the index case which might also be responsible for the thrombus within the right pulmonary artery, thereby conforming to these literatures.
Patients with PTE most frequently present with dyspnea, chest pain, cough, but occasionally present with fever, tachycardia, abnormal pulmonary signs, peripheral vascular collapse, occasional cyanosis, hemoptysis and syncopal attacks [1-18]. The current case also presented with most of these clinical features, thereby conforming to these documented literatures.
Imaging plays a role in the diagnosis of PTE; these are mainly computed tomography angiography (CTA) and magnetic resonance angiography (MRA). CTA however is regarded the examination of choice in detecting PTE [1-15]. The index case had CTA, this confirmed the thrombus within the right pulmonary artery and features of destroyed lungs bilaterally, thereby agreeing with these literatures.
The diagnostic criteria of PTE following CTA are either, 1; arterial occlusion with failure to enhance the entire lumen due to a large filling defect within the artery, 2;partial filling defect surrounded by contrast material producing the polo mint signs on images perpendicular to the long axis of the vessel, and, 3; a peripheral intraluminal filling defect that forms an acute angle with the arterial wall [19,21]. The case under review had a large filling defect within the right pulmonary artery measuring about 51mm x 18mm in craniocaudal and mediolateral dimensions, and seen causing dilatation and occlusion of the artery. These features are in conformity to that reported in these literatures.
In patients with PTE with tuberculous destroyed lung, the treatment is aimed at treating the tuberculosis with multi-drug treatment which include: rifampicin, isoniazid, ethambutol and pyrazinamide. The thrombus is however treated by anticoagulation, most often by using anticoagulant agent heparin [2,5,8]. The index case was not an exception, he also had the combination therapy for PTB and low molecular weight heparin to achieve anticoagulation, thereby conforming to these literatures.
PTE should be suspected in patients with imaging features of tuberculous destroyed lung syndrome, CTA should be done promptly to exclude PTA, in order to reduce the morbidity and mortality associated with PTE especially in this group patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
