
case report | DOI: https://doi.org/10.31579/2690-4861/591
1Post-Doctoral Fellow, Department of Cardiology NH-RTIICS, Kolkata.
2Physician, NH-RTIICS, Kolkata.
3Physician, KPC Medical College, Kolkata.
4Senior Consultant Interventional Cardiologist Academic Co-ordinator, Department of Cardiology NH-RTIICS, Kolkata.
*Corresponding Author: Debabrata Roy, Senior Consultant Interventional Cardiologist Academic Co-ordinator, Department of Cardiology NH-RTIICS, Kolkata.
Citation: Debabrata Biswas, Nibedita Chakraborty, Arnav Roy, Anwesha Roy, Debabrata Roy, (2024), Reverse Takotsubo Cardiomyopathy mimicking inferior wall STEMI– A case report, International Journal of Clinical Case Reports and Reviews, 20(4); DOI:10.31579/2690-4861/591
Copyright: © 2024, Debabrata Roy. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 October 2024 | Accepted: 22 November 2024 | Published: 10 December 2024
Keywords: takotsubo syndrome; reverse takotsubo cardiomyopathy; stresscardiomyopathy; stemi; cardiogenic shock
Takotsubo syndrome is a disease of uncertain aetiology characterized by transientregional wall motion abnormality without associated coronary artery disease. Though the classical variant or the apical ballooning syndrome is most commonly seen in post-menopausal women atypical variants like reverse Takotsubo cardiomyopathy can occur in younger patients. Reverse Takotsubo cardiomyopathy more frequently presents with ST-segment depression and presentation as STEMI is rare. Here we are presenting a case of a39-year-old lady who presented as STEMI inferior wall but eventually diagnosed to have reverse Takotsubo cardiomyopathy based on clinical, echocardiographic and angiographic findings.
Takotsubo cardiomyopathy (TTC), also known as “stress cardiomyopathy” or “broken heart syndrome,” is an uncommon form of cardiomyopathy characterized by reversible regional wall motion abnormality of the left ventricle(LV) without obstructive coronary arteries.1,2Usually there is apical or less frequently midventricular ballooning of the LV.3Reverse Takotsubo cardiomyopathy(rTTC) is a rare variant of Takotsubosyndrome which has distinct features in terms of patient profile and clinical presentation compared to the classic apical ballooning syndrome.It is characterized by basal hypokinesis and apical hyperkinesias usually following an emotionalor physical stress.[4] Here we report a case of 39 years old lady who was diagnosed as reverse takotsubo cardiomyopathy based on clinical, echocardiographic and angiographic features.
A 39 years old lady presented with a history of fever, diarrhea, nausea, and vomitingfor which she was admitted to a local hospital where she developed retrosternal chest pain with a severity of 8/10 on visualanalog scale, not related to exertion. ECG was suggestive of STEMI inferior wall. She was treated in the line of acute coronary syndrome with dual antiplatelets, atorvastatin, and intravenous heparin. The fever subsided but she developed shortness of breathwhich rapidly progressed from NYHA class I to class IV over the next 2 days. She also developedhypotension for which she was put on intravenous noradrenaline infusion.
She arrived at our hospital 4 days after the onset of chest pain. At arrival, her BP was 84/56 mm Hg despite noradrenaline infusion, and herpulse was 124/min. She was severely dyspneic with bilateral basal crackles. Chest x-ray was suggestive ofpulmonary edema. ABG was suggestive of type 1 respiratory failure. She was intubated and put on mechanical ventilation. She was put on dopamine infusion.Initial blood investigation showed raised TLCand CRP. Trop I was 555 ng/L, NT-pro-BNP was 8070 pg/ml.Broad-spectrum antibiotics (meropenem and doxycycline) were started. D-dimer was elevated and thedirect Coombs test was negative. USG Doppler both lower limbs showed no deep vein thrombosis.
Subsequent ECG done after 2 days showed ST resolution compared to the previous one. Transthoracic echocardiography revealed akinetic basal inferior, posterior wall and basal septum, with preserved systolic function of the other walls andLeft ventricular ejection fraction (LVEF) of 40% with normal diastolic flow pattern.
Blood and urine culturesshowed no growth. She improved gradually over the next 4 days with supportive treatment. After extubation and discontinuation of inotropic support, she was taken up for invasive coronary angiography which revealed non-obstructive coronary arteries.
Repeat transthoracic echocardiography showed complete resolution of regional wall motion abnormalities with normal LV systolic function and ejection fraction of 60%. A diagnosis of reverse takotsubo cardiomyopathy was made as per the Mayo Clinic criteria.
Takotsubo is a Japanese word meaning “octopus pot” which is a vase-like contraption used to fish for octopus1. The syndrome was named so by Sato et alin 1990[2], because of the peculiar “octopus pot” like appearance of the left ventricle on the ventriculogram. It is estimated that around 2% of all troponin-positive patients presenting with suspected ACS have Takotsubo syndrome [3]. Takotsubo cardiomyopathy refers to an acute but often reversible left ventricular dysfunction with clinical presentation resembling acute coronary syndrome and characteristic anteroseptal-apicaldyskineticballooning of the left ventricle with hyperkineticbasal segments in the absence of obstructive coronary artery disease on angiogram.[3]
TTC has been classified into 4 subtypesbased on the regions of the ventricular wall motion abnormality: (1) classic type, (2) reverse type, (3) mid-ventricular type, (4) and localized type [4]. The reported incidence of rTTC varies from 1% to 23% in the existing literature [5]. According to the International Takotsubo Registry, only 2.2% of patients with Takotsubo syndrome had the reversed variant [6].
90% of the patients with Takotsubo cardiomyopathy are elderly women, with an average age of 58–75 years6. However, the reverse TTC variant is more commonly seen in younger women. In a study by Ramaraj et al. the mean age was 36 years for reverse type versus 62 years for the classic variety of TTC [7].
Although the precise pathogenic mechanism forTakotsubo cardiomyopathy is not known, catecholamine cardiotoxicityis the mostpopular theory [8]. It has been suggested that perimenopausal women have a higher concentration of B2 adrenergic receptors at the apex of the left ventricle, whereas young women have B2 receptors more concentrated at the base. This might explain the difference in the age distribution between the classic and the reverse variety of TTC [8].
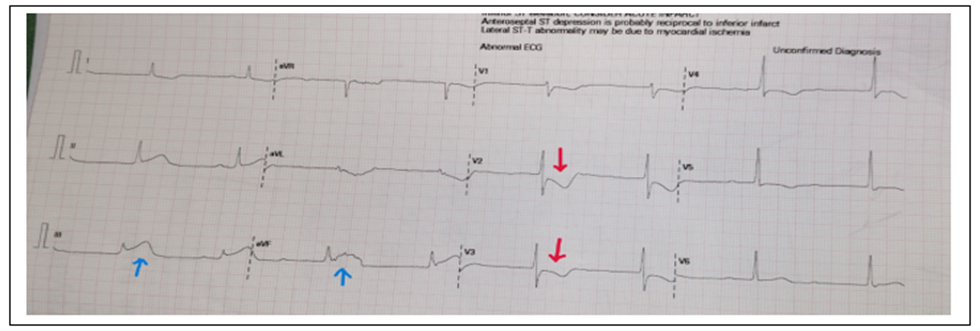
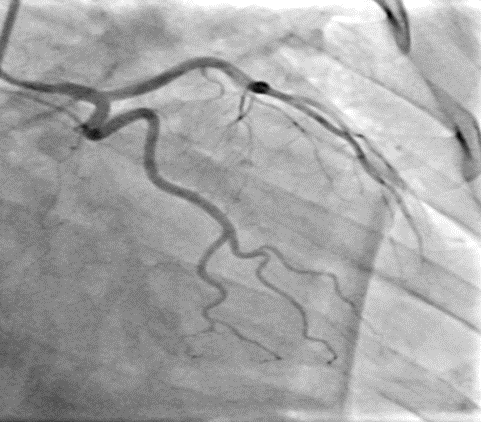
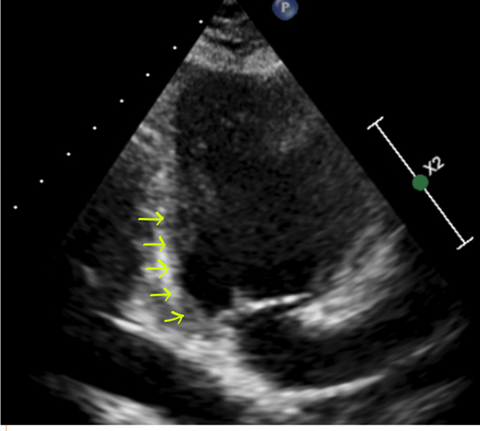
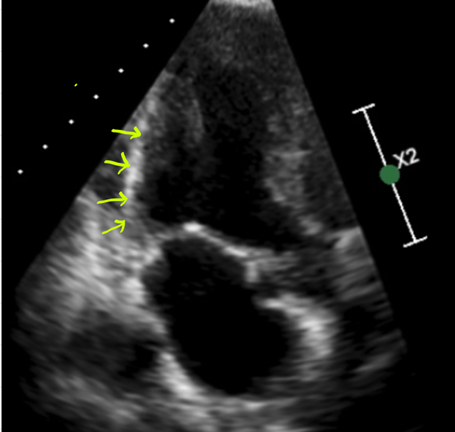
Figure 1: upper panel: ECG showing inferior wall STEMI (blue arrow: ST elevation; red arrow: ST depression); middle panel: coronary angiogram showing non-obstructive coronary arteries; lower panel: Echocardiography at presentation showing basal akinesia(left) and normal systolic function at recovery(right). (yellow arrows: basal akinesia)
Clinical features of rTTC include angina-likechest pain and/or dyspnea preceded by an emotional or physically stressful event. In our case, the physical stress was acute gastroenteritis. Acute complications like cardiogenic shock, cardiac arrest, and congestiveheart failure can occur in 15-20
Reverse Takotsubo cardiomyopathy is a rare variant of the Takotsubo syndrome. The reverse variety ismore common in younger women. Unlike the classical variety which may present with ST elevation in ECG, ST depression is the predominant ECG abnormality in the reverse variety. Moreover, the presentation of Takotsubo syndrome as a mimicker of STEMI usually involves theanterior wall. Here we have presented a rare presentation of reverse Takotsubo cardiomyopathy as STEMI of inferior wall. Patient had complete recovery with supportive management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
