
Case Report | DOI: https://doi.org/10.31579/2690-1919/424
Department of Urology, Hefei BOE Hospital, Hefei, China.
*Corresponding Author: Shaoyang Zhan, Department of Urology, Hefei BOE Hospital, Hefei, China.
Citation: Lufeng Zhang, Shaoyang Zhan, (2025), Retroperitoneal Fibrosis Caused by Cysticercosis, J Clinical Research and Reports, 18(2); DOI:10.31579/2690-1919/424
Copyright: © 2025, Shaoyang Zhan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2024 | Accepted: 03 January 2025 | Published: 24 January 2025
Keywords: retroperitoneal fibrosis; cysticercosis; bilateral ureters
Cysticercosis refers to a disease caused by the larvae of Taenia solium parasitizing various tissues and organs of the human body. It is reported that cysticercosis is most commonly caused by the central nervous system, and retroperitoneal fibrosis is rare. We report a case of retroperitoneal fibrosis caused by cysticercosis and a urinary tract obstruction caused by retroperitoneal fibrosis, which was successfully relieved by transurethral stenting. The complex pathophysiological mechanism of cysticercosis-induced retroperitoneal fibrosis requires further study. In the diagnosis and treatment of the disease, it is very important to consider the patient's epidemiological history and the presence of parasite infection.
Retroperitoneal fibrosis (RPF) is a rare disease whose histological features are inflammatory-fibrous tissue surrounding the abdominal aorta, iliac arteries, and even extending to the retroperitoneum and surrounding adjacent tissues such as ureter and inferior vena cava, resulting in a series of compression symptoms [1]. RPF is divided into primary (also called idiopathic) and secondary types according to the cause. The etiology of primary RPF is unknown, but some studies suggest that it is the result of autoimmune inflammation. Secondary RPF has a clear etiology, mostly secondary to tumors, drugs, radiation therapy, etc [2]. Among them, lymphoma, retroperitoneal sarcoma, carcinoid, and primary tumor metastasis are malignant causes of secondary RPF [3]. However, RPF caused by cysticercosis is rare and has not been reported at home and abroad. A case in our hospital:
The patient, male, 69 years old, BMI: 20.03 kg/m, was admitted to the hospital for more than three months due to low back pain and discomfort. Before admission, magnetic resonance urography (MRU) showed that both kidneys and the middle and upper ureters were dilated with hydrops, and retroperitoneal fibrosis was possible. Renal function test showed: creatinine: 356 umol/L, urea: 20.97 mmol/L. After admission, plain and enhanced abdominal and pelvic scans showed: [1] abnormal density around the abdominal aorta and bilateral ureters, considering the possibility of idiopathic retroperitoneal fibrosis (Figure 1A), please combine clinical; [2] change of chronic pancreatitis; [3] abnormal enhancement of pancreas and left kidney parenchyma, consider abnormal perfusion, follow-up; [4] local abnormal density in venous phase of left internal lobe of liver, consider local poor perfusion; [5] right kidney atrophy; bilateral renal pelvis and bilateral The upper segment of the ureter was dilated with hydrops; [6] pleural effusions and ascites were present on both sides; [7] there were multiple short-strip high-density shadows in the subcutaneous and abdominal pelvic cavity of the chest, abdomen, and pelvis, and calcification of cysticercosis was considered (Figure 1B); [8] prostate calcification; [9] the right renal artery was slender, and calcified plaques formed at the origin of bilateral renal arteries and abdominal aorta. Renal function test showed: creatinine: 376.0 mmol/L, urea: 23.4 mmol/L, K+: 6.0 mmol/L. Ureteroscopy and bilateral ureteral stent placement were performed. Postoperative re-examination of kidney ureter bladder (KUB) showed the presence of bilateral ureteral stents (Figure 2). The patient's creatinine was 331.2 mmol/L, creatinine was 25.1 mmol/L, and K+ was 4.0 mmol/L 3 days after surgery. The patient was followed up after discharge for 2 years, during which the double J tube was replaced every six months. The creatinine was close to 170 mmol/L, urea was close to 12.9 mmol/L, and K+ was normal.
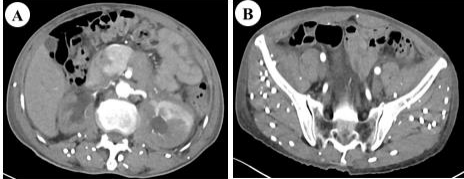
Figure 1: Abdominal and pelvic plain scan + enhancement (A); abnormal density around the abdominal aorta and bilateral ureters may be considered as idiopathic retroperitoneal fibrosis (B); there are multiple short-stripe high-density shadows in the thoracoabdominal subcutaneous and abdominal pelvic cavity, and cysticercosis calcification is considered.
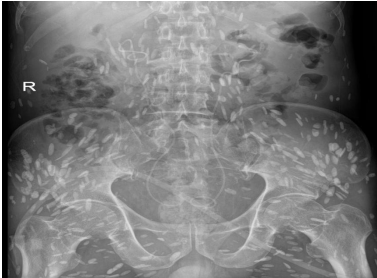
Figure 2: kidney ureter bladder (KUB), after ureteral stent placement.
Cysticercosis is a disease caused by taenia solium larva parasitism in various tissues and organs of the human body. Taenia solium adult parasite in the human intestine, eggs with human excrement out of the body, when the eggs are swallowed by the intermediate host (pig), can develop into cysticercus in the pig, when people eat raw pork containing cysticercus can cause tapeworm disease, also can cause cysticercus disease, also known as cysticercosis [4]. In 2010 and 2014, it was listed as one of the neglected tropical diseases and negligible zoonotic diseases by the World Health Organization (WHO) and the Food and Agriculture Organization of the United Nations (FAO), respectively [5]. Cysticercosis is spreading around the world and is a major health problem in most countries in Latin America, Africa and Asia. With globalization and increased exchanges between countries, more and more cases of cysticercosis are reported in non-endemic areas, and some developed countries have classified cysticercosis as an emerging infectious disease [4]. In China, the disease is mainly prevalent in the southwest region, especially in Yunnan Province, where a considerable number of residents have the habit of eating raw or undercooked pork. Cysticercosis can affect any tissue in the body, such as the central nervous system, subcutaneous tissue, eyes, and muscles [6]. The central nervous system is most common in clinical cases [7,8].
Systemic disseminated cysticercosis is clinically rare, and the mechanism of retroperitoneal fibrosis in this patient is unclear. Parasites can produce a series of physical and chemical stimulation and inflammatory reactions in human body, such as mechanical stimulation and immune pathological damage caused by insect movement, and toxic reactions caused by insect secretions, excreta and corpses. In this case, it was considered that the formation of fibrous tissue caused by physical and chemical stimulation and inflammation caused by parasites might encase adjacent tissues, press the ureter and lead to ureteral obstruction, resulting in renal failure. Therefore, after the double J tube was indwelled, the creatinine and potassium decreased significantly and stabilized at a slightly higher normal value. Therefore, we recommend long-term indwelling of the double J tube to keep the ureter open.
In conclusion, systemic disseminated cysticercosis caused by taenia solium infection is relatively rare in clinical practice, and the disease itself and the impact on the host are more complicated, which makes the diagnosis and treatment of clinical diseases more difficult. In clinical practice, the cause of parasites is often overlooked. In the diagnosis and treatment, the uncommon cause of parasites should be considered to avoid misdiagnosis and missed diagnosis, which will affect the diagnosis and treatment plan and prognosis of patients.
RPF: Retroperitoneal fibrosis
KUB: Kidney ureter bladder
MRU: Magnetic resonance urography
WHO: World Health Organization
FAO: Food and Agriculture Organization of the United Nations
We thank our patient for her consent in allowing us to share his experience.
All data generated or analysed during this study are included in this published article.
Informed written consent was obtained from the patient for publication of this manuscript, including images or other personal or clinical details of the patient.
The authors declare that they have no conflicts of interest.
LZ conceived and designed the report and collected and organized the data. SZ wrote the initial and final draft of the article and provided logistic support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
