
Research Article | DOI: https://doi.org/10.31579/2578-8965/132
1 Department of Obstetrics and Gynecology, University Clinical Hospital of Valladolid, Management Regional Health of Castilla y León (SACYL), Spain.
2 Department of Pediatrics and Immunology, Obstetrics and Gynecology, Nutrition and Bromatology, Psychiatry and History of Science, Faculty of Medicine, University of Valladolid, Spain.
3 Obstetrics and Gynecology Service, Hospital Universitario Doctor José Molina Orosa de Lanzarote, Canary Health Service (SCS), Spain.
4 Obstetrics and Gynecology Service, Regional Hospital of Valdeorras, Galician Service of Health (SERGAS), Spain.
*Corresponding Author: María Cuaresma-González, Department of Obstetrics and Gynecology, University Clinical Hospital of Valladolid, Management Regional Health of Castilla y León (SACYL), Spain.
Citation: María C. González, Sonia D. M. Manso, Elena G. García, Marta I. Nieto, Julio G. Tejedor et al. (2022) Results of Treatment of Female Stress Urinary Incontinence Treated with Transobturator Suburethral Banding: 9-Years Follow-Up. An Observational Prospective, Single-Center Study. J.Obstetrics Gynecology and Reproductive Sciences 6(5); DOI: 10.31579/2578-8965/132
Copyright: © 2022, María Cuaresma-González, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 August 2022 | Accepted: 05 September 2022 | Published: 19 September 2022
Keywords: stress urinary incontinence; suburethral bands; transobturator; continence rate and complications.
Background: tension-free suburethral bands represent the "gold standard" for the surgical treatment of stress urinary incontinence (SUI). Specifically, the transobturator approach is the most widely used because of its high cure rates in the medium term, and its good safety profile. These data support the use of suburethral bands and, since the beginning of this century, they have displaced retropubic colposuspension.
Objective: Study the long-term efficacy and safety (9 years) of transobturator suburethral band surgery (TOT) in the treatment of SUI.
Material and methods: An observational descriptive study with N=133 patients operated with TOT between 2012 and 2021 at the Valladolid University Clinical Hospital (Spain), who had completed at least one year of postoperative follow-up.
Variables analyzed: total continence and objective healing rates, subjective healing rate and postoperative complications.
Statistics: Statistics: Student t-test or U-Mann-Whitney for quantitative variables, Chi-Square for categorical variables.
Results: total continence rate from 1 to 9 years: 70.7%, 63.4%, 63.9%, 55.4%, 54.2%, 51.2%, 52.4%, 33.3%, and 100%. Objective cure rate from 1 to 9 years: 92.1%, 91.5%, 89.7%, 80%, 85.4%, 75.6%, 71.4%, 66.7%, and 100%. Subjective cure rate according to the median score on the ICIQ-IU-SF questionnaire from 1 to 9 years: 0, 1.5, 2, 4, 4, 6, 8, 12, and 0. Immediate complications were reported in 12.8% of cases, intermediate in 5.3%, and late in 30.1%. Of note was the occurrence of “de novo” urge urinary incontinence (UUI) in 8.3% and recurrence of SUI in 12%.
Conclusions: TOT surgery is one of the main therapeutic tools in the surgical treatment of SUI, with high efficacy and a good safety profile. However, more long-term studies are needed to consolidate the results obtained with this technique.
Stress urinary incontinence (SUI) is defined such as the involuntary loss of urine related to physical activity, coughing or any situation that increases intra-abdominal pressure [1]. It is a pathology with an increasing prevalence, ranging between 10 and 40% in women worldwide, which significantly affects their quality of life. This high prevalence represents also a significant social burden in economic terms [2]. Multiple risk factors are associated with SUI but, above all, age, parity and type of delivery, constipation or body mass index (BMI) [1].
SUI is usually due to a mechanical or anatomical defect, or weakness of the urethra or pelvic floor; this is why the therapeutic approach tends to focus on mechanical therapies [3]. Management depends on the severity of incontinence, the criteria of the doctor and the characteristics of the patient. In our country there are no drugs marketed for the treatment of SUI. The therapeutic possibilities are, therefore, conservative management and surgery. Lifestyle modifications, bladder reeducation and rehabilitation of the pelvic floor muscles are three important therapeutic pillars prior to surgical management [4]. The surgical treatment of SUI has evolved greatly in recent decades, thanks to the appearance in 1996 of surgery with a sling or retropubic mediourethral band, and later the transobutrator approach in 2001. Since 1999, mini-slings with bio-materials have been designed, and it was in 2006 that polypropylene mini-bands with specific insertion systems were developed [5]. Currently, tension-free suburethral bands represent the "gold standard" for the surgical treatment of SUI. Specifically, the transobturator approach is the most widely used due to its high objective and subjective cure rates in the medium term and its good safety profile, with fewer intraoperative and postoperative complications. These data support the use of suburethral bands and since the beginning of this century they have displaced retropubic colposuspension [6].
The aim of the study is to analyze the long-term (9 years) efficacy of transobturator suburethral banding (TOT) in the treatment of SUI, using objective and subjective cure rates. Other secondary objective is to examine the complications derived from the procedure at long-term follow-up.
An observational, prospective, single-center study was carried out for 9 years (2012-2021) at the Valladolid University Clinical Hospital (Spain), in women who had underwent TOT band surgery, and who had completed one year of postoperative follow-up.
Inclusion criteria: SUI due to urethral hypermobility, associated or not with mixed urinary incontinence (MUI) and failed or undesired conservative treatment.
Exclusion criteria: diagnosis of neurogenic bladder and postvoid residual >100ml.
Age and BMI did not limit inclusion in the study because both are important variables that could determine surgical outcomes.
At the initial visit, patients were evaluated clinically and ultrasonographically, using validated questionnaires such as ICIQ-IU-SF. Urodynamic study (EUD) was performed in complex or recurrent incontinence or in patients with previous incontinence surgery. In the first two years of follow-up, patients were evaluated in the Pelvic Floor Unit by exhaustive anamnesis, physical examination and ultrasound, assessing the efficacy of TOT and analyzing immediate (<7>
Statistical analysis: continuous quantitative variables with normal distribution were described by mean and standard deviation, and those with non-normal distribution by median and interquartile range (P25-P75). Qualitative variables are described by “n” and percentage. The Student t-test was used to study quantitative variables with a normal distribution, and the U-Mann-Whitney test was used otherwise. The Chi-square test with Yates correction was used to study categorical variables. In all cases, less than 0.05 was the value taken as statistically significant. SSPS v. 25 was the statistic software used.
Ethical approval: authorization of the study by the ethics and research committee of the Valladolid East health area (Code: FO-P07-12). Verbal informed consent was obtained from the patients included.
Demographic characteristics are shown in Table 1: average age was 66.5 (56.3-72) years. The average BMI was 27.5 ± 4.2 kg/m2. The 96.2% were multiparous, 9% had had an instrumented delivery with forceps, and 21.1% had fetal macrosomia.
| VARIABLE | RESULT |
| Age | Median (P25-P75): 66.5 (56.3-72) |
| BMI | Average ± SD: 27.5 ± 4.2 |
| Physical activity | 30 (22.6%) |
| Parity | Primiparous: 5 (3.8%) |
| 1 delivery: 13 (9.8%) | |
| ≥2 delivery: 115 (86.4%) | |
| Instrumented delivery with forceps | 12 (9%) |
| Fetal macrosomia | 28 (21.2 %) |
| Respiratory disease | 8 (6%) |
| Psychiatric disease | 28 (21.1%) |
| Neurological disease | 5 (4%) |
| Smoke | 11 (8.3%) |
Gynecological surgery | Abdominal hysterectomy 15 (11.3%) |
| Laparoscopic hysterectomy 1 (0.8%) | |
| Vaginal hysterectomy 8 (6%) | |
| Anterior colporrhaphy 15 (11.3%) | |
| Posterior colporrhaphy 11 (8.3%) | |
| Anterior prolapse mesh 2 (1.5%) | |
| Posterior prolapse mesh 2 (1.5%) | |
| Mini-Sling 8 (6%) | |
| Burch 1 (0.8%) | |
| Marshall-Marchetti 3 (2.3%) | |
| TOT 7 (5.3%) |
Table 1: Demographic characteristics:
Regarding the type of urinary incontinence: 36.8% presented SUI, 54% MUI and 9% occult urinary incontinence; in 75.2% the SUI was grade II and in 20.3% grade III. DUS was performed in 10.5% of the patients. The average initial ICIQ-IU-SF was 15 (14-17) points.
The approach and type of suburethral band are described in Table 2; the In-Out technique with I-Stop® band was the most frequently used. The median surgery time was 65 (45-90) minutes.
IN-OUT TECHNIQUE 100 (75.2%) | I-Stop® (CL Medical) 61 (45.9%) |
| In Gyne S® (Dipromed) 17 (12.8%) | |
| Gynecare TVT obturador® (Ethicon-Johnson) 13 (9.8%) | |
| TOA® (Presurgy) 9 (6.7%) | |
OUT-IN TECHNIQUE 33 (24.8%) | In Gine S® (Dipromed) 1 (0.8%) |
| Monarc® 32 (24%) |
Table 2: approach and type of suburethral band.
Immediate complications were reported in 12.8% of cases, intermediate in 5.3% and late in 30.1% (Table 3). Of note was the occurrence of “de novo” urinary incontinence (UUI) in 8.3% and recurrence of SUI in 12%.
Inmediate (<7> Bladder injury Fever Urinary tract infection Urinary retention Urinary catheter Pain Reoperation for bleeding Vaginal perforation | 17 (12.8%) 1 (0.8%) 1 (0.8%) 2 (1.5%) 11 (8.3%) 4 (3%) 1 (0.8%) 1 (0.8%) 2 (1.5%) |
Intermediate (≥ 7 days- < 30> Fever Bleeding Urinary tract infection Urinary retention Urinary catheter Pain | 7 (5.3%) 1 (0.8%) 1 (0.8%) 3 (2.3%) 2 (1.5%) 1 (0.8%) 1 (0.8%) |
Late (≥ 30 days) “De novo” UUI Urinary retention Mesh extrusion Pain Recurrence of SUI Urethrolysis | 40 (30.1%) 11 (8.3%) 3 (2.3%) 3 (2.3%) 13 (9.8%) 16 (12%) 3 (2.3%) |
Table 3: postoperative complications:
The number of patients completing follow-up each year is detailed in Table 4, with only one patient having finished the complete follow-up at 9 years.
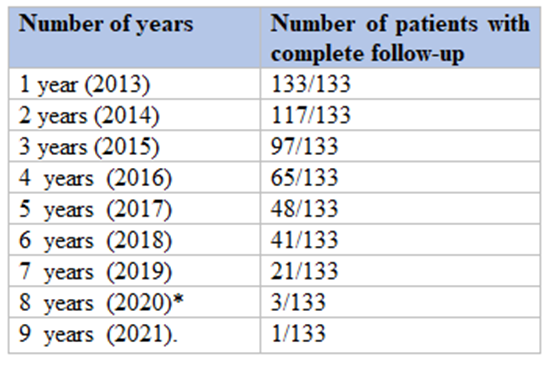
Table 4: patients follow-up. *Covid-19 pandemic.
The total continence rate at 12 months was 70.7%, and during follow-up: 63.4% (2 years), 63.9% (3 years), 55.4% (4 years), 54.2% (5 years), 51.2% (6 years), 52.4% (7 years), 33.3% (8 years) and 100% (9 years) (Figure 1).
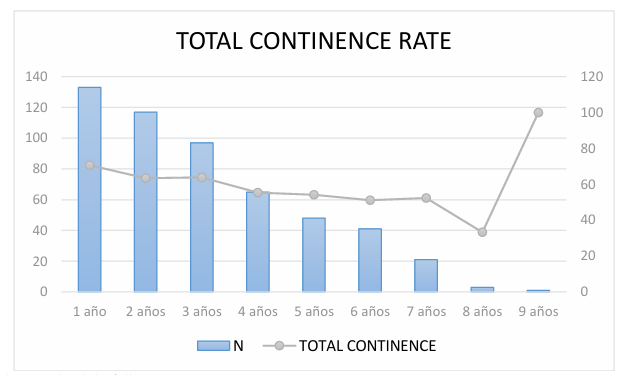
N=numer of patients who completed the follow-up.
Figure 1: Total continence rate.
The objective cure rate at 12 months was 92.1%, and subsequently 91.5% (2 years), 89.7% (3 years), 80% (4 years), 85.4% (5 years), 75.6% (6 years), 71.4% (7 years), 66.7% (8 years), 100% (9 years) (Figure 2).
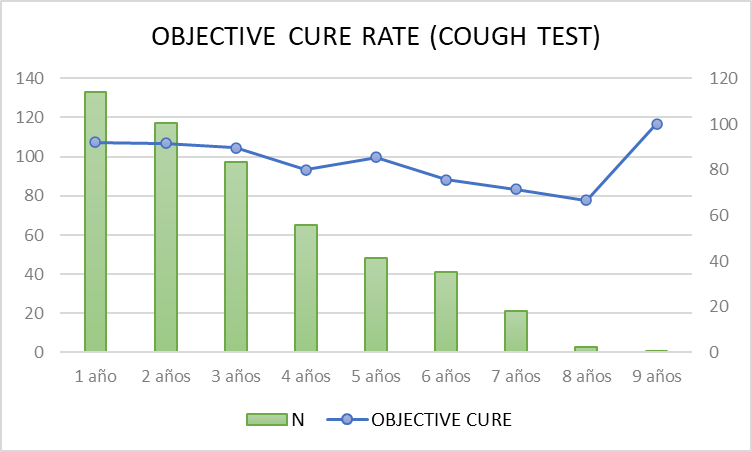
N=numer of patients who completed the follow-up.
Figure 2: Objective cure rate.
Regarding subjective cure according to the degree of satisfaction: at 12 months 81.7% were considered very satisfied. At follow-up: 76.6% (2 years), 73.1% (3 years), 65.6% (4 years), 68.1% (5 years), 56.1% (6 years), 47.7% (7 years), 33.3% (8 years) and 100% (9 years). According to the PGI-1 scale: in the first year 83.5% of the patients gave scores of 1-2, reporting feeling much and much better, respectively, compared to before the surgery. Subsequently, these scores were maintained at 89.6% (2 years), 85.4% (3 years), 78.1% (4 years), 77.1% (5 years), 68.3% (6 years), 57% (7 years), 66.7% (8 years) and 100% (9 years). According to the ICIQ-IU-SF questionnaire, the median was 0 the first year, 1.5 (2 years), 2 (3 years), 4 (4 years), 4 (5 years), 6 (6 years), 8 (7 years), 12 (8 years) and, the only patient with complete follow-up of 9 years, expressed a score of 0. (Figure 3)
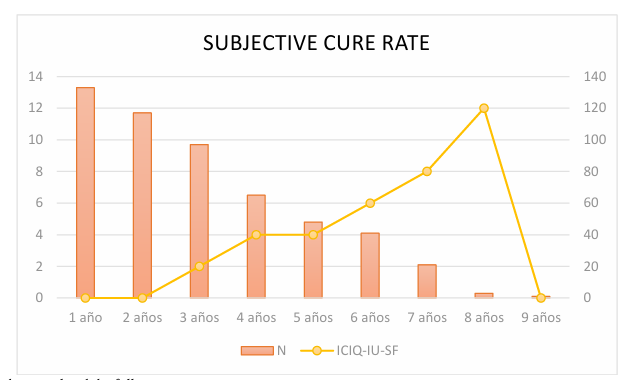
N=numer of patients who completed the follow-up.
Figure 3: Subjective cure rate using the ICIQ-IU-SF questionnaire.
In the last few years, many data about the efficacy of treatment of SUI with TOT have been published [6][7]. However, there are few publications [8][9][10] of long-term results, such as this study with nine years of follow-up. In the latest Cochrane review (2017) about the use of mediourethral bands, the authors conclude in the same sense, that longer-term studies are needed to clarify both the evidence and the uncertainty about the effectiveness and complications of TOT [11].
In the analysis of these patients, it is interesting to evaluate the objective cure rate. According to published data, patients who undergo TOT maintain high stress continence, especially during the first years [8][10][12][13][14][15][16]. It should be noted that in this study, after 7 years of follow-up, it remains above 70%, supporting the medium and long-term efficacy.
The degree of satisfaction remained above 80% during the first year, with PGI-1 scores of 1-2, similar to that reported by other authors [7][13][14][15] and with better results compared to another 4-year follow-up study [17]. The subjective cure rate decreases over time, partly due to the appearance of aging-related symptoms such as urgency. The subjective cure rate is also demonstrated by the ICIQ-IU-SF questionnaire by comparing how the initial median value is higher than that observed during follow-up and, although the score gets worse over the years [especially after the seventh year], it does not reach the initial median [16].
A meta-analysis by Fusco et al. [19] showed that bladder perforation, pelvic hematomas and urinary retention were less common after transobturator band [TOT] surgery. The obturator approach leads to limited intraoperative damage to the urinary bladder, but does not exempt from other intraoperative and postoperative complications.
In general, complications were classified as minor (Clavien-Dindo [18] Grade I and II), except two major complications Clavien-Dindo [18] Grade III]: a bladder injury and a perforation of the inferior epigastric artery in the space of Retzius.
The frequency of complications is higher in the long term [30.1%]. The most frequent complications, also observed in other studies [7][12][13][14][15][16] are urinary retention, pain and mesh extrusion. Only one case of bladder perforation occurred, which is consistent with other publications [4][19]. The rate of “de novo” UUI, the main reason for the worsening of patients, was 8.3%, a lower value than the obtained in other studies [6][7][13][15], although higher than that found in short-term follow-up studies [15][20]. Recurrence of SUI occurred in 12% of patients, a higher value than the published by Tulokas in 2020 (17-year follow-up) [9] or by Sharma in 2021 (3-year follow-up) [16], although lower than that described in most studies on the medium-term efficacy of TOT [6][7][14][21]. The main limitations of the study are the sample size, because it is not very large, and the fact than only one patient has completed the fully follow-up period.
TOT surgery is a great therapeutic alternative in the management of SUI after failure of conservative treatment, with high long-term efficacy, reflected in both objective and subjective cure, and a good safety profile, with few minor and more frequent late complications. Overall patient satisfaction and objective outcomes should be standardized and reappraised at each postoperative visit in order to be able to analyze the evolution throughout the follow-up. Finally, more long-term studies are needed to consolidate the results obtained and to allow comparison of inclusion and exclusion criteria, as well as evaluation of effectiveness.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
