
Case Report | DOI: https://doi.org/10.31579/2693-7247/202
Department of Surgery Roosevelt Hospital, Guatemala.
*Corresponding Author: René Daniel Villatoro Martínez, Department of Surgery Roosevelt Hospital, Guatemala.
Citation: René Daniel Villatoro Martínez, Jimmy Edmundo Guillén, (2024), Resection of pleomorphic parotid adenoma in children, J. Pharmaceutics and Pharmacology Research, 7(9); DOI:10.31579/2693-7247/202
Copyright: © 2024, René Daniel Villatoro Martínez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 June 2024 | Accepted: 27 June 2024 | Published: 22 August 2024
Keywords: pleomorphic adenoma; carotid; adolescent
Salivary gland tumors are rare and encompass a diverse group of histologies. Less than 5% of the affected population is paediatric. Pleomorphic adenoma, is the most common tumor of the salivary glands, consisting of epithelial and mesenchymal components. The main characteristic of this benign tumor is its slow growth, which causes the notorious presence of a mass or deformity at the facial or cervical level, its treatment is surgical and as in any procedure there are complications, the main one and the one that demands greater caution in treatment is post-surgical facial paralysis, together with possible vascular lesions of large vessels at the cervical level and even the possible injury of another nearby nerve structure. Due to the complexity of the surgical approach, it is important to take into account the anatomical structures in both the parotid region and its adjacent structures, the parapharyngeal space is one of the cervical fascial spaces in which inflammatory or neoplastic processes can be found, the latter occupying less than 1% of head and neck tumors. The space has an inverted pyramid shape that extends from the base of the skull specifically from the greater wing of the sphenoid to its vertex that is located in the greater horn of the hyoid, this anatomical region is divided into 2 compartments by the styloid process, in the first compartment called pre-styloid are located the internal maxillary artery and the inferior alveolar nerves, lingual and atriculotemporal, in the retro-styloid compartment are located the internal carotid artery, the internal jugular vein, the cranial nerves IX, X, XI and XII, the cervical sympathetic chain and multiple lymph nodes, all this anatomical delimitation is essential to determine the possible origin of the mass under study in addition to knowing the great risks and complications that may appear at the time of performing the surgical approach. We present the case of a 14-year-old boy with satisfactorily resected pleomorphic adenoma.
Salivary gland tumors are a rare and heterogeneous group of neoplasms, they are classified according to the World Health Organization (WHO) system of 2017 [1]. They correspond to 3% of all head and neck tumors, the most common being pleomorphic adenoma, which represents 80% of all benign masses of this gland. Also known as benign mixed tumor, it derives from a mixture of ductal and myoepithelial elements. The parotid gland is the most common of the salivary gland tumors, accounting for approximately 80-85% of these tumors. Histologically, it can present a great diversity between one tumour and another and even in different areas of the same tumour, which is why it owes its name pleomorphic or mixed adenoma. Pleomorphic adenoma is slow-growing, not attached to the skin, and usually ulcer-free [2]. Tumors that arise in the minor salivary glands are malignant, clinically, pleomorphic adenomas arise as asymptomatic masses of slow growth, with size ranging from a few millimeters to several centimeters, reaching considerable sizes in some cases; More symptoms such as foreign body sensation, otalgia, parotid mass, trismus are described. Facial pain and paralysis are uncommon, but they can occur in certain cases [2,3]. The anamnesis should ask about the existence of glandular swelling and its form of presentation, since it can be unilateral or bilateral; as well as symptoms of fever, the administration of medications and the presence of other diseases such as viral diseases. The age of onset of clinical manifestations will be taken into account, so parotid tumors in newborns and young children are hemangiomas or lymphangiomas and, in very exceptional cases, congenital cysts. In school-age age, viral infection predominates, and the presence or absence of asymmetries must be observed in the inspection. Parotid palpation compares the size and consistency of the two glands, and ends with bimanual or bidigital palpation by placing a hand inside the oral cavity. This last maneuver is essential for the exploration of the submaxillary and sublingual glands. Through the expression of the Stenon or Wharton's ducts, it is possible to observe the characteristics of the saliva produced by the different glands. If inflammatory disease is excluded, tenderness of the parotid is usually a sign of malignancy. The examination is completed with an inspection of the oral cavity [2,3].
A 14-year-old male patient. who consulted for increased volume in the right hemineck of 1 year of evolution. The patient did not have a personal or family history relevant to the current condition. Physical examination revealed an asymmetrical neck: with growth of the parotid region of the right Iado. A regular, firm, delimited and mobile mass was palpable. The function of the easy nerve was preserved. (Figure. 1A). Computed tomography (CT) at the parotid level showed no invasion of adjacent structures (Figure. 1B). X-rays of the anteroposterial neck and lateral neck showed no airway obstruction. An incisional biopsy was performed. which reported findings compatible with pleomorphic adenoma. With a diagnostic impression of a benign salivary gland tumor, the patient underwent surgery. The wound was extended to the right hemineck for lymphanode resection (Figure. 1C). Complete excision of the tumor was performed (Figure. 1D), respecting the integrity of the facial nerve. Neurostimulation was performed to rule out injury to the glossopharyngeal nerve. Patient with satisfactory evolution (Figure. 1E) The surgical specimen measured 7x4 cm, external surface intact. No lymph nodes were seen. The pathological diagnosis was pleomorphic adenoma of the parotid gland.
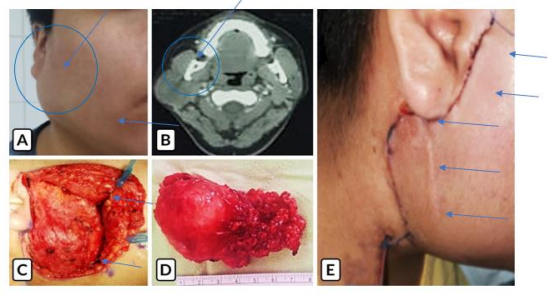
Figure 1: Pleomorphic adenoma. A) A well-defined mass within the right parotid region. B) ICT without invasion of adjacent structures. C) Initial dissection. D} Surgical piece. E) Closure of the surgical bed.
Parotid gland tumors are rare in pediatric patients. As in the adult population, benign tumors make up the majority of pediatric parotid gland tumors. Most studies consider pleomorphic adenoma to be the most common benign tumor of the parotid [4]. Pleomorphic adenoma of the parotid gland represents a therapeutic challenge in the pediatric population. Its benign histology advises preserving the facial nerve. However, its preference for recurrence and the risk of malignant degeneration in a population of patients with a long life expectancy requires aggressive treatment, always taking into consideration that nerve structures must be maintained and preserved to avoid the main complications of paralysis after surgery.
Pleomorphic adenomas should be treated diligently as they tend to relapse and malignant transformation. Rupture of the capsule and subsequent spillage of the tumor during excision are risk factors for recurrence [3]. Up to 10% of cases show malignant transformation and features that predict malignant change include advanced age, massive tumor size, long duration of the mass, appearance in the submandibular salivary gland, and hyalinized connective tissue [3].
According to the literature, the proper management of this pathology is purely surgical, performing parotidectomy in cases of salivary gland tumor is the only way to prevent the mass from causing lesions at the level of nearby structures, such as the facial nerve. Their correct dissection and identification are among the main issues within the procedure. Most salivary gland tumors are of epithelial origin, the parotid gland being the most affected. Fine needle aspiration biopsy is part of the diagnosis of this pathology, it has a specificity of 80 to 87% and a sensitivity of 73 to 97% [5]. Once the initial diagnosis has been made, the treatment of pleomorphic adenoma is purely surgical, in fact, it is considered the main pillar in the therapeutic management of this pathology. Superficial
parotidectomy with preservation of the facial nerve is the most commonly indicated procedure, and submandibular sialadenectomy or wide local excision for a minor salivary gland can be performed. The common point
of all these modalities is the need to perform a meticulous dissection of the capsule to avoid recurrence of the neoplasm [5].
Expanded facial nerve dissection and tumor tissue resection depend on size, location, and histopathology; It is a real challenge for the surgeon when the normal anatomy of the parotid is altered with the tumor. There are some constant anatomical points that will help identify it such as the cartilaginous pointer, the tympanomastoid suture in the stylomastoid foramen, the styloid process. Retrograde dissection is indicated in cases where, despite anatomical constants, the main trunk of the facial is not identified [6]. Tumor resection must involve the capsule where the mass is contained, because as mentioned above, recurrences are related to its presence, the incidence of recurrence is 2 to 5%. In the case of our patient, the resection included the total presence of the tumor capsule [6]. Maintaining the line in the diagnosis and evaluation of tumor masses allows an appropriate therapeutic decision to be made. The best way to have a clear diagnosis, according to the experience obtained and the literature studied, will be to obtain data from the medical history, physical examination, simple and contrasted tomography of the neck. Surgical resection is the recommended management for this pathology. The performance of parotidectomy in cases of salivary gland tumor is the only way to prevent the mass from causing lesions at the level of nearby structures, such as the facial nerve, its correct dissection and identification are among the main issues within the procedure. Histopathology will confirm the benign nature of the mass.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
