
Research Article | DOI: https://doi.org/10.31579/2639-4162/012
1 Department of Clinical Sciences, Copperbelt University, Michael Chilufya Sata School of Medicine, Public Health Unit, Ndola.
*Corresponding Author: David Mulenga, Department of Clinical Sciences, Copperbelt University, Michael Chilufya Sata School of Medicine, Public Health Unit, Ndola.
Citation: David Mulenga, Seter Siziya, Impact of Cooking Fuel Choices on Maternal Lung Functions in Selected Rural and Urban Areas of Copperbelt Province, Zambia, Doi: 10.31579/2639-4162/012
Copyright: © 2018. David Mulenga. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 June 2018 | Accepted: 21 June 2018 | Published: 02 July 2018
Keywords: Cooking fuel, Lung function, Biomass
Background: Considering the respiratory health risk of exposure to biomass cooking fuel emissions, this study was conducted to elucidate the relationship between cooking fuel choices and declined pulmonary function in rural and urban population in the Copperbelt Province of Zambia.
Methods: We carried out a cross-sectional study of 1,170 healthy nonsmoking pregnant women from Masaiti and Ndola predominantly using biomass fuel for cooking. Questionnaire based data was acquired along with standardized measures of lung function. MIR Spirobank G (Italy) was used in spirometry based on American Thoracic Standards.
Results: The present study found that over two thirds (69.2%) of pregnant women in the study population use biomass for cooking and only 12.4 % use electricity only. Declined lung function was found to be statistically significantly associated with cooking fuel choices (p – value 0.005) and a weak association was observed with gravida at a p-value of 0.056. Pregnant women using crop residues as cooking fuel were two times more likely to have a declined lung function [AOR 2.33 (1.27, 4.30)] compared with pregnant women using mixed fuel type (biomass and electricity) and those using electricity only were 57% less likely to have a declined lung function [AOD 0.43 (0.26, 0.69)].
Conclusion: Use of biomass for cooking among pregnant women is a strong determinant of declined lung function. Interventions to improve maternal respiratory health outcomes in Zambia and other countries in sub-Saharan Africa should involve making cleaner cooking fuel energy options available and accessible by ordinary women from both rural and urban areas.
In developing countries, use of fuels such as wood, dung and crop residue is estimated in as many as 70% of households [1,2] or in more than 3 billion people worldwide according to other researchers[3]. According to Chidumayo et al and Indaba Agricultural Policy Research Institute (IAPRI), charcoal is widely used in urban Zambia as a source of cooking fuel, either on its own or in combination with electricity, it’s further been observed that even among electrified households, charcoal is commonly used in combination with electricity, more than electricity only, an indication of pervasive fuel stacking, rather than fuel switching [4,5]. Health problems related to the use of solid fuels as an energy source have been an issue of concern especially in many poor countries. Biomass fuels are at the low end of the energy ladder in terms of combustion efficiency and cleanliness [6], they emit large quantities of smoke that contains many noxious components [7]. Periodic and longtime exposure to solid fuel emissions may lead to various types of adverse health outcomes such as chronic bronchitis, increase in the risk of tuberculosis, respiratory failure and cor pulmonale [8].
It is for this reason that biomass use for cooking and heating houses has been implicated in respiratory function disorders and pulmonary diseases due to emissions from incomplete combustion in usually poorly ventilated houses. The cheaper cooking fuel options in any context are generally less efficient cooking fuels, emit more smoke, and are the ones used by groups of people with the most poorly designed houses. Fuels such as propane, liquid petroleum gas (LPG), or ethanol usually burn very cleanly, but remain too expensive for many households. Electricity is the least polluting type of energy for domestic use provided households are geographically separated from power stations, but the problem is that it is not affordable to the average population.
According to Rehfuess, descending from the energy ladder to cheaper types of cooking fuel such as charcoal, wood and dung or crop residues, there are polluting fuels with both poor combustibility and highly toxic emissions. Simple muddy, thatched homes sometimes built with animal skins rarely have a chimney and, if present, the chimney is often a simple vent with no air-drawing flue [9]. Combustion of cheaper fuels in homes is responsible for indoor air pollution and indoor air pollution is in turn responsible for almost 2 million annual deaths and accounts for 2.7% of the global burden of disease [10]. Fuel types determine the amount of pollutants that would be emitted for instance, more pollutants are expected from fuels at the bottom of the energy ladder such as wood, cow dung and crop residue because they are unprocessed energy sources. The emissions have an adverse effect on the lung functions of the exposed individuals. Lower FEV1 and FVC values have been reported [11] among people predominantly using biomass compared with those using other fuel types. This observation is attributed to the effects of pollutants emitted by unprocessed cooking fuel types [12] on lung functions. Therefore, cooking fuel choices are an important predictor of reduced lung function among exposed populations and this has been demonstrated by many other researchers. In a study to evaluate the effects of solid fuels smoke exposure on pulmonary function, researchers observed a significant reduction in FVC, FEV1, FEV1 /FVC ratio and forced expiratory flow 25-75 in solid fuel users compared to individuals who used liquefied petroleum gas[13].
Biomass combustion causes high levels of health-damaging indoor air pollution including carbon monoxide, particulate matter, nitrogen dioxide and polycyclic aromatic hydrocarbons [14]. Since studies consistently show high indoor air pollution levels in households using biomass with PM2.5 being observed to be 10 to >50 times the WHO annual average Air Quality Guideline level [15], it therefore, follows that cooking fuel choices are a good proxy for noxious pollutants especially particulate matter (PM2.5). Many researchers have demonstrated that biomass combustion emits PM2.5 and many other pollutants. Some researchers in resource constrained countries do not directly measure exposure to household air pollution due to challenges in acquiring indoor air pollutant measurement devices. They use the effect estimates which are based on exposure determined by fuel type such as “use of solid fuels” or “exposure to biomass” compared with “use of other fuels” [12]. The proxy factors used to estimate level of exposure include involvement in cooking during pregnancy , use of charcoal or wood for cooking [16,17,18], and cooking in an enclosed kitchen with no window present [19].
To demonstrate the impact of solid fuel on the lung function, Desalu et al recruited women who predominantly used solid fuels for cooking in the study and findings indicated a reduction in pulmonary function [20]. It is important to note that reduction in pulmonary function due to the effect of solid fuel has not been documented consistently by all investigators. In a previous study to assess the impact of different cooking fuels on pulmonary function, Rinne et al. observed no difference in lung function among the different fuel types [11]. Another previous study by Reddy et al. also demonstrated that cooking with biomass was not significantly associated with lung function decline. However, this unexpected result was attributed to good ventilation in the kitchen where cooking was conducted. Inefficient ventilation of the kitchen is known to concentrate pollutants leading to adverse effects of biomass smoke on lung function [21]. We therefore, conducted this study in order to assess the impact of cooking fuel choices on maternal lung functions among Masaiti and Ndola residents in Zambia.
Methods and Materials
A cross sectional study among 1170 pregnant women in Masaiti and Ndola was conducted and a structured questionnaire was used to obtain information on background characteristics. Pulmonary function tests were performed at least three times for each pregnant woman in a sitting position with closed nostrils using MIR — Spirobank G (Italy) spirometer and with a different mouthpiece for each subject. The spirometer was calibrated to suit individual participant according to sex, age, height and weight. Demonstration about the test was done for the pregnant woman before the test. The tests were performed according to American Thoracic Society (ATS) standards. Spirometry values (FEV1, FVC and FEV1/FVC) were taken three times and the best result of the three measurements was recorded.
Data processing and analysis
Spirometry parameters of interest were FVC, FEV1 and FEV1/FVC. FVC and FEV1 < than 80% was regarded as a declined or poor lung function and similarly, FEV1/FVC ratio of < than 70% was also regarded as a reduced lung function. Preliminary analysis involving bivariate analysis was conducted in Epi Info and then the Multivariate Logistic Regression was carried out to determine the cooking fuel type that determines poor lung function. The magnitudes of association were estimated using odds ratios and their 95% confidence intervals. Statistical significance level was set at 5%.
Ethical Consideration:
The Tropical Disease Research Centre (TDRC) Ethics Committee approved the study and participants signed a consent form to participate in the study.
Results
Socio-economic and demographic characteristics of the pregnant women
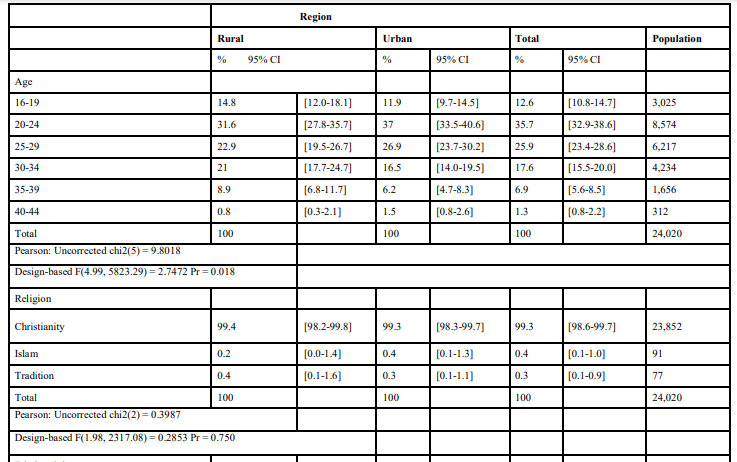
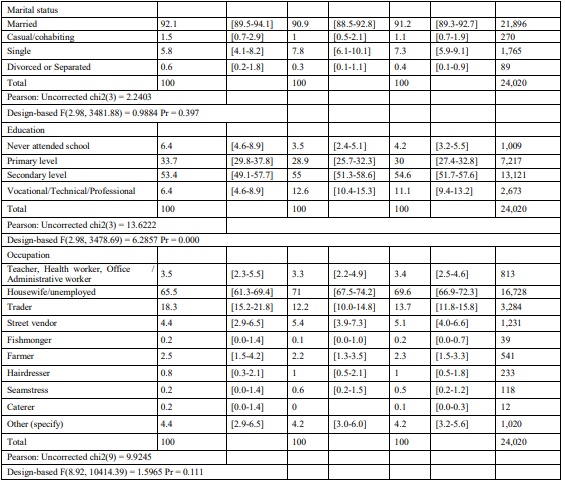
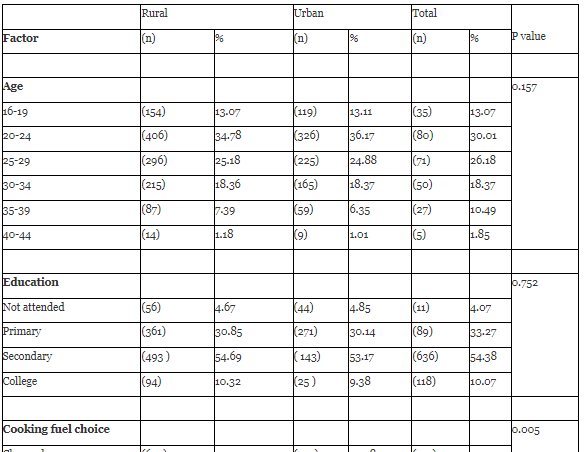
Out of a total of 1,170 pregnant women recruited to the study, more than half of them (58.9%) were from the urban area (Ndola City) and the rest (41.1%) from the rural area (Masaiti District). More than 80% of the study population were between the age of 35 and 16 years old with the highest proportion (35.7%) belonging to the age group 20-25 years old. Almost everyone (99.3%) practiced Christianity. Slightly over half of the participants when put together belonged to two provinces, namely northern (31.2%) and eastern (20.4%) provinces of Zambia. Majority (91.2%) of the participants were in a marriage relationship with more than half of the women (54.6%) having attained secondary and a third (30.0%) primary level of education. Over two thirds of the pregnant women (69.6%) were unemployed housewives and 13.7% were traders. Table 1 gives a summary of the demographic and socio-economic characteristics of the population.

Environmental and behavioral characteristics relating to exposure
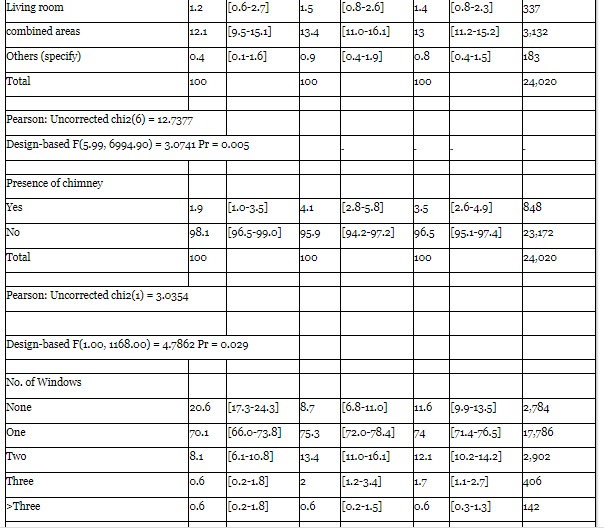
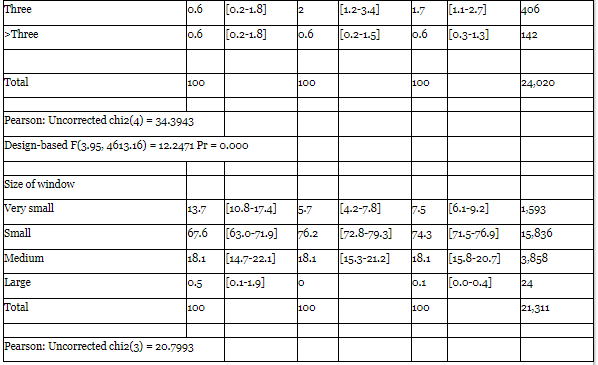
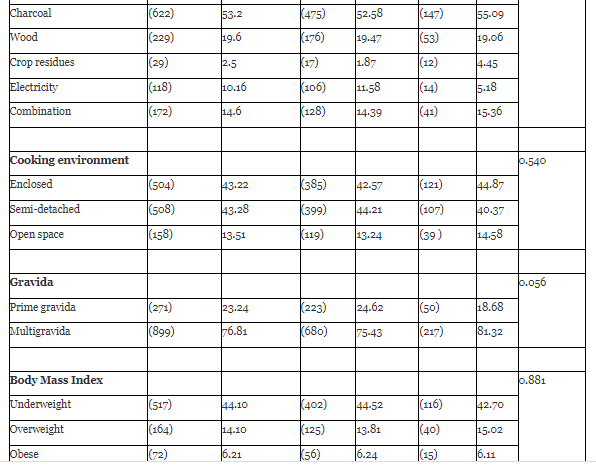
Almost all (94.5%) the pregnant women were involved in cooking duties during pregnancy and majority (82.5%) cooked on a daily basis compared to only 7.9% who cooked occasionally. Most of the pregnant women spent one to four hours on cooking. Out of those involved in cooking during pregnancy, less than a third (28.7%) spent the whole cooking period in the cooking area and close to three quarters (43.0%) stayed in the cooking area half of the cooking period. More than half (52.3%) of the participants reported using charcoal and less than a quarter (14.8%) reported using wood. With regard to kitchen type, more than one third (40.1%) pregnant women cooked in an enclosed kitchen, more than a quarter (16.9%) in a semi-enclosed shelter and slightly more than one fifth (20.3%) in an open space. Chimney was not common, only 3.5% reported presence of a chimney. Out of all those who cooked in an enclosed environment, 11.6% had no window while 74.0% and 12.1% reported having one and two windows respectively and out of those with windows, 74.3%, 18.1% and 7.3%, classified their windows as small, medium and very small respectively. Close to two thirds of the participants (61.6%) agreed that garbage burning was done at household level and 23.6 % reported always present when garbage burning is taking place, others 24.1%, 26.5% and 25.8% reported mostly present, occasionally present and never present at all respectively. Of those who burn garbage at home 39.8% reported occasional burning while 19.1% of them reported burning 2-3 days/week and 14.8% burn daily. Majority (79.6%) of the pregnant women reported that no one smoked at home and only 15.2% reported having one person smoking at home. Most of them (80.4%) reported not being exposed to second hand smoke at home. More than half of pregnant women (52.7%) reported spending 1- 4 hours outdoor and 28.9% reported spending 5-8 hours outdoor per day. More than a third (38.4%) women agreed to conducting their outdoor activities near an air pollution source and more than two quarters (62.4%) described the air pollution source as a busy road (traffic hot spot) while 19.3% of them described it as a combustion site and for the 14.5% it was a waste disposal site. Table 2 shows the summary of the exposure characteristics for both rural and urban areas.



Lung function test results of the pregnant women in the study population
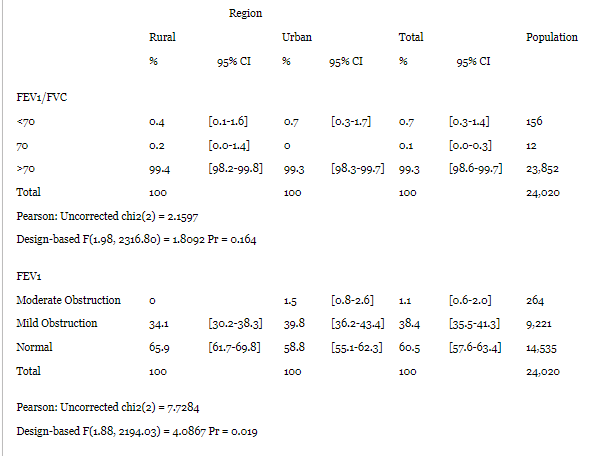
Table 3 presents the proportions of spirometry results of pregnant women in the study population. Almost all the pregnant women (99.3%) had an FEV1/FVC higher than 70% and close to two thirds (60.5%) of pregnant women had a normal FEV1 while more than one third (38.4%) recorded mild obstruction. Normal FVC was obtained in 35.6% of pregnant women while mild reduction and moderate reduction was recorded in 37.4% and 26.9% of pregnant women respectively.

Mean differences of lung functions between rural and urban area
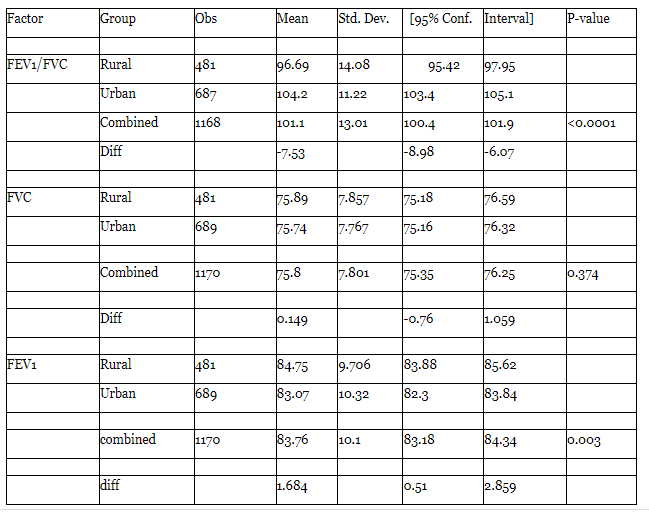
The mean FEV1/FVC were 96.69% (SD 0.64) and 104.2% (SD 0.43) respectively observed in rural and urban area. The two means varied significantly with a p-value of <0.0001. The mean FVC between rural and urban did not vary significantly while the mean FEV1 in the rural (84.75% SD 0.44) and urban (83.07% SD 0.39) varied significantly with the p-value 0.003. Table 5 below presents the mean differences of the lung functions between rural and urban area.
Factors associated with a declined lung function at bivariate analyses in rural and urban areas
Table 6 below present’s results of the bivariate analysis and only one factor showed a statistically significant association with declined lung function. Cooking fuel was statistically significantly associated with a declined lung function (p – value 0.005) while gravida only showed a weak association with declined lung function at p value 0.056.

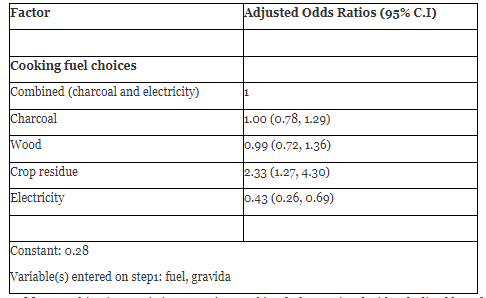
Association between cooking fuel choices and declined lung function at Multivariate analyses in rural and urban
After running a multivariate analysis to determine the association between declined lung function and the type of cooking fuel, the findings indicate there was a statistical significant relationship between cooking fuel of choice and declined maternal lung function. Compared with pregnant women who use combined type (charcoal and electricity), pregnant women using crop residues as cooking fuel are two times more likely to have a declined lung function [AOR 2.33 (1.27, 4.30)] and those who use electricity only are 57% less likely to have declined lung function [AOD 0.43 (0.26, 0.69)]. Table 7 summarizes the findings of the multivariate logistic regression.
Discussion
Our study findings indicate a high biomass use for cooking among pregnant women in the study population. Compared to the urban areas, rural areas recorded the highest level of biomass use, an observation that is comparable with most sub-Saharan African countries where previous studies indicate consistent results of high level of solid fuel use for cooking especially in the rural areas when compared with the urban areas [22,23]. The use of solid fuel as a primary source of household energy is consistent with the findings in previous studies in other developing countries, a study in Ethiopia observed that solid fuel in form of crop residues, firewood and animal dung was the primary source of household energy [24] in most households.
In our study, use of mixed fuel for cooking showed no adverse effect on respiratory functions compared to the use of biomass only. However, a contrasting result from a study conducted in India found that women using mixed fuel experienced more respiratory symptoms, followed by biomass, stove and LPG users [25]. Our current study found that use of crop residue for cooking was more likely to cause a declined lung function compared to use of mixed type of cooking fuel. This finding is supported by the fact that the efficiency of cooking with cleaner fuels is higher compared with crop residues. Crop residue is at the bottom of the energy ladder and this is one of the reasons that commercial fuels such as electricity or LPG are considered to be superior to crop residue and dung [26]. The fact that crop residues are more inefficient than other fuel types, it also follows that they emit high levels of pollutants compared to other fuel types, increasing the risk of poor lung function among the women using this type of cooking fuel. Women who used electricity only for cooking in our study were less likely to have poor lung function result compared to those who used mixed fuel types. This is an expected finding, however, it is sad to note that only 12.4% of the study population reported use of electricity only for cooking. The large majority use solid fuels such wood, charcoal, crop residue and mixed (charcoal and electricity). This scenario is comparable to many other countries in sub-Saharan Africa [20]. A study conducted in Addis Ababa reports that traditional fuels (wood, charcoal and dung) meet about 75% of household energy needs in Ethiopia and the remaining 25% is provided by kerosene, LPG and electricity [27,28]. Unlike Ethiopia where, the price of electricity has declined by more than 50%, being sold at approximately 75% less than the price of kerosene [29], the price of electricity in Zambia is on the higher side for an average Zambian household and most households that have electricity in their houses prefer to use it for lighting and not cooking as cooking is said to consume a lot of energy leading to unaffordable high electricity bills [30] (Zambia Energy Sector Report, 2014).
A strong correlation between use of biomass fuel for cooking and reduced pulmonary function was recorded in our study. This finding is in accord with a large body of evidence [11,20,30,31,32]. However, it is also important to note that reduction in pulmonary function has not been consistently documented by all researchers. In a previous study to assess the impact of different cooking fuels on pulmonary function among nonsmoking women, Reddy el al observed no correlation between biomass cooking fuel and pulmonary function [22]. The researchers attributed the absence of the expected adverse effects of biomass on pulmonary functions to better ventilation in the cooking environments of women in the biomass group compared to previous studies that support our findings.
Conclusion
The findings of our study proved evidence that use of cooking fuel options that are at the bottom of the energy ladder is a strong determinant of declined lung function. The availability and affordability of cleaner fuels in both rural and urban areas should be improved through promoting and harnessing technologies that are important in the development of affordable, high efficient and low-emission cooking fuel options.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
