
Research Article | DOI: https://doi.org/10.31579/2640-1045/037
1 Department of Adult health and critical care, Sultan Qaboos University and Hospital, Muscat, Sultanate of Oman.
2 Abbotsford Regional Hospital, British Columbia, Canada
*Corresponding Author: Melba Sheila D'Souza, Department of Adult health and critical care, Sultan Qaboos University and Hospital, Muscat, Sultanate of Oman
Citation: Melba Sheila D'Souza, Eilean Lazarus Rathinasamy, Education and Exercise on the Quality of Life among Adults with Chronic Renal Disease .J. Endocrinology and Disorders, Doi:10.31579/2640-1045/037
Copyright: © 2018 Melba Sheila D'Souza et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 August 2018 | Accepted: 22 August 2018 | Published: 27 August 2018
Keywords: quality of life; kidney disease quality of life; education; exercise; chronic renal disease; end-stage renal disease; hemodialysis
Objective: Evaluate the effectiveness of education and exercise on the quality of life among adults with chronic renal disease (CRD) on hemodialysis post-intervention (4 and 8 weeks).
Methods: An evaluative true intervention approach was used. An ethical approval was obtained from the institutional ethics committee. A random sample of 150 patients (75 in intervention and 75 in control group) with CRD receiving dialysis was selected based on the inclusion criteria. The intervention group received interactive education and supervised exercises. RAND health-related kidney disease QOL (KDQOL) questionnaire was used.
Results: Mean scores for the Kidney Disease and general QOL sub-scales among the intervention group were higher and statistically significant (p<0.01) compared to the control group. Conclusion: Education and exercise was shown to have a positive effect on the physical and mental health among the adults.
Chronic kidney disease (CKD) or chronic renal disease (CRD) is a progressive loss of renal function overtime causing a slow decline in kidney function [29]. CRD may be caused by chronic hypertension, diabetes, congestive heart failure, lupus or sickle cell anemia and initiated by acute disease processes like sepsis (infection), shock, trauma, kidney stones, kidney infection, drug toxicity (aspirin or lithium), poisons or toxins (drug abuse) or after injection with an iodinated contrast dye (adverse effect). CRD may result in a life-threatening metabolic imbalance [3] and leads to end-stage renal disease [1]. In India, the causes of end-stage renal disease (ESRD) are diabetic nephropathy, hypertensive nephropathy, chronic pyelonephritis, autosomal polycystic kidney disease and obstructive uropathy [22]. The approximate prevalence of CKD is 800 per million population (pmp) and the incidence of ESRD is 150-200 pmp. There is no data on the true incidence and prevalence of chronic renal failure in the developing world [1]. Hence, CRD is a distressing medical, social and economic problem for adults and their families.
People with CRD surface with physical and emotional changes related to their disease and its treatments. They can live independently if they are able to function, both physically and mentally [26]. Physical and mental function are inversely correlated with the risk for hospitalization and mortality (15). Health-related quality of life (QOL) refer to the measure of adult's functioning, well-being, and general health perception in each of three domains: physical, psychological, and social among adults with CRD. CRD influences QOL and QOL is predictor of outcome in CRD. Adults with CRD on dialysis have lower level of QOL. QOL of adults with CRD is influenced by the disease and by the type of replacement therapy. QOL is an indicator of the effectiveness of the medical care they receive.
Background
QOL is compromised, by fatigue and encounters in planning meals and limiting fluids. Adults' social and role responsibilities may be altered due to problems with travel, impotence, and changes in body image [13]. Education, social support, and self-care have been shown to raise coping skills among people on dialysis [33]. Emotional adjustment, adherence to treatments, positive attitude, exercise, and engagement in life pose challenges to adults with CRD [16]. Kidney failure, treatment choices, medications, and the renal diet can help adults with CRD on dialysis to maintain a sense of control, a factor linked to improved adherence and life satisfaction [23]. Early education about renal disease, and the potential to live long can aid in overall adjustment and decision making for people on dialysis [37].
Informed adults have reported fewer symptoms as well as more confidence in their ability to manage the symptoms they do have. Supportive social environments have shown a positive impact on adjustment for people with renal disease [10]. Support received from their families and dialysis staff was a major factor in promoting employment; an activity that contributes to emotional health [31]. With education and support, people on dialysis can begin to make careful, informed decisions about their treatment [18]. Renal rehabilitation is an optimal functioning for adults and restoration to productive activities [32] and the “5 E's”- encouragement, education, exercise, employment, and evaluation are used [21]. Energy and activity levels, functional ability, sleeping and eating behaviors, disease symptoms, health status, sex life, well-being, psychological effect, satisfaction with life and health, and happiness was found to affect QOL in young and elderly adults [11]. There is no data to explore the effect of combined education and exercise on the QOL among adults with CRD on hemodialysis [34]. Hence this study was conducted to examine the effects of combined education and exercise on QOL among adults with CRD.
Conceptual model
Adaptive system model (Roy, 1984) was used in this study (Figure 1).
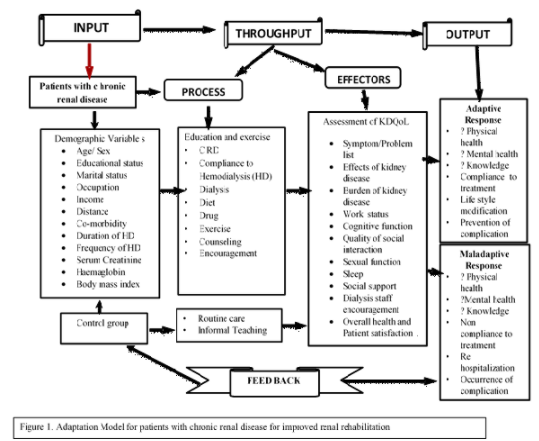
The adaptive system (person) has inputs of stimuli includes variables, outputs as adaptive responses that serves as feedback [28]. Individual is a whole and dysfunction in one component
affects the entire system. The inputs is identified as stimuli are age, gender, educational status, occupation, economic status, co-morbidity, frequency of dialysis, hemoglobin level, serum creatinine and body mass index. Throughput makes use of a person processes and effectors. The processes used for intervention group special intervention like education, exercise, adherence to treatment options, dialysis, diet, drug, exercise, counseling, and encouragement. Effectors refers to the assessment of Kidney Disease QOL which includes physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health. Output
is the outcome of the system. When the system is a person, output refers to the person’s behaviors. In the intervention group the adaptive responses are used when a person demonstrates behaviors that achieved the goals like better physical health, mental health, knowledge and adherence to treatment.
Aim
Effectiveness of education and exercise on the quality of life among adults at base line and post-intervention with chronic renal disease on hemodialysis.
Design
An evaluative true intervention approach using randomized pre-test and post-test control group design was employed to evaluate the effectiveness of education and exercise on the quality of life among adults on hemodialysis. This study instituted two groups, an intervention group exposed to education and exercise and the control group with usual care.
Selection and description of participants:
This study was conducted at a selected multi-specialty hospital with high-tech dialysis center consisting of 12-bedded unit with hemodialysis. The target population was adults with CRD subjected to hemodialysis at the dialysis unit during the period of data collection in 2012.
A sample size of 64 was determined using mean difference for a power of 0.80, a medium effect of 0.80 with p<0.05 (Cohen 1992). A total sample size of 75 adults was estimated for intervention and 75 adults for the control group to reduce the rate of attrition (Figure 2. Consort diagram).
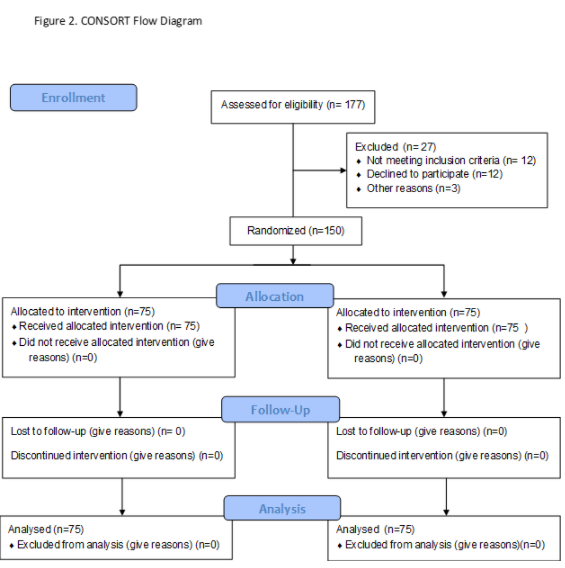
A random probability sampling was used to select the total sample of 150 adults with CRD undergoing hemodialysis. Adults with CRD on hemodialysis who fulfilled the inclusion criteria (elective basis, more than 6 weeks on dialysis, and age group of 20-70 years) during the data collection period were recruited to participate in the study. Adults who were known to have psychiatric disorder, and altered level of consciousness were excluded from the study.
Measurements:
The Kidney Disease Quality of Life- Short form (KDQOL-SF) instrument is a self-report measure developed for individuals with kidney disease and on dialysis [12]. It includes 43 kidney-disease targeted items and 36 items of SF that provide a generic score and an overall health rating item. It focus on particular health-related concerns like Symptoms/Problems (12 items), Effects of kidney disease on daily life (8 items), Burden of kidney disease (4 items), Work status(2 items), Cognitive function (3 items), Quality of social interaction (3 items), Sexual function (2 items), Sleep (4 items), Social support (2 items), Dialysis staff encouragement (2 items), adult satisfaction (1 item) (KDQOL-SF 1997). The KDQOL-SF includes a 36 item health survey (RAND 36-item health survey) as the generic core (12). It consists of 8 multi-item measures of physical and mental health status: physical functioning (10), role-physical (4), bodily pain (2), general health (5), vitality (4), social functioning (sf) (2), role-emotional (re) (3) and mental health (5). An overall health rating item rates their health on a 0-10 response scale ranging from worst possible to best possible health. A score between 0 and 100 is calculated on the basis of well-defined guidelines, with a higher score indicating a better state of health. The 80 KDQOL-SF take about 16 minutes to complete. The reliability of the KDQOL-SF was r=0.80 in this study. Hence the instrument was valid and reliable for the study.
Demographic variables consist of age, gender, educational status, occupation, marital status, place of residence, type of family, family monthly income, distance of residence from hospital and medical insurance. Clinical variables include presence of co-morbidity, frequency of dialysis per week, physical activity, hemoglobin level, serum creatinine and body mass index.
Intervention:
Renal rehabilitation is defined as an optimal functioning for adults and restoration to productive activities. To nurture renal rehabilitation and guide program development, the Life Options Rehabilitation Advisory Council (LORAC) identified five core principles, called the “5 E's”—Encouragement, Education, Exercise, Employment, and Evaluation. Renal Rehabilitation Program with intervention include interactive education, exercise, life style modification, and coping was developed by the investigator and validated for content and concepts. Online, videos and CDs provided information based on the perceived needs of adults with CRD and life style modification, orientation to health team members, structure and functions of the kidneys, hemodialysis, stages of kidney failure, causes of CKD, signs and symptoms, tests, treatment, dietary guidelines and modification, quitting smoking and alcohol, strategies for slowing progression and treating conditions underlying chronic kidney disease, complications of chronic kidney disease may require medical treatment, dialysis and its impact, exercise, sexual life alteration , change of work, recreation and planning for holiday with their family members and process of leading to near normal life style. The sessions on education and exercise were provided in the local vernacular language before the dialysis. Counselling was provided by the nephrologists and the unit nurses. The control group subjects received the usual treatment and no intervention.
Data collection:
An ethical approval was also obtained from the Institution Ethics Board. The permission to conduct research in Dialysis Unit was obtained from concerned authorities. The eligible participants were identified from the hospital medical records after obtaining permission. Ethical principles were adhered too throughout the study. The purposes of the study and their right to participate or withdraw from the study were explained with written informed consent. Adults who volunteered and fulfilled the inclusion criteria were enrolled for the study. Baseline data on demographic variables was collected using interview technique. Privacy was provided during the data collection. Baseline data was collected from the selected voluntary adults with CRD in 2012. The first post test was taken after 4 weeks before initiating dialysis and reinforcement was given. The second post-test was taken after 8 weeks of the first post test before initiating dialysis and after the reinforcement was given on the same.
Data analysis:
SPSS21 was used to analyze the descriptive and inferential data. Paired ‘t’- test, independent ‘t’–test were applied to determine the effectiveness of education and exercise. Test of homogeneity indicated no significant difference between the groups in the demographic and clinical variables.
Demographic and clinical variables
One-third of the adults were 40-49 years in the intervention (31%) and control group (41.3%) (Table 1). One-third of the adults had primary education in the intervention (32%) and control group (42.7%).
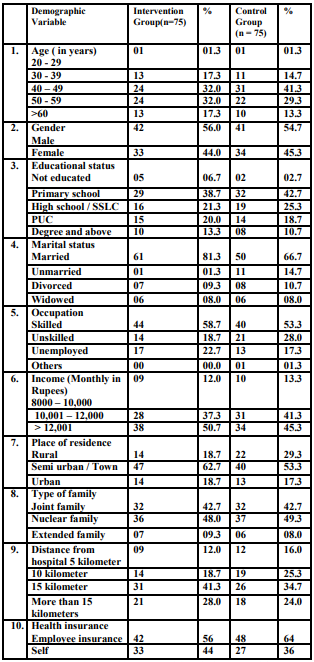
Majority of the adults lived in the town in the intervention (62.7%) and control group (53.3%). Majority of the adults had dialysis more than once a week in the intervention (80%) and control group (73.3%) (Table 2).
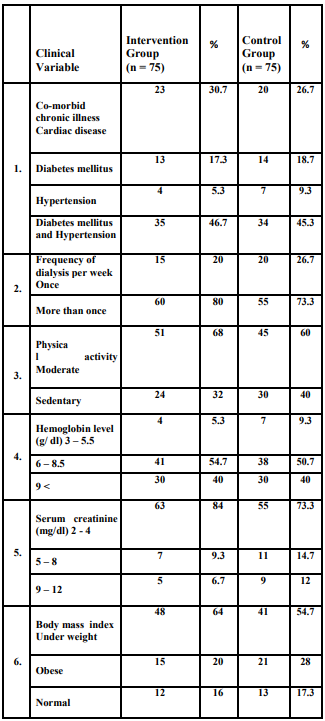
Half-percentage of the adults had low hemoglobin in the intervention (54.7%) and control group (50.7%). Kidney disease quality of life after education and exercise
There is no differences in the KDQOL between the intervention and control group in the pre-test (Table 3).
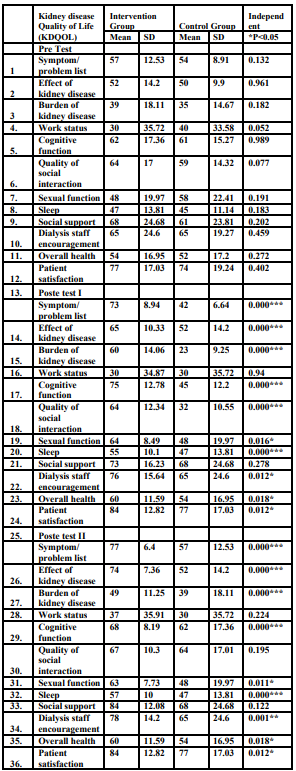
The mean scores of the KD QOL was significantly higher with symptom, effect of kidney disease, burden of kidney disease, cognitive function, sexual function, sleep, social support, encouragement, overall health and satisfaction in the intervention group compared to the control
group in the post-test 1. The mean scores of the KDQOL was significantly higher with symptom, effect, social support, encouragement, overall health, and satisfaction (p<0.001) in the intervention compared to the control group.
General QOL after intervention
Mean QOL scores of physical functioning, role physical, pain, general health, role emotional, social function, were significantly higher in the intervention group compared to the control group (p<0.001) (Table 4).
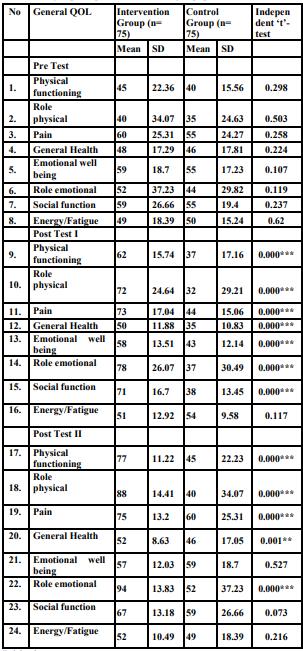
Mean QOL scores of physical functioning, role physical, and role emotional were higher in the intervention group compared to control group (p<0.001).
Physical and Mental Composites of General QOL
The mean scores of the QOL physical composite significantly improved among the intervention group compared to the control group (p<0.001) in the post-test 1 and post-test 2 (Table 5).
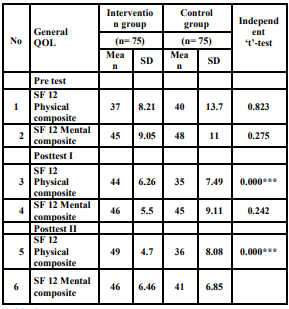
*P<0.05
Association between variables and KDQOL
Middle age (40-59 years), male gender, higher income (more than 12,000 IRS) were significantly associated with QOL among adults in the intervention group (Table 6).
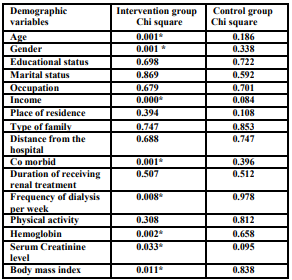
*Significant at p <0.05
Co-morbidity (DM and Hypertension), frequency of receiving dialysis more than once /week, moderate anemia (6-8.5 g), low Serum Creatinine (2-4 mg/dl), and underweight BMI were significantly associated with QOL among adults in the intervention group.
In this study education and exercise improved physical functioning among adults on hemodialysis leading to an improvement in their quality of life. Education and exercise had a positive effect on improving the quality of life of adults with dialysis. Other studies showed that increased QOL had a significant decrease in serum urea, intradialytic weight gain, and improving QOL [20]. Increased QOL was observed after an intradialytic exercises [25]. Education influences dietary compliance and medication regimen improves serum albumin and hemoglobin [35].
In this study middle age group, men, higher income, dialysis more than once /week, moderate anemia, low Serum Creatinine, and underweight BMI were significantly associated with QOL after intervention at 8 weeks among the intervention group. Education, diet, and regular exercise had a better impact on the adults on hemodialysis. Men who are independent, self-controlled good family support and good biochemical control have better QOL. Better QOL mean scores were observed among men, those married, working, good hemoglobin, low serum creatinine among adults with hemodialysis [27]. Cognitive function and quality of social interaction and QOL was associated with older age, socio-economic and higher educational level among adults on HD in Romania [7]. Education and employment influenced the physical and social domains of QOL as they are aware of the quality of service and individual rights [6].
In this study intervention group that participated in education and exercise showed better physical functional and QOL than the control group. These positive effects of participating in an education were seen after 8 weeks of dialysis treatment. Adults exposed to pre-dialysis education scored significantly better mood, less functional disabilities compared to the comparison group [36]. Education improves knowledge and self-management and treatment efficacy [4]. Physical exercise increased physical function among adults on hemodialysis [24] and increased exercise capacity, improves muscle function [6].
In this study education for adults with end-stage renal failure was found to improve QOL. Other studies showed that physical composite scores were correlated with age, hemoglobin and comorbidity, and mean PCS was lower in depressed adults on hemodialysis [19]. Physical functioning scale were significantly lower for obese subjects than for those with normal weight or moderately high BMI [9]. QOL of the intervention group was higher than the control group in 50% of the dimensions in KDQOL-SF and reported better emotional state, less bodily pain, improved social functioning and fewer problems with work [18]. QOL improved by 20% in coping among adults with hemodialysis [2].
In this study, the intervention group had higher general and kidney disease QOL compared to control group, except for energy fatigue, emotional well-being, social function and energy fatigue, work status, quality of social interaction, and social support. Physical and mental composites of general QOL were higher in the intervention group compared to the control group. Reduction in HRQOL of elderly adults of the same age and gender was lower than in younger adults. Elderly adults on hemodialysis had relatively better HRQOL [30]. Intervention improves QOL among adults with CRD [8].
In this study, physical, mental domains have significantly influenced QOL. QOL was improved with interactive education and supervised exercise among adults with CRD. Education and exercise improves knowledge and QOL and impacts adults with hemodialysis. Adults with CRD are encouraged to accept responsibility for their health and self-care. Education and exercise was shown to be a positive predictor of physical and mental health for people on hemodialysis as they have reported fewer symptoms and confidence in their ability to manage the symptoms they do have. They have reported better subjective quality of life, including social and role functioning, and emotional well-being. Hence education and exercise can enhance the potential for physical activity and improved quality of life and may influence other important outcomes.
A small sample size and past experiences among adults with dialysis may influence the results.
Implications
Adults with CRD may take more responsibility for things they can control, including exercise, remaining actively engaged in life, and renal meal plan. Their involvement in self-care can positively affect their adherence with treatment regimens. Education, exercise, staff encouragement toward education, exercise rehabilitation help adults form positive attitudes that will allow them to participate actively in life. Encouragement and counseling especially from families and dialysis staff, can increase autonomy, control, and participation in treatment. Adults with CRD on hemodialysis are encouraged and reinforced to learn about their self-care for improved quality of life. They take more responsibility for domains that they can control, including exercise, being actively engaged in life, and renal meal plan.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
