
Research Article | DOI: https://doi.org/10.31579/2642-9756/075
*Corresponding Author: Michel Alary, Département de médecine sociale et préventive, Université Laval, Québec, Canada.
Citation: Gentiane Perrault Sullivan, Fernand Aimé Guédou, Fatoumata Korika Tounkara, Luc Béhanzin, Nana Camara. et all (2021) Reproductive History and Pregnancy incidence of Malian and Beninese female sex workers before and During Sex Work Practice. J.Women Health Care and Issues, 4(6); DOI:10.31579/2642-9756/075
Copyright: © 2021 Michel Alary, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2021 | Accepted: 26 June 2021 | Published: 30 June 2021
Keywords: sex workers; therapeutic abortion; pregnancy; reproductive health; sub-saharan africa
Aim/Background: To reduce maternal mortality (MM), access to family planning and reproductive health care services are key strategies. Access to and use by marginalized populations pose a substantial challenge. The objective of this study was to describe the reproductive history of female sex workers (FSWs) before and during sex work.
Materials and methods: FSWs aged ≥18 years were recruited in Benin, and Mali, to answer a questionnaire during a face-to-face interview. Descriptive analyses were carried out and comparisons made between countries (Pearson chi-square) and between the periods before (BSW) and during sex work (DSW) practice within women in each country (McNemar chi-square). In addition, multiple imputations were used to estimate and compare the incidence rate of pregnancy BSW and DSW calculated with a generalized linear model for count data with a Poisson distribution and a log link.
Results: Mean age was 26 years in Mali (n=322) and 35 years in Benin (n=330). More women had at least one pregnancy BSW compared to DSW in both Mali (62.1%-vs-33.5%) and Benin (91.2%-vs-32.7%). The pregnancies occurring DSW had lower livebirth rates (57.9%-vs-74.7% Mali, 17.6%-vs-60.6% Benin) and ended more often with a therapeutic abortion, DSW compared to BSW, especially in Benin (65.2%-vs-25.6%). The level of complications associated with therapeutic abortion was high, both DSW (23%) and BSW (20%). The incidence rate of pregnancy was about twice lower DSW compared to BSW [incidence rate ratio (IRR): 0.49; 95% confidence interval (95%CI): 0.37-0.66-Mali and IRR: 0.45; 95% CI: 0.32-0.63-Benin].
Conclusion: In both Benin and Mali, FSWs had more pregnancies during the period preceding sex work practice, about twice more than during sex work when considering the differences in incidence rates. Single mothers need to be supported to avoid sex work as a financial solution. On the other hand, the reproductive needs of FSWs need to be acknowledged to reduce maternal mortality within this marginalized population. It is of paramount importance that interventions remain focused on reproductive health and prevent unwanted pregnancies, answer contraceptive needs and provide safe therapeutic abortions.
BSW: Before sex work
CI: Confidence interval
DSW: During sex work
FCFA : Franc des communautés financières africaines
FSW: Female sex workers
HIV: Human immunodeficiency viruses
HPV: Human papillomavirus
MM: Maternal mortality
IR: Incidence rate
IRR: Incidence rate ratio
MICE: Multiple imputations by chained equations
NGO: Non-Governmental Organisation
One of the main action to promote health in the 2030 agenda for sustainable development, proposed by the World Health Organization, is to achieve health equity [1]. Maternal mortality and access to family planning constitute two inequity-related indicators. The global fertility rate in sub-Saharan Africa is 4.6 births per woman during lifetime [2] which is three times the rate in European Union and Canada [3].The maternal mortality rate in this region is also the highest in the world with 542 deaths per 100 000 live births reported in 2017 [4], thus accounting for roughly two thirds of maternal deaths worldwide [4, 5]. In Benin, one in 49 women risks dying due complications of pregnancy and/or childbirth and one in 29 in Mali [4]. To reduce maternal mortality, universal access to family planning and reproductive health care services remains a key strategy globally.
Marginalized populations are groups that experience discrimination and exclusion because of unequal power relationship across economic, political and cultural dimensions [6]. Because of this exclusion and discrimination, marginalized populations pose a substantial challenge worldwide when it comes to preventing maternal death through use of and access to family planning and reproductive health services [7, 8].
Sex workers are known to experience discrimination especially in accessing health services [9, 10]. In West Africa, it is estimated that one in 20 women has ever practiced sex work [11] and most African female sex workers (FSWs) are mothers [12, 13].. Moreover, sex work is associated with many risks that increase pregnancy complications, as well as maternal mortality and morbidity [14]. For example, HIV accounts for 5.5% of the maternal mortality [15] and among FSWs, HIV prevalence is 12 times higher than in the general population [13]. Unsafe abortion can explain up to 13% of the maternal mortality [16] and lifetime abortion varies between 35 and 65% among FSWs in low and middle income countries [17-20].
Despite all these risks and stigma surrounding sex work [21], FSWs have the same rights and desires as women from the general population, regarding pregnancy [22]. Yet, FSWs are underrepresented in fertility-related researches [22] and most of the programmes specifically targeting FSWs often ignore broader sexual and reproductive care needs and family planning [23].
Meeting the reproductive health needs of this marginalized population is required to prevent maternal mortality [24] and to reach the World Health Organization Sustainable Development Goal that states that by 2030, we need to ensure healthy lives and promote well-being for all at all ages. One of the key priorities is to improve maternal health. To do so, we need to have a better knowledge of the reproductive history of FSWs, not only during their sex work practice, but also before. Most of the researches have been fragmentary in describing their reproductive history (unwanted pregnancy or therapeutic abortion) [25], generally covering their entire lifetime (without differentiation between before sex work practice and during involvement in sex work) [18, 26] or only a small time period [27, 28]. Thus, until now, there is no understanding of the full picture of the reproductive history of FSWs. As a result, many questions remain unanswered and because of this lack of knowledge it is difficult to know which intervention to prioritize and at what moment in a women’s life the intervention should be available...
The objective of this study was to fulfill these knowledge gaps by describing FSWs’ reproductive history before and during sex work in two West African countries (Mali and Benin). To achieve this goal, we first described pregnancy outcomes. Then we characterized the therapeutic abortions. Finally, we calculated and compared the pregnancy incidence rate before and during sex work.
The recruitment for the present study was combined with another one investigating cervical cancer and human papillomavirus (HPV) infection among FSWs [29]. This collaboration was made to avoid soliciting the same population for two studies over a short time period. However, the development of the present study was distinct from the one investigating cervical cancer and HPV. To recruit FSWs, trained peer educators and senior staff from participating non-governmental organisations (NGOs) conducted cervical cancer awareness activities in bars, brothels and hotels, etc. Following these activities, women were referred by peer educators to FSW-friendly clinics Dispensaire IST (DIST) in Cotonou, Benin, and Clinique des Halles run by ARCAD/SIDA, a national NGO, in Bamako, Mali for cervical cancer screening. After participating in the HPV study, they were offered to participate in the study on reproductive history for which they had to complete a questionnaire administered face-to-face. However, FSWs who declined participation in the HPV study or were excluded from it because they were pregnant were also offered to participate in the present study. 330 women were recruited in Cotonou, Benin, between March and June 2017 and 322 in Bamako, Mali, between November 2017 and February 2018.
Inclusion criteria
FSW was defined as any woman who regularly receives money in exchange for sex. To be included in the study, FSWs also needed to have been involved in the sex trade for at least six months in either Cotonou, Benin, or Bamako, Mali, to be aged 18 years or older and to provide written informed consent. All FSWs included in that study are working for money and to our knowledge were not forced to.
Data collection
A quantitative questionnaire developed by the research team was administered during a face-to-face interview by a qualified interviewer. We collected data on reproductive history, pregnancy intention and contraception. Also, a pelvic examination and a urine pregnancy test were carried out by a physician.
All the data regarding sociodemographic characteristics as well as the HIV and pregnancy test results were extracted from the HPV study dataset.
Missing data
Some participants of the study who were excluded from the HPV study because of a positive pregnancy test (n=18 in Mali and n=13 in Benin) did not complete the sociodemographic section of the questionnaire that was only included in the HPV study questionnaire. The sociodemographic data were backtracked for some women in their medical file, but we could not retrieve the missing data for all women. In addition, women included in both studies had some missing values for different variables. Although, the number of women with entirely missing sociodemographic information was low, we used multiple imputation to compensate for these missing data because most of the exclusions from the HPV study were because of pregnancy at the time of enrolment and we wanted to avoid the introduction of a selection bias since pregnancy is the outcome of interest.
Multiple imputation
We wanted to have a complete data set to calculate the incidence rate of pregnancy before and during sex work practice. We used an imputation model with multiple imputations by chained equations (MICE). We decided to use MICE because all the missing values had a non-monotonous pattern and we had to impute different types of variables [30]. We used the distribution of the observed data to estimate the plausible values for the missing data. We included all the variables needed to assess the incidence rate in the imputation model and further added all the variables that were associated either with the variables that had missing values or with the presence of missing values for a given variable [31], as required to obtain valid MICE models. The number of imputations needed was decided based on the rule of thumb [31]. This rule suggests that the number of imputations should at least be equal to the percentage of incomplete cases. The linear variables were not transformed even if they were skewed. We used predictive mean matching to improve the estimation and avoided transforming the relation between the variables in the imputation model [32, 33].
Incidence of pregnancy before and after sex work
The incidence rate was calculated as the total number of pregnancies over the person-time at risk [34]. To calculate the amount of time at risk for pregnancy during sex work practice we used the duration declared by FSWs at the question: for how long have-you been practicing sex work? To calculate the time at risk before sex work practice, we subtracted the duration of sex work from the period of time between age at recruitment and the age at first sex to obtain the amount of person-time at risk before sex work for each woman. To be able to discriminate between pregnancy occurring before and during sex work practice, FSWs were asked specifically how many pregnancies they had before practicing sex work and how many during sex work practice. Furthermore, to validate those results we asked how many pregnancies each woman had during her lifetime and the total was compared with the aggregate for the two periods. Finally, the total number of pregnancies for each period was compared with the summation of the outcomes. When a discrepancy was observed, a verification was made with the research coordinator in each country.
Statistical analyses
To present the studied population characteristics we used descriptive analyses (frequencies, means values with standard deviations). We also present a comparison between the two countries using Pearson chi-square.
Furthermore, we used descriptive analyses and paired comparisons (McNemar’s chi-square for discrete variables and paired Student’s t test for continuous variables with normal distribution) in each country, to assess differences in outcomes (pregnancy, therapeutic abortions) according to the period when they occurred (prior to or during sex work practice). For the descriptive analyses, a p-value of 0.05 or less was considered statistically significant.
Thereafter generalized linear model for count data with a Poisson distribution and a log link was used to compare the incidence rate of pregnancy before and during sex work. The log of the duration of the periods before and during sex work was used as offsets in the models. Generalized estimating equations were used to consider the correlation between the periods before and during sex work for a given woman. This analysis was performed with the original as well as the imputed databases. We performed all the analyses using SAS 9.4 (SAS Institute, Cary, NC, USA).
Ethical considerations
Each participant provided a signed informed consent and no nominal information was reported on the questionnaire. The participants received a monetary compensation to cover their transport fees and the possible loss of income due to their participation (5 US dollar in Mali and 2 US dollar in Benin).
The study was approved by the ethics committees of the CHU de Quebec – Université Laval (Quebec City, Canada) and the School of Medicine of Bamako, Mali, as well as by the National Health Research Ethics Committee in Benin. Moreover, all methods were performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki).
Missing data
Of the 652 FSWs, ten (3.1%) had missing data in Mali for all the sociodemographic variables. In Benin, since we were able to recover some information, seven (2.1%) women had missing information for all sociodemographic variables. We had no missing data for the pregnancy variables (number, outcome and period of occurrence of the pregnancy). For the variables characterising therapeutic abortion, we had five (1.3%) missing data for therapeutic abortion occurring before sex work and four (2.3%) during sex work. We had respectively 16.1% (105/652) of missing data for the number of years before practicing sex work and 5.2% (34/652) for the number of years during sex work practice. For the data set used to calculate incidence rate, 82.2% of the women had no missing information.
Multiple imputations
We did 20 imputations to impute variables for the incidence rate analysis. We used 15 variables in the imputation model. They included the number of pregnancies before and during sex work, the time variables (number of sexually active years while fertile preceding sex work and the number of years as a sex worker), the variables that both predict the number of sexually active years while fertile preceding sex work practice and the number of years as a sex worker and those predicting missing data for each of the latter variables (country, country of origin, religion, education, marital status, number of biological children and HIV status).
Descriptive analyses
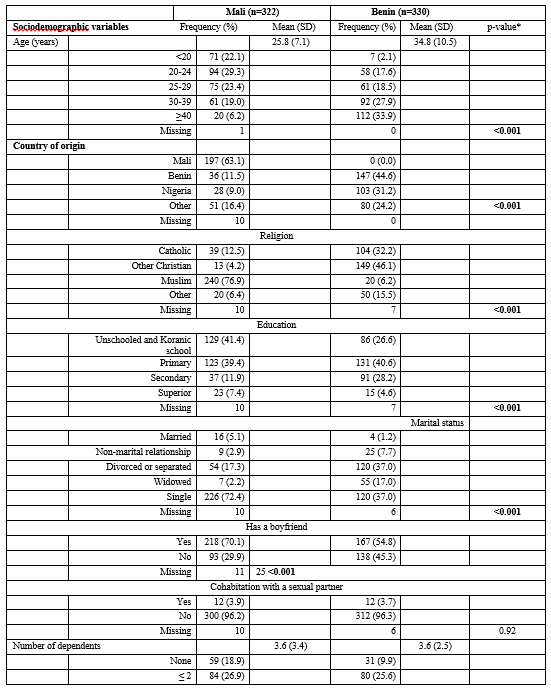
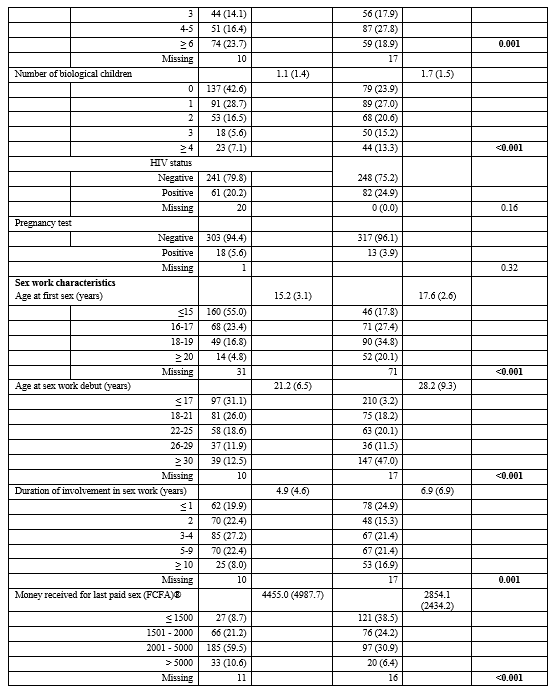
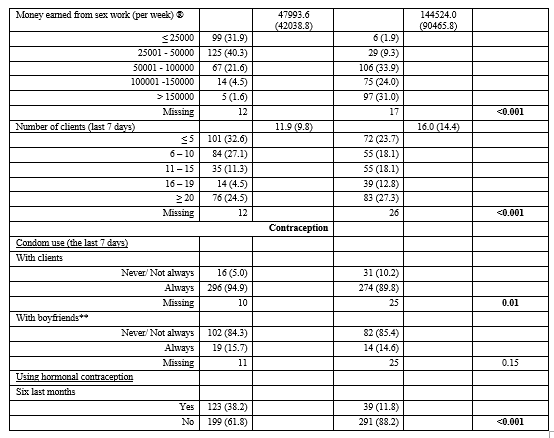
Table 1 shows the sociodemographic and sex work characteristics of the participating FSWs. Women in Benin were older (mean age 34.8 vs 25.8 years - p-value <0 xss=removed xss=removed xss=removed xss=removed xss=removed>
Comparison of pregnancy and therapeutic abortion’s prevalence before and during sex work practice
In Mali, during their lifetime, 79.5% of the FSWs had at least one pregnancy and 50.9% more than one (Table 2). 14.9% of the women had at least one therapeutic abortion which represented 18.8% of the women who ever had a pregnancy (data not shown). In Benin, almost all FSWs (95.2%) had at least one pregnancy, 87.9% more than one pregnancy and more than half of them (57.0%) at least one therapeutic abortion (Table 1).
By comparing the period during sex work practice and the period preceding, we saw a different picture (Table 2). More women had at least one pregnancy before sex work than they did during sex work in both countries (p-value <0>
Table 2: Comparison of pregnancy and therapeutic abortion’s prevalence between sex work practice and the period preceding (n=652)

By comparing the period during sex work practice and the period preceding, we saw a different picture (Table 2). More women had at least one pregnancy before sex work than they did during sex work in both countries (p-value <0>
Fewer women had resorted to therapeutic abortion in Mali than in Benin (14.9% vs 57.0%). In Benin, of the women who had at least one pregnancy, over half of the women had had a therapeutic abortion (59.9 %) during their lifetime and almost two out of three women who had a therapeutic abortion had more than one (64.4%) regardless of the period (data not shown).
Depiction of pregnancy outcomes before and during sex work practice
In Mali, FSWs had a total of 470 pregnancies before sex work practice and 131 while practicing sex work (Table 3). Most of the pregnancies led to livebirths. Before sex work, it was three out of four (74.7%) and slightly more than one out of two during sex work (57.9%). Approximately the same proportion of pregnancies (13%) resulted in a therapeutic abortion both before and during sex work. Regarding pregnancies during the sex work period, most of them were from boyfriends (82.4%), and followed by husbands with 13.2%. Most of the pregnancies from husbands (90.5%) led to livebirths, with 9.5% of miscarriages. Finally, 14 Malian FSWs (8.8%) knew they were pregnant at the time of recruitment and 4 learned they were with the pregnancy test result.
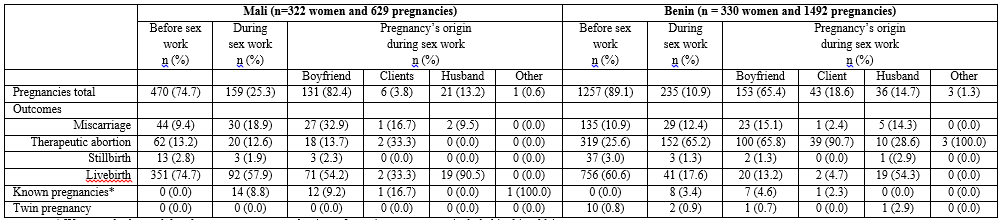
In Benin, FSWs had a total of 1257 pregnancies before sex work and 235 while practicing sex work. There was an important decrease in the livebirth rate from the period before sex work (60.6%) to that of sex work (17.6%). Expectedly, the therapeutic abortion rate markedly increased from 25.6% to 65.2
The aim of this research was to describe the reproductive history of FSWs, a marginalized population, in both Mali and Benin. To acquire a global portrait of their realities, we described their reproductive history not only during sex work practice but also before. The main observation is that FSWs had more pregnancies leading to livebirths during the period preceding sex work practice. In Benin as in Mali, the incidence rate of pregnancy declined by half after the initiation of sex work. It is worthy to note that although fewer pregnancies occurred during sex work practice, the ones occurring during that period had lower livebirth rates and higher therapeutic abortion frequency, with associated complications such as hemorrhage and abdominal pain, as described by the FSWs we interviewed.
The number of pregnancies before sex work practice is undoubtedly high. The fact that a large number of pregnancies have occurred before sex work practice can lead women to precariousness and economical strain especially since the vast majority of these pregnancies led to livebirths. For example, in Benin, the country with the higher number of pregnancies before sex work practice, half of the women were widowed or separated. The lack of opportunities to earn money often draws women to sex work [13, 35]. In Mali, the women were 10 years younger than in Benin but were responsible, on average, for the same number of dependents (3.6). In Mali, family poverty is a determining factor for engaging in sex work. Young girls can be driven towards sex trade to help support their family [36]. In our population, one out of three Malian FSWs started selling sex before being 17 years old.
When comparing the two countries, FSWs in Mali had twice less pregnancies during the period preceding sex work than in Benin. FSWs recruited in Mali were younger. Another factor that could explain this discrepancy is that FSWs in Benin were active sexually for a longer period before getting involved in sex work than women from Mali. Indeed, FSWs had their first sexual relation on average over two years younger in Mali (15.2 years) compared to Benin (17.6 years), but the mean age at sex work initiation was 7 years younger in Mali (21.2 years) compared to Benin (28.2 years). Consequently, women in Benin spent 10.6 of their sexually active years before selling sex rather than the six years found for Malian women. For several women, the need to take care of their children is a sufficient incentive to engage in sex work practice [37-39]. In Mali, prior to initiating sex work, almost 60% had at least one child and in Benin, it was three out of four FSWs.
The cumulative incidence of pregnancy during sex work is similar in the two countries with no regards to the outcome. Our findings indicate that a third of the FSWs had at least one pregnancy while practicing sex work. This overall cumulative incidence is high compared to what has been observed during sex work in other studies which is around 20% [27, 28, 40-43]. Social and popular judgements induce significant stigma to pregnant women during sex work practice [22]. The fact that our study inquired globally about reproductive history for their lifetime may have helped to reduce fear and shame surrounding those issues. The high frequency of pregnancies during sex work, compared to other studies, is worrisome especially considering that nursing a baby during sex work practice is undeniably an added burden for women who already are mothers [44].
Fewer pregnancies occurred during sex work. but a smaller proportion of those led to livebirths. In Mali, three out of four pregnancies led to livebirths before sex work practice compared to half during sex work. In Benin, this difference was even greater, less than one out of five pregnancies have led to livebirths during sex work, as opposed to three out of five before. These data seem to support the idea that more pregnancies are unwanted during sex work practice. Nevertheless, it must be kept in mind that is not because a pregnancy’s outcome is a livebirth that the pregnancy is intended. Low-income countries have both the world’s highest unintended pregnancy rate and the world’s lowest proportion of unintended pregnancies ending in therapeutic abortion [45]. Worldwide, it is estimated that half of the unwanted pregnancies lead to therapeutic abortion but that the other half leads to livebirths [46]. In both countries, when the husband is the father, the livebirth rate is at its highest. Yet, those pregnancies represent less than 15% in each country. Most pregnancies during sex work came from boyfriends (82% in Mali and 65% in Benin). We also observed that condom use is low with their boyfriends compared to with their clients. Not using condoms with their boyfriends helps women to make a distinction between their professional and personal lives [47], but also seems to lead to unplanned pregnancies. Moreover, in Mali, the prevalence of miscarriage doubles between the two periods (9.4
Most of the pregnancies occurred before sex work practice in Mali as in Benin. Nevertheless, resorting to therapeutic abortion was more frequent during sex work practice especially for Beninese FSWs. These results highlight the need for two types of prevention. First, single mothers, as well as divorced and widowed ones, need to be supported to avoid sex work as a financial solution. Secondly, reproductive needs of FSWs must be acknowledged and understood so that specific sexual and reproductive health interventions can be targeted towards their needs. Finally, to properly support FSWs who want to have children, more research is needed to understand the mechanisms leading to the intention of becoming pregnant in this population.
The authors thank the study participants and the interviewers for their contribution to the study. They also acknowledge the contribution of the staff of the DIST in Benin, ARCAD-SIDA, SOUTARA and DANAYA-SO in Mali.
The authors declare that they have no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
