
Re-print Article | DOI: https://doi.org/10.31579/2694-0248/076
1 Associate professor, PhD, University of “Vasile Alecsandri” din Bacau, Faculty of Mouvement, Sport and Science, Department of Physiotherapy and Occupational Therapy, Romania.
2 Associate professor, PHd, University of “Vasile Alecsandri” din Bacau, Faculty of Mouvement, Sport and Science, Department of Physical Education and Sport, Romania.
3 student, University of “Vasile Alecsandri” din Bacau, Faculty of Mouvement, Sport and Science, Department of Physiotherapy and Occupational Therapy, Romania.
*Corresponding Author: Ochiană Gabriela, Associate professor, PhD, University of “Vasile Alecsandri” din Bacau, Faculty of Mouvement, Sport and Science, Department of Physiotherapy and Occupational Therapy, Romania.
Citation: Ochiană Gabriela, Ochiană Nicolae, and Tolontan Dumitru, (2024), Reprint-Study on the Effectiveness of Neurodynamic Techniques Used in the Treatment of Lumbosciatics, J Clinical Orthopaedics and Trauma Care, 6(1); DOI: 10.31579/2694-0248/076
Copyright: © 2024, Ochiană Gabriela. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 December 2023 | Accepted: 21 December 2023 | Published: 05 January 2024
Keywords: sciatica; neurodynamics; neuroimmune system; lumbosciatics
Objectives: The research in question aims to highlight the role of mobilizing the neuroimmune system through specific neurodynamic techniques in treating the symptomatology given by lumbosciatics.
Methods: In this study I chose 14 patients, divided into two groups of 7. Group 1 being the experimental one that benefited from neurodynamic exercises and group 2 being the control one, which benefited only from classical physical therapy.
Results: The experimental group showed better results in terms of pain relief than the control group after the tests performed.
Conclusions: Following the research carried out on the two groups of patients diagnosed with the symptomatology of lumbosciatics, we can confirm the hypothesis from which we started and we can also find that this study concisely presented the use of neurodynamic techniques in the treatment of lumbosciatics.
Sciatica is the consequence of an underlying medical condition. Understanding the possible causes of sciatica can help focus treatment on addressing the root problem rather than masking the symptoms.
The mechanism of sciatic nerve damage is either a result of direct nerve compression, inflammation, an abnormal response of the body's immune system, or a combination of all these factors.
The neuroimmune system is a system of structures and processes that involve biochemical and electrophysiological interactions between the nervous system and the immune system that protect neurons from pathogens. It serves to protect neurons from diseases by maintaining selectively permeable barriers (for example, the blood-brain barrier and the blood-cerebrospinal fluid barrier), mediating neuro-inflammation and healing of lesions in damaged neurons, and mobilizing the host's defense against pathogens. (Butler D.S., 1991)
Neuro-dynamics is an innovative management tool that involves conservative nerve decompression, various neural mobilization techniques, and patient education techniques. Neuro-dynamics provides a new understanding and management strategies for common syndromes such as plantar fasciitis, tennis elbow, nerve root disorders, carpal tunnel syndromes and back pain. (Shacklock, M., 2005).
Neuro-mobilization is a method of conservative treatment of neural tissue disorders. The rationale for using neuro-mobilization in the treatment of musculoskeletal disorders is based on in vivo and in vitro studies that indicate a high efficacy of neuro-mobilization procedures. (Coppieters, M. W., and Butler D., S., 2007). During the movements, the central and peripheral nervous system must perform three functions: resistance to tension, sliding in its shell and be compressible. These functions, during the movement are manifested in the form of: neuro-dynamic tension, neuro-dynamic sliding and compression. The techniques used in neuro-dynamic therapy are: opening, closing, sliding and tensioning techniques with a single end, sliding and tensioning with two ends. (Basson A, et al., 2017).
Through this research we want to highlight the role of mobilizing the neuroimmune system through specific neuro-dynamic techniques in treating the symptoms of lumbosciatica. The hypothesis from which we started - it is assumed that the introduction of neuro-dynamic techniques in the recovery program of patients with lumbosciatica, will effectively influence the functional parameters compared to the classic recovery program. In this study we selected 14 subjects, divided into two groups of 7. Group 1 - experimental which benefited from neuro-dynamic exercises (table no. 1) and group 2 being - control, which benefited from classical physiotherapy (table no. 2). The research took place between June 2020 and May 2021, at a private recovery clinic, the program being staged in two stages. The first stage was 8 sessions, with the following objectives: decrease pain and inflammation, restore muscle balance and regain muscle elasticity. The second stage of 4 sessions, in which the aim was: toning the muscles, reforming the lumbar lordosis and reeducating proprioception. The duration of the recovery sessions was 30 minutes and consisted of: opening or closing techniques depending on the preferred direction of flexion or extension, sliding and tensioning with one end, sliding and tensioning with two ends.
For evaluation we used: Lasegue Test (SLR) (Balint, T., 2007), SLUMP Test (Johnson, E. K. & Chiarello, C.M.1997, p. 313), Scala VAS (0-10) and Roland‐Morris Disability Questionnaire (Roland, M., Fairbank, 2000, p.3115). In table no. 3 and 4, the initial, intermediate and final values are presented in the tests performed, both in the experimental group and in the control group.
Table 1: Experimental group
| No. | Subject | Age | Sex | Diagnosis |
| 1. | S1 | 39 | M | Low back pain with irradiation on the lower left limb |
| 2. | S2 | 55 | F | Left lumbosciatica |
| 3. | S3 | 37 | M | Algo-paresthetic right hyperalgesic lumbosciatica Disc herniation L5-S1 under observation |
| 4. | S4 | 67 | M | L5-S1 root syndrome |
| 5. | S5 | 38 | M | Algo-paresthetic right hyperalgesic lumbosciatica Disc herniation L5-S1 under observation |
| 6. | S6 | 61 | F | L5-S1 root syndrome |
| 7. | S7 | 46 | F | L5-S1 right herniated disc under observation |
Table 2: Control group
| No. | Subject | Age | Sex | Diagnosis |
| 1. | S1 | 55 | M | Low back pain with irradiation on the left lower limb |
| 2. | S2 | 37 | F | L4-L5 disc herniation under observation |
| 3. | S3 | 66 | F | Left L5-S1 radiculopathy |
| 4. | S4 | 53 | M | Low back pain with irradiation on the right lower limb |
| 5. | S5 | 71 | F | L5-S1 root syndrome |
| 6. | S6 | 49 | F | Operated lumbar disc herniation, left recurrent L4 vertebro-radicular syndrome |
| 7. | S7 | 36 | M | Low back pain with irradiation on the right lower limb |
Table 3: Subjects of the experimental group and values of initial and final tests
Nr. Crt. | S | Vas I | Vas Int | Vas F | Las I | Las Int | Las F | Slu I | Slu Int | Slu F | RMDQ I | RMDQ Int | RMDQ Fin |
| 1 | S1 | 7 | 3 | 2 | + | - | - | + | - | - | 8 | 4 | 2 |
| 2 | S2 | 5 | 3 | 2 | + | - | - | + | - | - | 6 | 3 | 1 |
| 3 | S3 | 8 | 5 | 2 | + | + | - | + | + | - | 9 | 5 | 2 |
| 4 | S4 | 9 | 8 | 3 | ++ | + | + | ++ | + | + | 13 | 8 | 3 |
| 5 | S5 | 6 | 4 | 1 | + | - | - | + | - | - | 5 | 2 | 0 |
| 6 | S6 | 9 | 6 | 4 | ++ | + | - | ++ | + | + | 12 | 7 | 2 |
| 7 | S7 | 7 | 3 | 2 | + | - | - | + | - | - | 7 | 4 | 1 |
VAS, visual analog scale; RMDQ, Roland‐Morris Disability Questionnaire, Lasegue, straight leg raise; (Legend: 0 (-) negative test (over 700), 1 (+) positive test (between 350-700), 2 (++) positive test (under 350)); SLUMP test (Legend: 0 (-) negative test (full knee extension + dorsal ankle flexion), 1 (+) positive test (incomplete knee extension pain), 2 (++) positive test (head flexion pain).
Table 4: Control group
Nr. Crt. | S | Vas I | Vas Int | Vas F | Las I | Las Int | Las F | Slu I | Slu Int | Slu F | RMDQ I | RMDQ Int | RMDQ Fin |
| 1 | S1 | 8 | 5 | 2 | + | - | - | + | + | - | 9 | 6 | 3 |
| 2 | S2 | 8 | 6 | 3 | + | + | - | + | + | - | 10 | 8 | 5 |
| 3 | S3 | 8 | 7 | 4 | + | + | + | + | + | + | 11 | 8 | 5 |
| 4 | S4 | 6 | 4 | 1 | + | - | - | + | - | - | 7 | 5 | 3 |
| 5 | S5 | 7 | 5 | 2 | + | + | - | + | + | - | 9 | 6 | 4 |
| 6 | S6 | 7 | 4 | 3 | + | + | - | + | + | - | 9 | 5 | 3 |
| 7 | S7 | 8 | 6 | 3 | + | + | - | + | + | - | 10 | 7 | 5 |
VAS, visual analog scale; RMDQ, Roland‐Morris Disability Questionnaire, Lasegue, straight leg raise; (Legend: 0 (-) negative test (over 700), 1 (+) positive test (between 350-700), 2 (++) positive test (under 350)); SLUMP test (Legend: 0 (-) negative test (full knee extension + dorsal ankle flexion), 1 (+) positive test (incomplete knee extension pain), 2 (++) positive test (head flexion pain).
In order to highlight the efficiency of neuro-dynamic techniques compared to classical recovery, I will further present graphically the values obtained from the tests used.
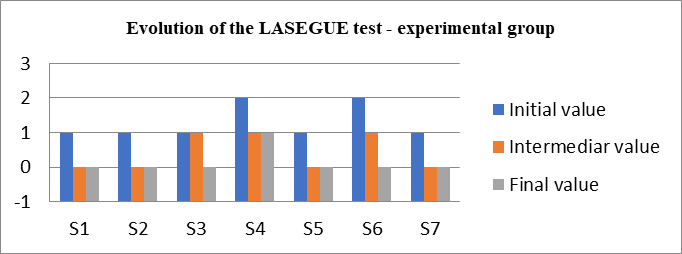
Chart 1: The evolution of pain according to the LASEGUE test in the experimental group.
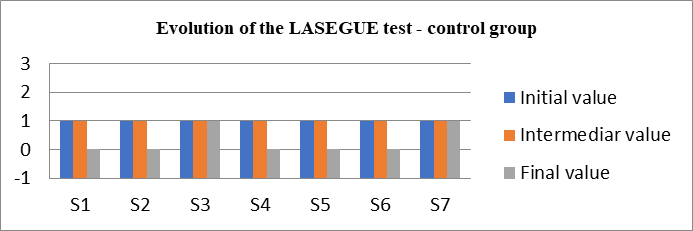
Chart 2: The evolution of pain according to the LASEGUE test in the control group.
As shown in chart no. 1 and 2, in the Lasegue test 4 of the subjects of the experimental group at the intermediate test showed negative values (without pain) of the test and in the control group only 2 subjects had the negative test, which represents a faster decrease of sciatic nerve inflammation for subjects in whom neuro-dynamic techniques were used, given that 2 of the subjects (S4, S6) initially had a limitation of nerve extension below 35 degrees (chart no. 1 and 2).
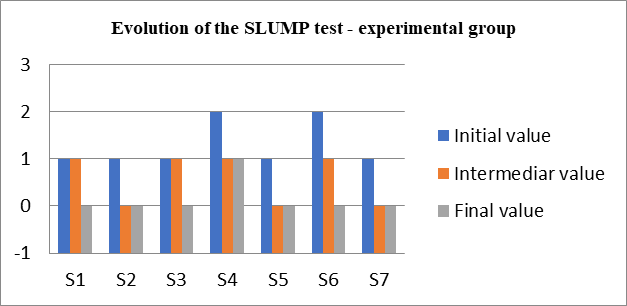
Chart 3: The evolution of pain according to the SLUMP test in the experimental group.
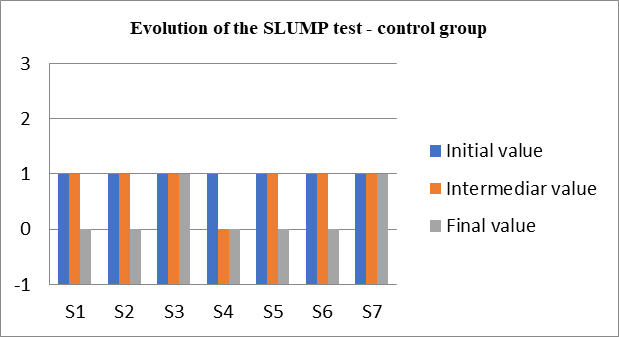
Chart 4: The evolution of pain according to the SLUMP test in the control group.
Regarding the values of the SLUMP test, it is found that the same 4 subjects from the experimental group obtained negative test values at the intermediate evaluation (after 8 sessions), while in the control group, only one subject obtained negative values.
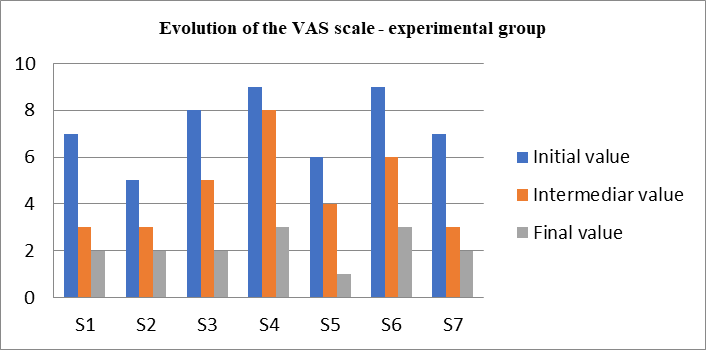
Chart 5: The evolution of pain according to the VAS Scale in the experimental group.
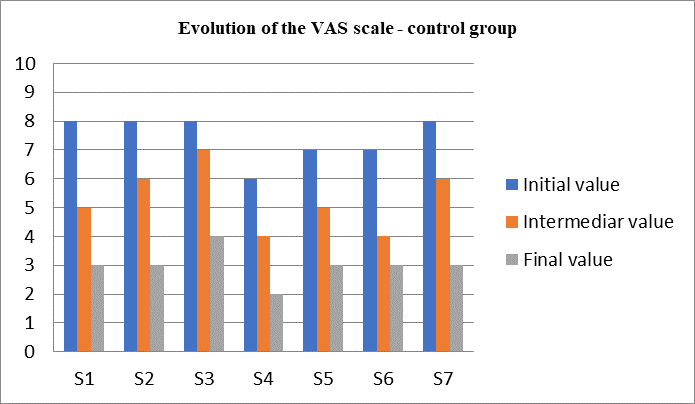
Chart 6: The evolution of pain according to the VAS Scale in the control group.
Regarding the assessment of pain according to the VAS scale, in the experimental group, we observe a decrease in pain to the value of 2 and 1, while in the control group the pain reached values of 3 and 4 at the end of the 12 sessions (graph 5, 6) .e SLUMP test values it is found that the same 4 subjects from the experimental group obtained negative test values at the intermediate evaluation (after 8 sessions), while in the control group, only one subject obtained negative values.
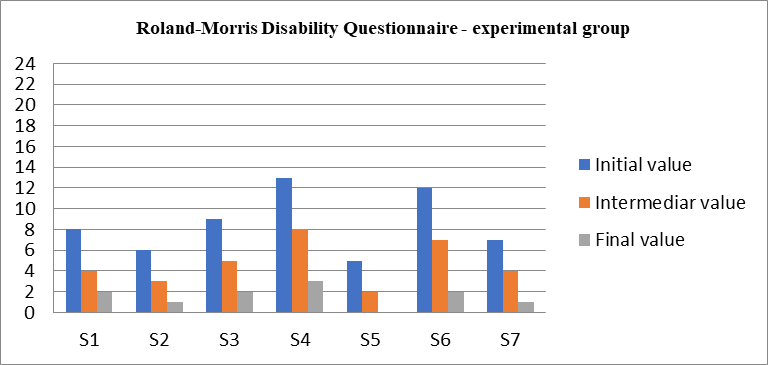
Chart 7: The evolution of pain according to the Roland‐Morris Disability Questionnaire in the experimental group.
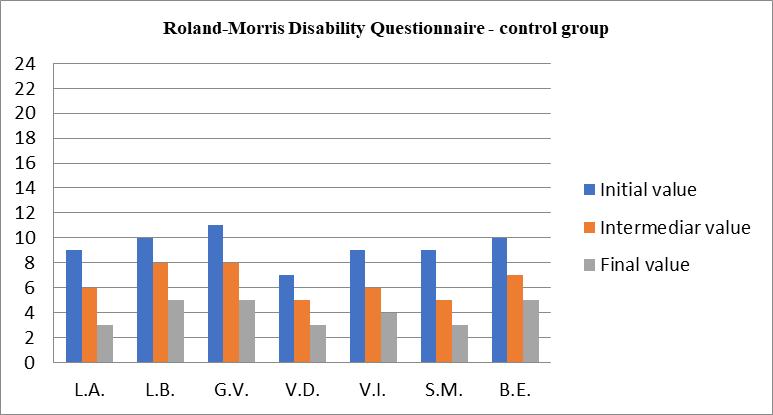
Chart 8: The evolution of pain according to the Roland‐Morris Disability Questionnaire in the control group.
In the Roland-Morris disability questionnaire we notice that the patients of the experimental group recorded an average score of 8.57 initial, 4.42 intermediate and 1.57 final and the subjects of the control group, an average score of 9.28 initial, 6.42 intermediate and 4 at the end. Thus, the average difference of 2.43 points at the end in favor of the experimental group, represents a higher mobility in daily activities.
Following this study on the effectiveness of neuro-dynamic techniques in the recovery of patients with lumbosciatica, the hypothesis was confirmed, in the sense of pain relief after 8 therapy sessions, in the experimental group, aspect highlighted by the test Lasegue, Slump and the VAS scale, as well as the development of daily activities with greater mobility and without the presence of pain in daily activities, an aspect supported by Roland-Moris Disability Questionnaire, in which the final score reached a value between 1- 2 at the end, compared to 8 - 9 initially.
It is important to emphasize that the use of these techniques requires a knowledge of the pathology, a correct diagnosis, informing patients about the techniques to be performed and the importance of understanding their effect, but also the therapist's ability to apply and individualize them. The effectiveness of these techniques is found in relieving pain and maintaining long-term effects, as patients understand the importance of following the rules of secondary prophylaxis to prevent the disease from getting worse.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
