
Case Report | DOI: https://doi.org/10.31579/2690-8794/049
1 Division of Gastroenterology and Therapeutic Endoscopy Unit, Medica Sur Clinic &Foundation, Mexico City.
2 Division of Interventional Radiology Unit, Medica Sur Clinic & Foundation, Mexico City.
*Corresponding Author: Lopez-Mendez YI. Gastroenterology and Therapeutic Endoscopy Unit, Medica Sur Clinic & Foundation. Puente de Piedra 150, Toriello Guerra, Tlalpan, ZC 14050, Mexico City.
Citation: Jorge A. Matus J, Adolfo L. Rodriguez and Ivan L. Mendez (2020) Rendezvous for afferent limb síndrome J. Clical Medical Reviews and Reports, 2(9); DOI: 10.31579/2690-8794/049
Copyright: © 2020 Farla Jean-Louis, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 November 2020 | Accepted: 20 November 2020 | Published: 10 December 2020
Keywords: ERCP; pancreatic oduodenectomy; cholangitis; stent
Endoscopic retrograde cholangiopancreatography (ERCP) in patients with surgical alterations in the normal biliary anatomy is technically challenging. We describe the case of a 73-year-old patient with an afferent limb syndrome secondary to a Whipple procedure for pancreatic cancer, in which a percutaneous rendezvous technique assisted in the endoscopic metallic stent placement with favorable outcome.
For patients with surgical alterations in the normal biliary anatomy (Whipple procedure), an endoscopic retrograde cholangiopancreatography (ERCP) in is technically challenging [1]. The afferent limb syndrome has been described in patients with biliodigestive derivative surgery in which the afferent limb is unable to empty its contents due to a mechanical problem [2]. In patients with afferent limb syndrome, the access to the afferent limb depends in the different type of reconstruction, the cannulation of the papilla is difficult due to the reversed orientation, and to performance of the therapeutic interventions often require uncommon endoscopic accessories [3] and the endoscopists skills in order to be successful. There is no gold- standard for endoscopic management of afferent limb syndrome, and alternative access points should be considered, like the rendezvous procedure (French for “encounter”), among others. We describe a successful case of afferent limb syndrome managed with a rendezvous and endoscopically stent placement.
A 73-year-old male was diagnosed with pancreatic adenocarcinoma underwent modified Whipple procedure (pylorus-preserving) three years earlier. Two months before presentation patient developed intermittent jaundice, low grade fever and pain in the upper right quadrant of the abdomen. Respect to biochemical data total bilirubin was 11.7 mg/dL (normal range 0.4-1.5 mg/dL), alkaline phosphatase was 800 IU/L (normal range 32-91 IU/L), and gamma-glutamyl transpeptidase was 550 IU/L (normal range 7-50 IU/L). An abdominal ultrasound reported dilatation of the biliary tree (common bile duct 8.5 mm in diameter). Ascending cholangitis secondary to an afferent limb syndrome was suspect and the patient underwent an emergency ERCP. Access to the biliary tree was impossible due to post-surgical alterations in anatomy.
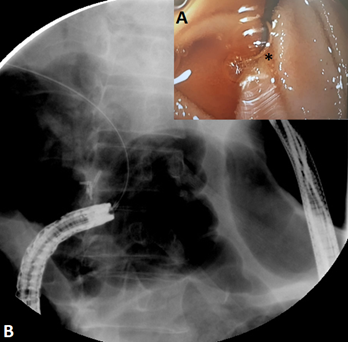
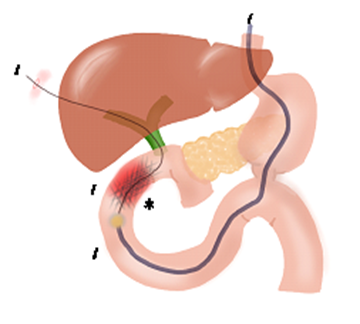
First, a colonoscope was passed up to the choledochojejunostomy, which was found kinked and angulated. Therefore, the colonoscope was withdrew and an enteroscope was passed until the kinked choledochojejunostomy. Second, a hydrophilic guidewire was introduced percutaneously into the biliary tree under transabdominal ultrasound assistance to access the afferent limb (Figure 1), and the guidewire was recovered with the enteroscope (Figure 2). Third, the enteroscope holding the guidewire was withdrew and interchanged into a stent-loaded colonoscope. Finally, the colonoscope holding the guidewire was introduced and an enteral uncovered self-expandable metal stent (22mm x 60mm) was successfully deployed in the site of the obstruction (Figure 3). The schematic representation of the technique is described inf Figure 4. The patient’s evolution was satisfactory and was discharged 48 hours after the procedure.


Afferent limb syndrome is a rare complication after Whipple procedure, resulting in a high risk of necrosis, perforation or ascending cholangitis [2]. In a retrospective case series, [4] reported in patients with 2 years or more of follow up after pancreaticoduodenectomy for pancreatic cancer, that 13% (24 patients of 186) developed afferent limb syndrome. Median time to diagnosis was 1.2 years and obstruction was primarily caused by recurrent pancreatic cancer; interestingly, 54% (13 of 24 patients) were found with stricturing of the afferent limb and 29% (7 of 24 patients) with angulation of a fixed afferent limb, as in our patient. Chahal et al. [5] reported that the success rate of ERCP was 51% (45 of 88 procedures) and it was more likely to be successful for biliary indications (37 of 44 procedures, 84%) than for pancreatic indications (3 of 37 procedures, 8%).
Depending on the site of the obstruction, endoscopic management should be the first treatment option. Many endoscopic techniques has been described to facilitate access to the afferent limb and biliary tree [1, 3, 6, 7], however, each technique must be individualized according to the cause of the afferent limb syndrome [2, 8, 9].
In this case, a rendezvous procedure was performed successfully with enteral stent placement. Therefore, there is no gold-standard procedure and the endoscopist’s and radiologist’s skills are the cornerstone to minimize the morbidity in these patients.
Jimenez-Pavon J, MD MSc for the graphic design of the illustrations.
The authors declare non conflict of interest.
All the authors contributed equally for this work
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
