
Research Article | DOI: https://doi.org/10.31579/2692-9392/160
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Lecturer of Obstetrics & Gynecology Faculty of Medicine, Beni-Suef University.
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Fatima Hosny Abd-ELhakam, Rasha El-Syed Ebrahim, Momen Zakria Mohammed and Hanan Elzeblawy Hassan, (2022), Relationship between Socio Demographic Data and Female Genital Mutilation. Archives of Medical Case Reports and Case Study, 6(5); DOI:10.31579/2692-9392/160
Copyright: © 2022, Hanan Elzeblawy Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 November 2022 | Accepted: 12 December 2022 | Published: 22 December 2022
Keywords: relationship; socio demographic data; female genital mutilation
Background: The World Health Organization and the United Nations Children's Fund and the United Nations Population Fund released the first joint statement directly addressing Fmale Genital Mutilation.
Aim: Assess Relationship between Socio Demographic Data and Female Genital Mutilation at Beni-Suef. Subject & Methods: A descriptive cross-sectional study was used. The study population consisted of 2837 females in family health centers (FHCs) in different sitting at Beni-Suef. Α Structured Interviewing Questionnaire sheet was used to collect data.
Results: The mean age of the studied participants was 22.6±5. The prevalence of FGM/C was 71.4%. Significant associations between FGM/C and participants' residence, level of education, marital status, religion, and parents' education (p≤0.001) were found.
Conclusion & Recommendations: There is an association between socio demographic data and Female Genital Mutilation at Beni-Suef. Development of an educational program for rural dwellers about FGM is required to increase their awareness.
Female genital mutilation (FGM/C) is a crucial global issue of interest attracting policy-makers attention attributed to its direct effect on women's health and representing a particular of gender-based violence (Sabry, et al., 2020). Over the past decades, the problem of FGM, which previously was referred to as female circumcision, has attracted the eye of researchers because it is one of the worst sorts of violations against females (Joseph, 2014).
The World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) and the United Nations Population Fund released the first joint statement directly addressing FGM/C in 1997. (UNFPA, 2019). Since then, the international response has picked up speed (McCauley, 2019).
Although the procedure is known as clitoridectomy in the nations where it is performed, its unpleasant physical and psychological ramifications have led to the use of the Latin term "mutylatio" in medical literature, which means "to maim, to chop off (mutilation)."(Birge, et al., 2019). The term female circumcision should be avoided since it draws a parallel with male circumcision and, as a result, creates confusion between these two distinct practices (UNICEF, 2016).
In the Arab world, FGM/C may be a contentious topic, and there's no consensus on whether it's an Islamic requirement or an ethnic tradition. However, the influential Egyptian Muslim institution Dar Al-Ifta Al- Misriyyah recently confirmed during a press statement that FGM/C is religiously forbidden as a result of its negative impact on physical and mental well-being. Sheikh of Al-Azhar reconsiders unreliable fatwas released by some members of the school of Al-Azhar University (Egypt) who claim FGM/C may be a religious necessity supported by weak Hadith (Prophet Mohammad‟s teachings) through the subsequent statement: “This act has no religious origin; it only dates back to inherited traditions and customs and therefore the biggest evidence for not being a religious duty for girls is that the Prophet Muhammad had not circumcised his daughters.” Nevertheless, this practice is widely prevalent in many Muslim countries, especially Sudan, Iran, and Egypt (Al Awar, et al., 2020).
The present study was carried find out about FGM in Beni-Suef Governorate through:
2.1. Research Questions
3.1. Research Design: A Descriptive Cross-sectional study was used
3.2. Subjects & Setting:
3.2.1. Setting: The family health centers (FHCs) in different sitting at Beni-Suef Governorate.
3.2.2. Sample:
3.2.2.1. Sample Type:
A Convenient sample was used. The study sample was selected according to the following Inclusion criteria: 18-60 years old women. Can read and writes
3.2.2.2. Sample size:
The study population consisted of all circumcised females (2837) who were accepted to participate in the study at the time of data collection (A period of six months from the start of data collection) and will be included in the study.
3.2.3. Tools of Data Collection:
A pre-designed structured questionnaire was used to collect data. Data were collected through personal interviews. The questionnaire is divided into three sections:
Section I: А Structured Interviewing Questionnaire sheet which includes the following parts: age, residence, level of education, marital status, occupation and experience with mutilation, etc……
Section II: Prevalence of Female Genital Mutilation (FGM/C) among total participant women
Section III: Relationship between Socio Demographic Data and Female Genital Mutilation among studied participants
3.2.4. Validity of the Tool
Five experts reviewed the content validity of the tool from maternity and gynecological nursing professors, obstetric and gynecological medical professors and mental health nursing professors.
3.2.5. Ethical Considerations & Administrative Considerations:
Researchers took approval from settings directors before starting the research in order to allow them to take the survey sample. Written letters, including the aim of the study was issued from the dean of the faculty of nursing, Beni-Suef University, to the directorate of the MCH centers in Beni-Suef city to obtain permission to collect the research sample from MCHs under their directorate. Consent from every woman before the beginning of the interview was taken. Explanation of the study's aim was done for women to gain their permission to participate. Every woman participating in the study was assured clearly about confidentiality of the information gathered, and its use only for this study.
3.2.6. Pilot study
It is approximately 10% of the study sample. Woman's abilities to participate in filling questionnaire were assessed. The pilot settings, selected in this study were inclusive in the original study subject, but the pilot sample was excluded from the main one in order to avoid contamination of the study sample. The pilot study assessed clarity of language, applicability of items, and time consumed for filling in the tools' items. According to the results of the pilot study, modifications were made on the questionnaires.
3.2.7 Field Work
Data were gathered over six months beginning in November 2021 and ending in April 2022. The researcher was present at the previously mentioned location until the entire sample size was gathered. Before data collection, the researcher introduced herself to the women and explained the purpose of the study.
3.2.8. Statistical Analysis
All data were collected, tabulated and statistically analyzed using IBM SPSS 25. Data was supplied, and appropriate analysis was performed for each parameter based on the type of data obtained.
3.2.8.1. Descriptive Statistics data were expressed as:
3.2.8.2. Analytical Statistics:
3.2.8.3. Graphical presentation:
Table (1) showed that the mean age of the studied participants was 22.6±5, most of them were rural residents (70.4%), 90.2% were highly educated, 57.5% were single, 96.8% were Muslims, and most of their mothers were educated (72.8%), and most of their fathers were educated (83.2%). About two-thirds of the participants were a student (65.4%).
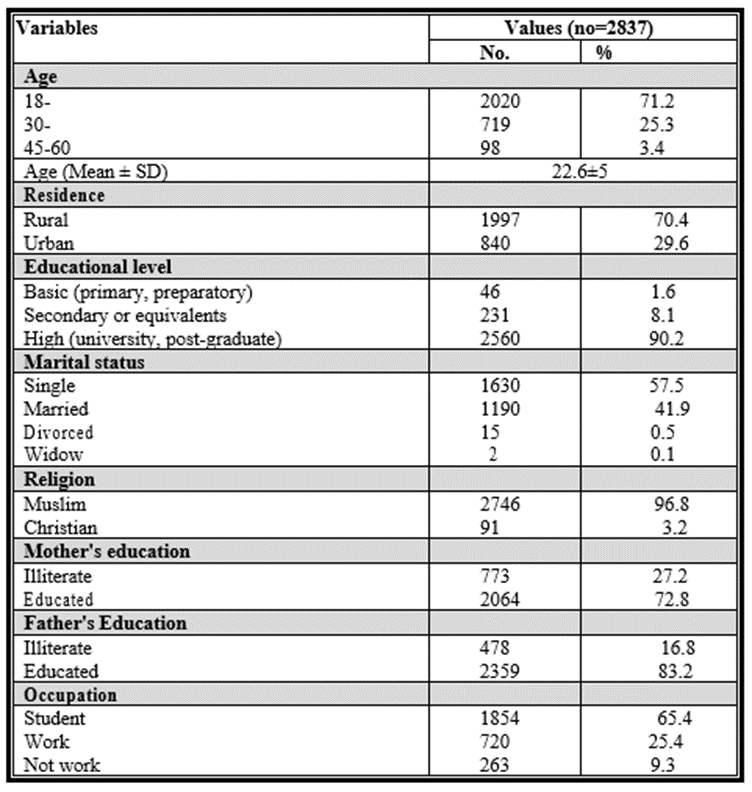
Table 1: Socio-Demographic & Personal Characteristics of the Studied Participants
Figure (1) showed that the prevalence of FGM/C among total participants (2837) at Beni-Suef was 71.4%.
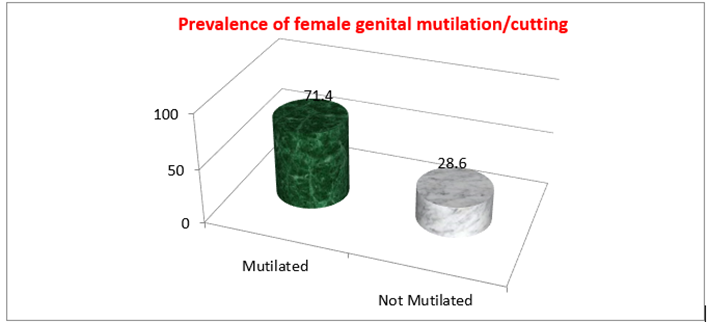
Figure 1: Prevalence of female genital mutilation/cutting.
Figure (2): presented the relationship between residence of studied participants and circumcision. It showed that there was a significant association between FGM/C and participants' residence (p≤0.001). Circumcision were more prevalent (81.3%) among rural dwellers than urban (18.7%) ones.
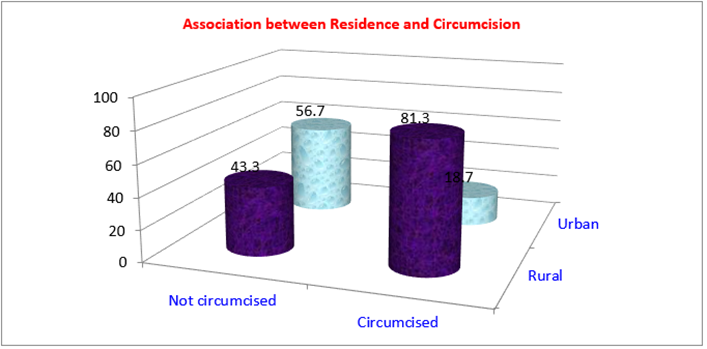
Figure 3: Association between Educational level of studied participants and Circumcision
VFigure (4): presented the relationship between marital status of studied participants and circumcision. It presented that there was a significant association between marital status and circumcision(p≤0.001). Circumcision was more prevalent (54.9%) among single females than other ones.
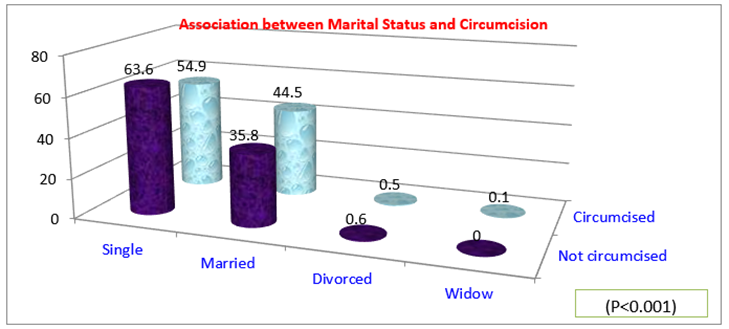
Figure 4: Association between Marital Status of studied participants and Circumcision
Figure (5): presented the relationship between religion of studied participants and circumcision. It showed that there was No significant association between religion and circumcision (p>0.05)
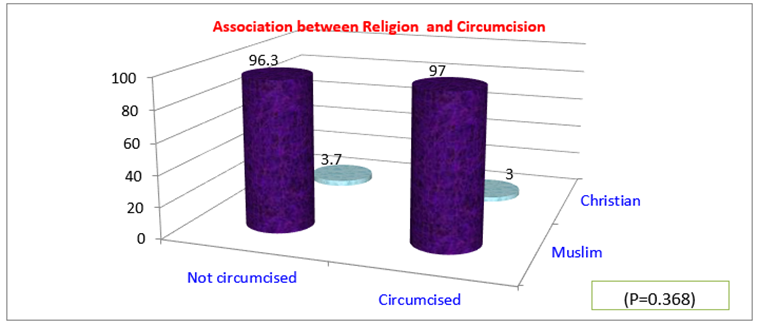
Figure 5: Association between Religion of studied participants and Circumcision
Figure (6): presented the relationship between parents' education and circumcision. It showed that there was a significant association between mothers' education and circumcision (p≤0.001). Non circumcised participants were more prevalent (82.2%) among those whose mothers were educated than illiterate ones (17.8%).
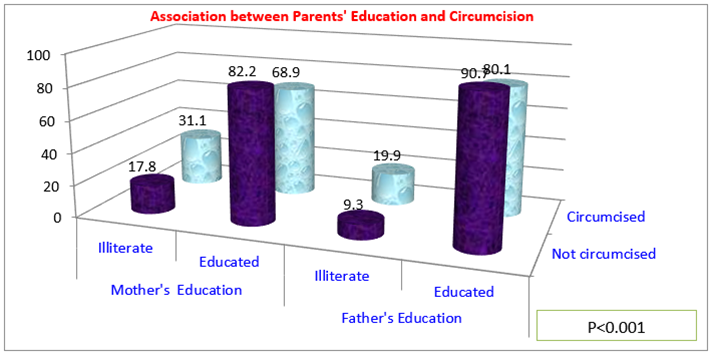
Figure 6: Association between Parents'' Education and Circumcision.
There is no concrete evidence of where FGM was first beginning to be practiced, but some studies suggest it'd are first started in ancient Egypt and then spread to different parts of the world at different times (Abdelhafeez, et al.,2020).
In the current study, the mean age at the time of mutilation was 12.5±2.5 years. The minority of those who had been mutilated was over 15 years, compared to majority of those who had been mutilated between the ages of 10 and 15, and near to tenth of those who had been mutilated between the ages of 5-10. Only zero point one of the females under the age of five (2-3 years) have female genital mutilation. It is worth mentioning that 4 of the participants were mutilated after their marriage their ages ranged from 23-28 years. The mean age of FGM/C discovered in this study was equal to that of FGM/C reported among schoolgirls in Beni-Suef which was (12- 16) years (Khamis, et al., 2019). On the other hand, it was lower than the mean age FGM/C discovered among Beni-Suef university students which was (Arafa, et al., 2018).
According to the Survey of young people in Egypt (SYPE), mutilation was performed at a younger age in Upper Egypt compared to the urban governorates and Lower Egyptfor females (Roushdy & Sieverding, 2015). However, data demonstrates that most Egyptian females are mutilated before puberty (El-Gibaly et al., 2002).
The results of the present study reveal a signification relationship between mutilation and residences, level of education, and marital status. There was a significant association between, rural residence, lower mother and father education, marriage, and the presence of mutilation. This conclusion, which highlights the importance of education and family educational background in decision-making about FGM, was previously documented by (Kandala, et al., 2018)
The prevalence of FGM/C in the present study was higher in rural areas. It is similar to the results of EHIS which reported that the highest prevalence of FGM/C was in rural areas (MOHP, et al., 2015). Also comparable to a study done in Beni-Suef, females from rural regions are far more likely to be mutilated than those from urban ones (Ali, et al., 2018).
The prevalence of FGM/C was found to be lowest among highly educated females, most of their mothers were educated, and most of their fathers were educated. This finding was at odds with the Survey of young people in Egypt, SYPE findings, and the EHIS, which indicated that the prevalence of FGM/C reduced as educational attainment rose.
The findings of the current study agreed with those of a study carried out in Alexandria, which revealed that mutilated females were more likely to be illiterate or have limited reading and writing skills than non-mutilated females (Mady, 2017). The present study shows that there was a significant association between rural residence, lower mother and father education, marriage, and the presence of circumcision. This outcome was consistent with a UAE study that found a significant correlation between education level and mutilation (Al Awar, et al., 2020)
The mean age of the studied participants was 22.6±5. The prevalence of FGM/C was 71.4%. Significant associations between FGM/C and participants' residence, level of education, marital status, religion, and parents' education (p≤0.001) were found. There is an association between socio demographic data and Female Genital Mutilation at Beni-Suef. Development of an educational program for rural dwellers about FGM is required to increase their awareness.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
