
Research Article | DOI: https://doi.org/10.31579/2768-2757/178
Associate Professor, International Institute of Health Sciences.
*Corresponding Author: Md Shafiullah Prodhania, Associate Professor, International Institute of Health Sciences.
Citation: Md Shafiullah Prodhania , (2025), Rehabilitation Among Post-Stroke Patients, Journal of Clinical Surgery and Research, 6(5); DOI:10.31579/2768-2757/178
Copyright: © 2025, Md Shafiullah Prodhania. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 May 2025 | Accepted: 21 April 2025 | Published: 02 June 2025
Keywords: rehabilitation; post-stroke patients
Stroke is a fatal disease; it brings either death or disability. After emergency management stroke patients need rehabilitation to back near normal life and make his or her life independent as much as possible. The study focuses on the physical rehabilitation status among the post-stroke patients. A cross sectional study was conducted among conveniently selected 150 patients irrespective of age and gender attending treatment in Bangladesh Medical University. A well designed structured standard questionnaire was used to collect required data from the study subjects. SPSS version 20 was used to analyze data. Average age of the respondents was 53.43±12.87 years. Male was quite double than female. About 31.3% respondents completed primary level education. More than half of the respondents came from upper middle-income group. Three-fourth of the respondents (76%) suffered from hemorrhagic stroke and one-fourth (24%) ischemic stroke. About 97.30% of the patients suffered from hemiplegia. About 96.70% patients received both medication and rehabilitation. Almost all of the patients were receiving physiotherapy. Active assisted exercise as means of rehabilitation was prominent (88%) and passive exercise was provided among 12% patients. Statistical significant association was found between gender and type of stroke (p=0.001<0.05). Statistical significant association was found between family type and type of stroke (p=0.004<0.05). Statistical significant association was found between income group and type of stroke (p=0.001<0.05). More large scale study can be constituted to get more precise result. Early rehabilitation is required.
Stroke is widely recognized as a major cause of disability among adults and is the most common cause of dependence in activities of daily living among the elderly. Approximately 90% of stroke survivors have permanent neurological deficits. Two thirds of stroke survivors require rehabilitation, and 50% do not regain their independence.1 Disability caused by stroke has a massive impact on the patient, with social consequences and physical consequences of stroke being equally devastating.2 Recent studies suggest that between one-fourth and one-third of stroke patients experience persistent dependency in one or more activities of daily living by 6 months after their strokes. Stroke survivors are often greatly challenged by post stroke depression, which can lengthen rehabilitation and recovery time considerably. Apart from having a deep impact on the survivors themselves, post-stroke depression also affects family and friends.3 However, patients with a history of stroke are at risk of a subsequent event of around 10% in the first year and 5% per year thereafter.4 The primary goals of stroke rehabilitation are to regain independence and improve quality of life by minimizing the limitations of activities of daily living.5 Structured stroke care should consider the early timing of rehabilitation, a qualified rehabilitation team, and duration of rehabilitation, which are important elements that have been distinguished as advancing better general outcomes for patients with stroke.6 Evidence from systematic reviews support that organized stroke rehabilitation units, and more prominent intensities of rehabilitation are associated with enhanced improved functional outcomes compared with mixed rehabilitation units, general units, and mobile stroke units.7 This suggests that neurological rehabilitation alone does not represent the level of useful changes observed in stroke rehabilitation. Rehabilitation services regardless of the setting are found to be associated with better functional outcomes. There is strong evidence supporting the beneficial effects of early admission to stroke rehabilitation units within 24-48 hours after stroke, to enhance functional outcomes. In Bangladesh no such study was done yet.
A cross-cut study was conducted to identify the status of rehabilitation among the post-stroke patients. Considering time period and resource availability, cross-sectional analytical study design was most feasible for this study. This study was conducted in BMU. This area was selected for data collection and get adequate sample for this study. As no sampling frame is available in the community level, non-probability convenient sampling was used to collect study subjects. Data were collected through questionnaire by personal interview. Face to face interview was carried out. Health status was determined by taking history and conducting physical examination. Medical records were checked if available. After administering questionnaire, data were checked for consistency. Individual sheet was checked and cleaned to avoid any error. Data were categorized and coded during entry into the SPSS software. Collected data were analyzed by computer technology SPSS version 22.0. Collected information was presented in the form of tables and graphs. Descriptive statistics (mean, SD, frequency, percentage) and inferential statistics (Chi-square) were used.
1. Age group of the study subjects
| Age in year | Frequency | Percentage |
| Mean±SD | 53.43±12.87 | |
| 21-35 | 18 | 12 |
| 36-50 | 42 | 28 |
| 51-65 | 63 | 42 |
| 66-85 | 27 | 18 |
| Total | 150 | 100.0 |
Average age of the study subjects was 53.43±12.87 years. Majority of the respondents (42%) belonged to 51-65 years followed by 28% from 36-50 years, 18% from 66-85 years and 12% from 21-35 years.
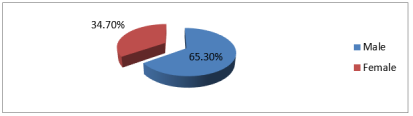
Figure 1: Gender distribution
Male was quite double (65.30%) than female (34.70%).
| Family income | Frequency | Percentage |
| Mean±SD | 34273.33±18821.98 | |
| Low-income (≤$75.41 or BDT ≤5360) | 3 | 2.0 |
| Lower middle-income ($75.5 - $299.58 or BDT 5361-21270) | 49 | 32.7 |
| Upper middle-income ($299.68 - $926.25 or BDT 21271-65761) | 88 | 58.7 |
| Upper income (>$926.25 or BDT 65761) | 10 | 6.7 |
| Total | 150 | 100 |
Table 2: Monthly family income of the study subjects
Average monthly family income among was 34273.33±18821.98 BDT. More than half of the respondents (58.7%) came from upper middle-income ($299.68 - $926.25 or BDT 21271-65761) group followed by 32.7% from lower middle-income ($75.5 - $299.58 or BDT 5361-21270) and 6.7% from upper income group (The Daily Star, 2011).
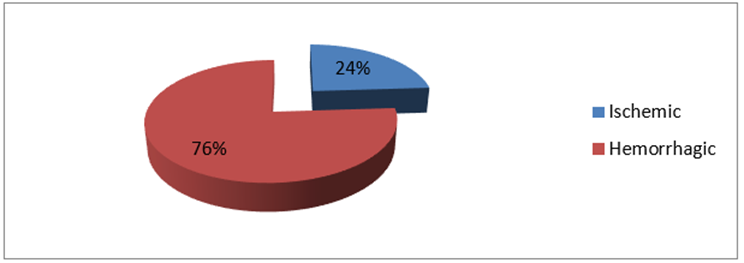
Figure 2: Type of stroke
Three-fourth of the respondents (76%) suffered from hemorrhagic stroke and one-forth (24%) ischemic stroke.
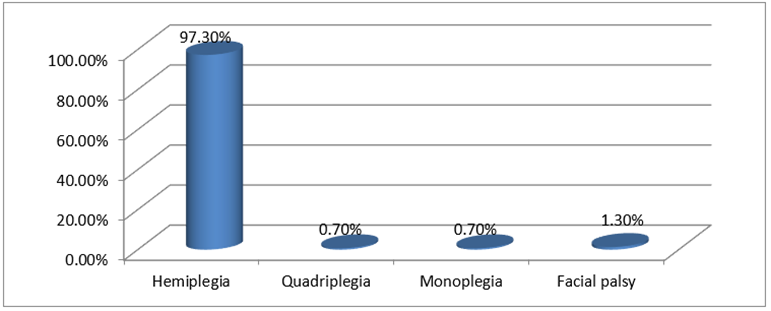
Figure 3: Type of disability
About 97.30% of the patients suffered from hemiplegia.
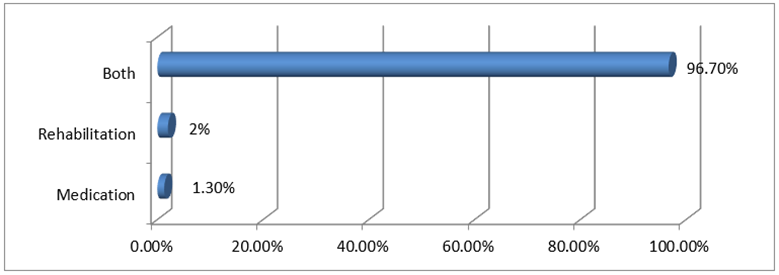
Figure 4: Type of treatment receiving
About 96.70% patients received both medication and rehabilitation.
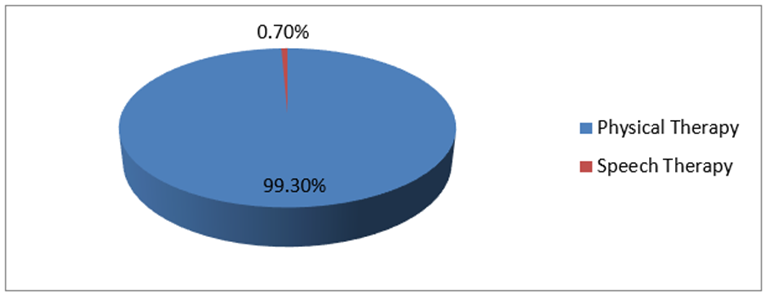
Figure 5: Type of rehabilitation receiving.
Almost all of the patients were receiving physiotherapy.
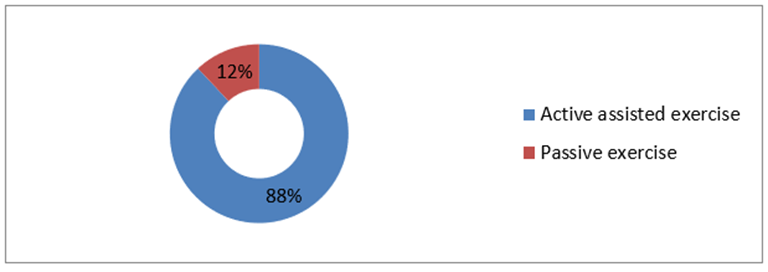
Figure 6: Means of rehabilitation.
Active assisted exercise as means of rehabilitation was prominent (88%) and passive exercise was provided among 12% patients.
| Age group | Type of stroke | Total | χ2
| p-value
| |
| Ischemic | Hemorrhagic | ||||
| 21-35 | 7(4.7) | 11(7.3) | 18(12.0) |
6.789 |
0.079 |
| 36-50 | 7(4.7) | 35(23.3) | 42(28.0) | ||
| 51-65 | 12(8.0) | 51(34.0) | 63(42.0) | ||
| 66-85 | 10(6.7) | 17(11.3) | 27(18.0) | ||
| Total | 36(24.0) | 114(76.0) | 150(100.0) | ||
Table 3: Association between age group and type of stroke
No statistical significant association was found between age group and type of stroke (p=0.079>0.05).
| Gender | Type of stroke | Total | χ2
| p-value
| |
| Ischemic | Hemorrhagic | ||||
| Male | 9(6.0) | 89(59.3) | 98(65.3) |
34.023 |
0.001 |
| Female | 27(18.0) | 25(16.7) | 52(34.7) | ||
| Total | 36(24.0) | 114(76.0) | 150(100.0) | ||
Table 3: Association between gender and type of stroke
Statistically significant association was found between gender and type of stroke (p=0.001<;0.05).
| Family type | Type of stroke | Total | χ2
| p-value
| |
| Ischemic | Hemorrhagic | ||||
| Joint | 18(12.0) | 28(18.7) | 46(30.7) |
8.327 |
0.004 |
| Nuclear | 18(12.0) | 86(57.3) | 104(69.3) | ||
| Total | 36(24.0) | 114(76.0) | 150(100.0) | ||
Table 4: Association between family type and type of stroke
Statistically significant association was found between family type and type of stroke (p=0.004<;0.05).
| Income group | Type of stroke | Total | χ2
| p-value
| |
| Ischemic | Hemorrhagic | ||||
| ≤5360 | 0(0.0) | 3(2.0) | 3(2.00 |
26.844 |
0.001 |
| 5361-21270 | 0(0.0) | 49(32.7) | 49(32.7) | ||
| 21271-65761 | 34(22.7) | 54(36.0) | 88(58.7) | ||
| >65761 | 2(1.3) | 8(5.3) | 10(6.7) | ||
| Total | 36(24.0) | 114(76.0) | 150(100.0) | ||
Table 5: Association between income and type of stroke
Statistical significant association was found between income group and type of stroke (p=0.001<;0.05).
Stroke is the third commonest cause of death worldwide and fourth leading causes of disease burden. It’s an unfortunate reality that the majority of strokes occurring in the world are in developing countries, projections over the next 30-years, clearly place increases in incidence and mortality from the burden of stroke in the developing, rather than the developed world. In many regions, some of the most formidable enemies of health are joining forces with the allies of poverty to impose a double burden of disease, disability and premature death in many millions of people. As because of several factors like demographical transition, urbanization, unplanned industrialization, epidemiological transition takes place in the developing countries of the world which causes double burden. This is happening in South Asia, which has one quarter of the global population but where about half of the population live below the poverty line and have limited access to health care. Although infectious diseases remain a formidable enemy, the population is ageing, non-communicable and lifestyle-related diseases are rising. There are bundles of research works done around the globe including developed and developing countries but there have been lack of in-depth study for identification of rehabilitation measures. Data generated through this study might be helpful for the hospital managers to equip themselves to provide better services to stroke patients in different categories of disability. It will also help us create awareness among general population about the risk factors of stroke in Bangladesh. The planners and policy-makers will also be benefited with findings of the study. The present study found that three-fourth of the respondents suffered from hemorrhagic stroke and one-fourth ischemic stroke. About 97.30% of the patients suffered from hemiplegia. About 96.70% patients received both medication and rehabilitation. Almost all of the patients were receiving physiotherapy. Active assisted exercise as means of rehabilitation was prominent (88%) and passive exercise was provided among 12% patients. Statistical significant association was found between gender and type of stroke. Statistical significant association was found between family type and type of stroke. Statistical significant association was found between income group and type of stroke. The greater prevalence of stroke in men is well known.8 Age is the single most important risk factor for stroke. Frequency of stroke rises exponentially with increasing age. The risk of stroke doubles for each successive decade after age 55 years.9-10 It estimates that almost 73% stroke occurs in age 45-64 age group in Bangladesh which affect the golden years of active population. If stroke occurs among working force of our society, definitely it will bring a serious impact on the families of the sufferers. Chapman et al11 which showed the incidence of stroke was high among the high-income group. This results also differ with the study by Hart-CL et al12 which concluded that poor socio-economic circumstances was associated with greater risk of stroke, which was also found in other studies.13-14 Findings of this study may reflect the recent trend of socioeconomic status of Bangladesh. Ischemic stroke account for 50%–85% of all strokes worldwide.15 Haque MM et al16 and Rahman KM et al17 found that 51% and 88.24% hemiplegic in their study. Data also shows that, 47.8% respondents were right sided hemiplegic and 52.2% were left sided hemiplegia among the hemiplegic respondents. They also develop 65.7% disarthria, 17.7% motor aphasia, and 16.6% were normal due to post stroke complication. Speech problem have found significantly higher among hemorrhagic stroke compared to ischemic stroke. Most patients with stroke will need some kind of ongoing physical rehabilitation to assist them in achieving best outcomes possible (with respect to the severity of the stroke but also with respect to the resource available). Perhaps there is a persuasive argument for delivering evidence-based stroke rehabilitation with appropriate levels of quality and intensity as it is considered a human right in many societies. Evidence for physical interventions relating to walking and physical rehabilitation after stroke is becoming increasingly available in the form of high quality systematic reviews that can inform clinical guidelines as well as high level government strategy with respect to stroke. We tend to find it mostly relating to physical therapy and exercise/fitness interventions. Physiotherapy, using a mix of components from different approaches, is effective for the recovery of function and mobility after stroke. Treatment sessions of 30-60 minutes, 5-7 days a week may provide a significant beneficial effect. No one approach to physical treatment is any more (or less) effective in promoting recovery of function and mobility after stroke. Physiotherapists should use their expert clinical reasoning to select individualized, patient-centred, evidence-based physical treatment, with consideration of all available treatment components, and should not limit their practice to a single “named” approach. This study does have limitations. Monthly income of the respondents was collected based on the verbal response so there might be some discrepancy at concrete. Age was estimated on the basis of response. So exact age detection was limitation of this study.
Disability is common after stroke. Reducing disability through rehabilitation programme is demanded. Three-fourth of the respondents (76%) suffered from hemorrhagic stroke and one-fourth (24%) ischemic stroke. About 97.30% of the patients suffered from hemiplegia. About 96.70% patients received both medication and rehabilitation. Almost all of the patients were receiving physiotherapy. Active assisted exercise as means of rehabilitation was prominent (88%) and passive exercise was provided among 12% patients. Statistical significant association was found between gender and type of stroke. Statistical significant association was found between family type and type of stroke. Statistical significant association was found between income group and type of stroke.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
