
Review Article | DOI: https://doi.org/10.31579/2692-9759/134
*Corresponding Author: Franz Porzsolt, Institute of Clinical Economics (ICE), 89081 Ulm / Germany.
Citation: Franz Porzsolt, (2024), Reducing corporate interests, failed regulation, and commercialization of academia, Cardiology Research and Reports, 6(5); DOI:10.31579/2692-9759/134
Copyright: © 2024, Franz Porzsolt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 August 2024 | Accepted: 19 August 2024 | Published: 28 August 2024
Keywords: covid-9; respiratory diseases; self-care; treatment adherence
.
The British Medical Journal has recently published an opinion paper on "Illusion of Evidence based Medicine" [1]. This paper describes a global problem, the dimension of which only be-comes apparent through the risks that arise as a result of this illusion. The resulting problem may be the three dimensions of “disbalanced health-care (dbhc)”. (a) The health problems of the patients are inadequately solved. (b) Neither the monetary expenditure on health (c) nor the non-monetary burdens to be accepted on individual patients and society are outweighed by the added health and social value of the services provided.
Corrective measures to reduce dbhc were recently outlined in a paper "Comparative effective-ness is the common denominator in health services research: experimental effects are promis-ing, real-world effects are compelling" [2]. The lack of differentiation between the effects generated under experimental study conditions and real-world conditions has been referred to as a "terminology conflict" [3]. Our goal is to integrate complementary strategies and methods into health care that have proven themselves from the perspective of science, patients and so-ciety. This implementation is intended to increase the efficiency of health-care [4, 5] i.e.,
• The quantification of healthcare effects under day-to-day conditions of healthcare
• Without an increase in undesirable non-monetary burden and
• Without increasing the monetary burden on patients and society.
The conventional definitions of CIM did not address the optimization of care under everyday conditions – in contrast to experimental laboratory conditions [e.g., 6 - 9]. The reason for this missing aspect has so far been the lack of a suitable method to detect differences in the quality of care under everyday (pragmatic, but not experimental) healthcare conditions [2, 10]. Proof of real-world effectiveness (RWE) could free CIM from its stigmatizing label of lack of evi-dence and pave new ways of describing the different forms and functions of CIM. Trust in non-stigmatized care methods is likely to increase and effects of combined therapies could be explained.
This review deals with the question of a new challenge to the claim of CIM. In addition to new interventions, CIM could also discuss new conceptual and methodological details. The maximum achievable successes and the unavoidable monetary and non-monetary burdens can be quantified. As an example to confirm the practical importance of this concept, we use a published proposal [11].
The published proposal
Four international cardiology societies (European Society of Cardiology, American Heart As-sociation, American College of Cardiology, World Heart Federation) issued a joint statement proposing a modification of randomized controlled trials (RCT) [11]. This modification is jus-tified by increased administrative requirements and financial burdens, as well as a dispropor-tionately low information gain from conventional RCTs. In a ‘joint opinion’, the design of an adaptive platform study is proposed to replace the traditional RCTs [12] because promising results could be achieved by this study design in different studies [13 - 15].
We agree with the ‘joint opinion’ group's call for a necessary optimization of the standards for gaining knowledge in the healthcare system. Before description of our methodological details, we may mention the supportive framework conditions, the "Ulm heritage", without which we would probably not have been able to cross the boundaries of the traditional way of thinking.
The “Ulm heritage”
The idea of evaluating the results of experimental studies and pragmatic care outside of stud-ies with different tools was triggered in the late 1980s when one of us, a young oncologist, noticed that treatment successes in patients at our own university hospital differed more than marginally from published oncology reports. Nearly a decade passed before a simple idea could plausibly explain the difference. We observed effects in our hospital that occur in eve-ryday care (or Real-World Effectiveness, RWE), whereas journals reported data were that were predominantly generated in experimental studies under strictly controlled conditions describing efficacy (or Proof of Principle; PoP). Although the scientific literature differentiat-ed between "efficacy" and "effectiveness" quite early [16 - 18], the explanations were not user friendly enough to become widely established.
Our research in evidence-based medicine was based on the three questions of Sir Archibald Cochrane and Sir Austin Bradford Hill – "Can it work? Does it work? Is it worth it?" – that should be answered before new interventions will be integrated in standardized healthcare [19]. Cooperation with teachers and students in the "ulmer hochschule für gestaltung (hfg)" (Ulm school of design) taught us the rule "Form Follows Function (FFF)"generated by Amer-ican designers and architects [20] and have passed on the demand of the founders of the hfg that the designers should develop universally valid solutions with relevance to social policy [21 - 22]. As citizens of Ulm, we are familiar with many of Albert Einstein’s (*1879 in Ulm) statements, e.g., “Problems cannot be solved with the mindset that caused them”.
These three recommendations of (a) the British epidemiologists, (b) the American designers and architects, and (c) the teachers and students of the former hfg facilitated the development of a three-dimensional strategy and a new method for the evaluation of healthcare perfor-mance. Here we describe some results of the new way of thinking in five themes. Finally, we suggest concrete contributions that CIM could make to reduce the undesirable consequences of the "illusions of evidence-based medicine".
Results in five themes
1.Forms and functions of the three-dimensional strategy
The concept of the three-dimensional strategy is based on the three Cochrane-Hill questions. Each of the responses to these questions is characterized by a specific form (structure) and function.
The response to the first question, "Can it work?", is characterized by the form (structure) of an RCT and represents the objective function of the PoP. The PoP basically reflects the per-spective of clinical research.
The response to the second question, "Does it work?", is characterized by the form (structure) of a Pragmatic Controlled Trial (PCT) and represents the objective function of RWE. The RWE basically reflects the perspective of health services research.
The response to the third question, “Is it worth it?”, is characterized by the forms (structures) of various Complete Economic Analyses (CEA) and represents the function of subjective Value (VAL) of healthcare services from an economical perspective of individual persons and the society (Table 1).
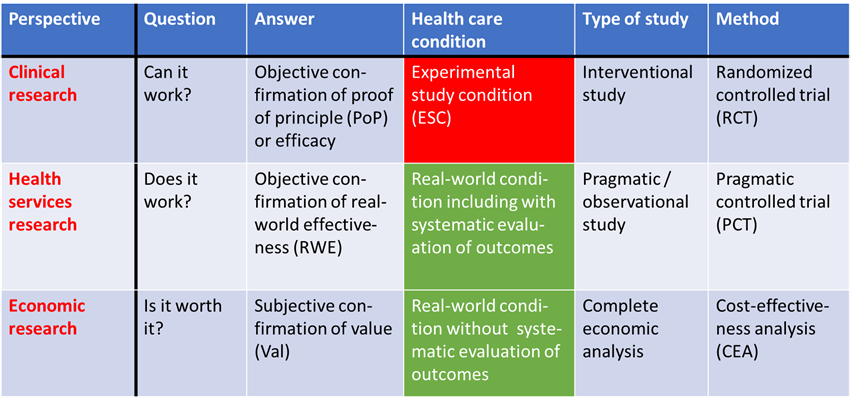
Table 1: Strategy for answering the three Cochrane-Hill questions from the perspectives of clinical research, health services research, and economic research (modified from [24]).
2.The conditions for implementation of care and analysis of outcomes are different
Care. Patient care can be implemented only under two different conditions (or forms of care): either under non-experimental (Nex) and unstructured, natural conditions (of everyday) care or under experimental (Ex) and strictly structured conditions of care.
If some of the subjects were eliminated from an original (Nex) target population to protect the excluded subjects from specific risks of an investigated intervention (by defining exclusion criteria), an artificial (Ex) population will be created. This artificial (Ex) population cannot represent results generated under natural, Nex and unstructured conditions.
Consequently, the effects observed in such a "risk-reduced population” cannot reflect the results obtained under RWC. The effects observed in such a population may describe the Proof of a Principle (PoP) but never the true RWE.
Analysis of outcomes. The results of treatment can be analyzed under three conditions (or forms): (a) under experimental (Ex) and strictly structured study conditions or (b) under non-experimental (Nex) and unstructured, natural (everyday) care conditions either (b1) with or (b2) without determination of the individual “endpoint-specific risks profiles (ESRPs)” of the patients.
The analysis of results under (Exp) experimental and structured conditions of a RCT results in the description of PoP. The analysis under Nex and natural conditions of a PCT (b1) with de-termination of the individual ESRPs of the patients results in the RWE. A systematic analysis of the results under the usual everyday (Nex) non-experimental conditions (b2) is impossible. Under these conditions outside of a clinical trial, only pre-post comparisons on individual pa-tients are possible.
3.Different tools are needed for assessment of outcomes in RCTs and PCTs
An RCT only guarantees the equal distribution of risk profiles. The average risk profiles of different RCTs are usually not comparable due to missing or imprecise description of the se-lection criteria. This unprecise definition of the selection criteria explains the lack of external validity of the results of most RCTs.
In a PCT, each patient is cared for under non-structured, natural everyday care conditions, but evaluated under structured conditions by applying Bayesian statistics. The advantage of Bayesian statistics over randomization is the ability to apply statistical methods under the non-structured conditions of everyday care without altering these natural conditions. The applica-tion of the Bayesian method in healthcare requires documentation of the intervention (thera-py) and all individual risk factors that could affect any of the measured endpoints of a PCT. Based on the categorization of therapies and individual risk profiles, each patient can be as-signed to the appropriate risk class with respect to each of the measured PCT endpoints [3, 10, 23, 24]. This accurate risk classification requires a large number of cases to account for multi-ple variables in one analysis. Patients with identical target diseases should be assigned to a risk class for each of the measured endpoints. This risk class divides this patient's risk of achieving the investigated adverse endpoint as high, intermediate, or low. In addition, the intervention applied is taken into account. The different conditions of healthcare provision and the result-ing functions and forms of the two objectively measurable dimensions of efficacy (PoP) and effectiveness (RWE) are summarized in Table 2.
| Efficacy (or PoP) is measured in a target population whose risk profile is defined by both inclusion and exclusion criteria of an RCT*. | Effectiveness (or RWE) is measured in a target population whose risk profile is defined only by inclusion criteria of a PCT (exclusion criteria do not exist in PCT)*. | |
| Functions of efficacy and effectiveness | Proof of principle (PoP; efficacy) under structured conditions of an experimental study (e.g. RCT) | Real-world effectiveness (RWE) under structured conditions of an observational study (e.g. PCT). |
| Forms (structures) of efficacy and effectiveness | Experimental (Exp) studies (RCTs; for assessment of PoP) differ in 12 criteria from the conditions of everyday care. | Non-experimental (Nex) Pragmatic studies (PCTs; for assessment of RWE) agree in six criteria with everyday care and in four criteria with experimental studies. |
Table 2: Application of the FFF designer rule to explain the different forms (structures) and functions of the two outcome dimensions, efficacy (PoP) and effectiveness (RWE). *Inclusion criteria describe the health problem to be solved, exclusion criteria identify the hurdles to solve the problem [25].
4.Explaining three different outcomes under two different conditions
Table 1 describes the healthcare strategy from three different perspectives. From these per-spectives, three different outcomes can be derived, although the supply can only take place under two different conditions - either experimental or non-experimental healthcare conditions [24]. This apparent conflict can be resolved by a simple explanation. By far the most common form of daily care takes place outside of clinical trials under conditions of "natural chaos" [10]. However, a systematic evaluation of the results is impossible in a “natural chaos” without any measures to structure the available information.
Therefore, a concept had to be applied that can structure the available information without changing the "natural chaos" of care. This apparent squaring of the circle could be solved by two steps. On the one hand, it was possible to distinguish the differences between three con-ditions of health care i.e., care under experimental conditions or under non-experimental con-ditions either with or without systematic recording of the individual patient’s risk profiles. The differences are described by two different functions and twelve different forms (structures) [25]. In addition, we were able to maintain the "natural chaos" by replacing the experimental randomization with non-experimental Bayesian statistics. In simple terms, Bayesian statistics is based on the principle of specifying the prediction of an event by calculating the probability of an expected event, with and without taking into account the factors that can favor or pre-vent the occurrence of the expected event [26].
5.Importance of study conditions and selection criteria
More attention should be paid to the exact description of both the study condition and the selection criteria in clinical trials. It is not possible to distinguish between the detection of PoP or RWE if the conditions (Ex or Nex) under which the study was carried out are not de-scribed. Neither will it be possible to predict the prognostic significance of an intervention if the selection criteria of the investigated target population are incompletely described or com-pletely missing [27]. Both the chosen study conditions and the chosen selection criteria influ-ence the study results via direct and indirect effects. Direct effects are the exact formulation of the study objective, the results obtained, and their interpretation. Indirect effects affect the homogeneity of a study by testing the eligibility of the patients included in a study. When the inclusion and exclusion criteria of the single studies that were included in a meta-analysis are only vaguely defined or even missing, it may be impossible to confirm the validity of the (pre-cisely) calculated results of this metanalysis [28].
Both inclusion and exclusion criteria depend on the study question but have different func-tions. Inclusion criteria of clinical studies should describe the problem to be solved, while ex-clusion criteria should identify the confounders that influence the assessed endpoint in exper-imental trials. Inclusion criteria are required for any form of health-related study as opposed to exclusion criteria. Exclusion criteria exist only in experimental studies, but not in studies de-scribing everyday healthcare, like the PCT or studies describing the subjectively perceived added value of a healthcare service or health-related quality of life [29]. We are concerned that the definition of exclusion criteria contains a risk that has not yet been taken into account. The exclusion criteria may distort the description of the actual risks of interventions, because the approval of drugs requires the detection of effects in experimental RCTs. RCTs report results obtained from patients without any risk factors that may affect the measured outcome except the investigated disease. This highly selected patient population cannot be representa-tive of all patients to whom the results of this RCT are applied.
Here we discuss the motivation to address the “illusion of evidence based medicine” and a possible strategy to solve it.
The motivation to address the challenge.
The comments of various authors confirming the "illusion of evidence-based medicine" and the publication of these comments by the scientific journals [1, 30, 31] supported by the de-mand of international professional societies to develop methods that facilitate the conduct of the necessary studies [11].
Our review confirms the statement of the professional societies. The current gold standard of the RCT is, indeed, no longer suitable for justifying the necessary decisions on health care. The three-dimensional Cochrane-Hill strategy and the topics we elaborated in this review may be related topics of discussion.
We recommend to use the FFF rule of architects and designers for confirmation of the quality of new products of concepts in science. This rule turned out to be useful in solving the termi-nology conflict [3, 29] and in distinguishing PoP and RWE (Table 2). The suggested differ-ences of PoP and RWE may be considered for several reasons.
•RCTs include only a highly selected patient population in which most risk factors in-fluencing the measured primary endpoint (with the exception of the intervention stud-ied) have been eliminated by exclusion criteria. In a PCT, exclusion criteria cannot be applied because they would eliminate significant confounding factors whose influence on outcomes in day-to-day care cannot be prevented.
•An RCT limits the choice of healthcare options to the few interventions that can be compared and interpreted in an experimental study. The PCT does not limit the choice of health care. Each participant selects with their physician the intervention that is ex-pected to produce the optimal results for that patient.
•An RCT is expected to ensure the equal distribution of all risk factors not excluded in the study populations. This, however, can hardly be confirmed because the size of the studied population depends on a large number of variables, e.g., the number of study participants and of risk factors, the effect sizes of risk factors, and their interrelation-ship. The smaller the population studied in an RCT, the greater the risk of unequal dis-tribution will be in the randomized groups. In PCTs, the differences in patient risk pro-files can be successfully managed by stratification according to the individual ESRPs.
•The time and costs of development to market access will be considerably reduced in PCTs for two reasons. The recruitment of patients in a PCT is by a multiple easier than in an RCT and the value of the information collected in a PCT is by far greater than in an RCT.
•The financing of PCTs has to be renegotiated because the care of patients in a PCT is not an experiment. Only the extraction of new scientific knowledge from the results obtained under the conditions of natural chaos requires additional costs. Most of these costs are incurred for the development of the study protocol, because after the target disease has been determined, a list of all risk factors that can distort one of the meas-ured endpoints has to be drawn up, from this study-specific risk list separate risk pro-files are to be defined for each endpoint, with which each patient can be assigned to an endpoint-specific risk group.
•The prediction of the individual's risk-dependent chance of successful care explains the significant difference in knowledge gained by a PCT in contrast to RCT.
As result of our research we may conclude the conception of health care should be based on RWE but not PoP. The scientific details of the concept are described [3, 10, 23, 24]. A sum-mary of the practical aspects to be taken into account when applying the concept in everyday care was published recently [32]. The concept could benefit from the support of colleagues who trust complementary and evidence-based innovations of traditional medicine and are committed to implementing these innovations.
The strategy to solve the challenge.
The links between business and science in the healthcare system will increase rather than de-crease in the future. These connections are driven by two powerful incentives that, depending on administrative control, can increase or decrease successes in both systems. In both systems, the incentives relate to the development and marketing of innovative products and concepts. These products and concepts have a direct impact on economic success. The success of scien-tific achievements in a health care system can only be measured indirectly by the quantifiable health consequences of the gain in knowledge.
The "illusion of evidence-based medicine" verbalized a weakness of evidence-based medicine that needs to be improved. This weakness describes the difference between the theoretical concept and the practical implementation of the evidence-based method. Conflicts of interest are a characteristic of biological variance and are therefore unavoidable. However, the inap-propriate handling of conflicts of interest can be avoided. Table 3 describes the conflicts of interest between science and business in healthcare.
| Functions | Forms (structures) | ||
| Scientific institute | Business enterprise | ||
| Scientific function: knowledge generation | (a) Develop an idea that may solve a problem (b) Express the idea as question in plain language | Institutions with scientific reputation should solve scientific tasks. | |
| Economic function: generation of profit | Institutions with economic reputation should solve economic tasks. | Profit maximization as a prerequisite for survival of a society, considering (a) economic, (b) social and (c) ecological aspects. | |
Table 3: Conflicts of interest between science and business in healthcare can be recognized by the lacking congruence of forms and functions [25].
The conflict between science and business was first addressed in the late 60s and has since spread to new areas and increased in intensity [1, 30, 31, 33]. Patients and health care profes-sionals can only make suggestions, policy makers take decisions [34] e.g., need to decide on the priority of the challenges outlined by Jureidini and McHenry [1]. Patients and health care professionals can only make suggestions. We have drawn up proposals for the application of the American recommendation on “checks and balances”.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
