
Research Article | DOI: https://doi.org/10.31579/2639-4162/038
1 Department of Geriatric and Palliative care, The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
*Corresponding Author: Jochanan E. Naschitz, Department of Geriatric and Palliative care, The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: J E. Naschitz, I Yalonetzki, G Leibovitz, N Zaigraykin. (2020) Red Blood Cell Distribution Width/Hemoglobin Ratio Correlate with Severity of Clinical Status in Residents of Long-term Geriatric and Palliative Care. General medicine and Clinical Practice. 3(4) DOI:10.31579/2639-4162/038
Copyright: ©2020 Jochanan E. Naschitz. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 September 2020 | Accepted: 20 November 2020 | Published: 05 December 2020
Keywords: cell distribution; hemoglobin ratio; geriatric; palliative care
Background: The red blood cell distribution width (RDW) is a simple measure of red blood cell size heterogeneity. A high degree of anisocytosis, expressed by RDW >15%, is observed in certain anemias, but also in other disorders, where RDW >15% is associated with worse prognosis. We questioned whether the RDW/hemoglobin ratio (RDW/Hb) might closer relate to disease severity than RDW.
Design: Cross sectional study
Patients: 76 residents of two Department of Comprehensive Nursing Care.
Method: Physicians classified the patients according to their clinical status in three groups: "stable", “severe-unstable”, and "intermediate". An outside observer extracted from the patients' files the results of RDW (elevated if >15%), hemoglobin, iron, and transferrin. The RDW (%)/Hb (g/dL) ratio and tansferrin saturation (TSAT) were computed. The associations between RDW, RDW/Hb, TSAT, and the patients' clinical status were assessed.
Results: In residents of Department A, RDW >15% was found in 33% of 19 stable patients, in 58% of 10 patients with intermediate severity, and in 81% of 10 patients classified severe-unstable. The RDW/Hb ratio >1.4 was found in 24% of stable patients, in 73% with intermediate severity, and in 93% of the severe-unstable patients. In Department B, 36 out of 38 patient's were classified stable: in 61.2 % the RDW was >15% and in 38% the RDW/Hb was >1.4.
Conclusions: In a heterogenic population presenting multimorbidity, the RDW and to a higher degree the RDW/Hb (p <0.00001), correlated with the patients' disease severity.
Red cell distribution width (RDW) indicates variability in red blood cell size. It is a standard parameter of the complete blood count, derived from the RBC size histogram measured by automated cell counters [1]. RDW normal range in our laboratory is 11.6% to 15%. Higher RDW indicates dysfunctional erythropoiesis, shortened RBC lifespan, or premature release of reticulocytes and may be due to oxidative stress, inflammation, poor nutritional status, alteration of erythropoietin function, tumorigenesis [2-16]. Traditionally, the RDW has been used in the diagnosis of anemias, but recently there is awareness of an association between elevated RDW and an increased risk of morbidity and mortality independently of anemia in numerous disease states. An elevated RDW was found in cardiovascular diseases, venous thromboembolism, cancer, hematologic malignancies, diabetes, rheumatic disorders community-acquired pneumonia, chronic obstructive pulmonary disease, liver and kidney failure, sepsis, critical illness, etc [3-16]. There is increasing evidence that the RDW might be helpful in assessment of disease severity and prognostication of patient survival [4-16].
Since anemia and RDW are independent predictors of disease severity, and frail elderly patients with multimorbidity often have chronic diseases as well as anemia, we combined RDW and Hb in a single measure. We proposed the combined parameter RDW/Hb ratio and tested in the present study study whether RDW/Hb might closer correlate with disease severity than does the parent RDW in a population of severely disabled patients by multimorbidity.
Patients and Methods
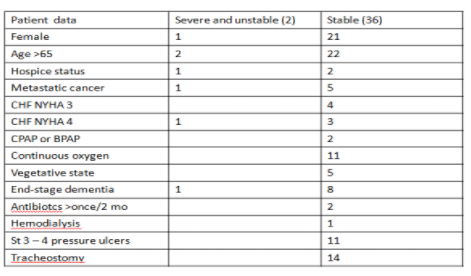
The institutional Review Board approved this observational cohort study and waived the need for informed consent, due to the study design. Included were all residents in Departments A and B of Comprehensive Nursing, provided they were staying in the ward for at least four weeks. In either department, 38 subjects out of 40 met this condition. The median duration of hospitalization in Department A was 4 months (range 1-79 months) and in Department B 5 months (range 1- 60 months). On study day a physician who was closely implied in the patients' care estimated their clinical state. A defined set of data was reviewed, those which could impact on the patient's outcome: age >65, hospice status, metastatic cancer, congestive heart failure NYHA stages 3 and 4, use of CPAP or BPAP, continuous oxygen supplementation, vegetative state, end-stage dementia, hemodialysis, stage 3 or 4 pressure ulcers, antibiotic prescription more than once during the last 2 months. In addition, the disease trajectory during the patient's stay in the ward, and the physician's intuition of the short term prognosis [17] were at the basis of classifying the patients in three groups: “severe-unstable”, "stable", and "intermediate".The following laboratory data were extracted from the patients' medical records by an independent observer: RDW, hemoglobin, iron, and transferrin. RDW >15% was considered elevated. The RDW/hemoglobin ratio (RDW/Hb) was calculated in which the RDW is expressed in percent and the hemoglobin in g/dL. We proposed the RDW/Hb based on results of a pilot study in residents of long-term geriatric care showing that a RDW/Hb ratio >1.4 closer correlated with poor patient prognosis than did RDW >15%. (Naschitz JE, unpublished observation). The transferrin saturation (TSAT) was calculated according to the equation TSAT = iron (microgram/dL)/transferrin (mg/dL) x 71.24. While TSAT <20% and more so <18% suggest an inadequate supply of iron for erythropoiesis, a very low value <15% is characteristic of iron deficiency [18]. A cutoff TSAT <15% was used in our study to mark iron deficiency.
The correlations were assessed between the hematologic indices (RDW, RDW/hemoglobin, TSAT) and the physicians' estimate of the patient condition. For statistical analyses, Student's two tailed t-test was used. P values <0.05 were considered significant.
Result
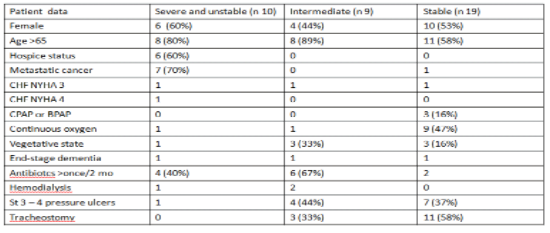
Seven patients having metastatic cancers (six among them in hospice status) were classified "severe and unstable", making out the majority in this category. One patient with metastatic prostate cancer, well controlled under hormonal treatment, was included in the "stable" group.
The RDW, RDW/Hb and TSAT averages and SD of residents of Department A are presented in Table 3. The RDW and RDW/Hb differed significantly between stable patients and all others (Table 4). The best discrimination between stable patients and the others categories was noticed for RDW/Hb >1.4. Similar analysis was done in residents of department B (Tables 5 and 6)


The study parameters of residents in Department B are shown in Tables 5 and 6.


An elevated RDW was found in a variety disorders, including cardiovascular diseases, venous thromboembolism, cancer, hematologic malignancies, diabetes, rheumatic disorders, community-acquired pneumonia, chronic obstructive pulmonary disease, liver and kidney failure, sepsis, and critical illness [3-16]. Our study addressed patients with multimorbidity and severe frailty, hospitalized in long-term geriatric and palliative care. In this population the RDW correlated with disease severity and clinical instability. This correlation was significant in residents of Department A which comprised a heterogenic population (10 classified unstable, 19 stable, and 9 of intermediate severity); the correlation could not be assessed by means of statistics in residents of department B where only two patients were unstable and all others classified stable. The combined parameter RDW/Hb correlated closer with diseases severity and clinical instability than did RDW.
The mechanism by which RDW carries a strong prognostic significance across many diseases is unclear. An explanation might be in the positive correlation between RDW and inflammatory markers, including interleukin-6, C-reactive protein, soluble tumor necrosis factor (TNF) receptors I and II, hepcidin, and soluble transferrin receptor. Indeed, inflammation impairs erythropoiesis and causes changes in red blood cell maturation, which contribute to anisocytosis [18]. Also, chronic intermittent hypoxemia is associated with elevated RDW, possibly via intermittent surges in erythropoietin [19]. The RDW was shown to be associated with malnutrition, inhibition of iron transport and utilization, and poorer prognosis in cancer patients [18]. Additional findings suggest that RDW is related to the aging process [20,21]. Although it is not established whether an elevated RDW is a risk factor or a risk marker, i.e. and epiphenomenon of the underlying biological imbalance, an elevated RDW conveys in general important information for short and long-term prognosis (2-16). So, the RDW might serve as an integrative measure of multiple clinical and subclinical processes occurring simultaneously. We tested the hypothesis whether the relationship between RDW and clinical status severity can be strengthened by merging RDW and hemoglobin as a combined parameter. In the present study RDW/Hb >1.4 was found in 93% of patients with severe-unstable status and only in 24% and 38%, respectively, of patients in stable condition in either department. The RDW/Hb correlated closer than RDW with the patients' clinical condition. The advantage of the combined parameter RDW/Hb over RDW may be analogous to the advantage of the combined parameter RDW-carcinoembrionic antigen, better predicting the prognosis for survival in colorectal cancer than either parameter alone [18].
There are limitations to our present study. First, the estimate of patients' clinical status by physicians is intuitive to a certain degree and might not be identical by different physicians, which might partially explain the differences of patient classification in departments A and B, and also might have affected the results. Second, inhomogeneity of the patient population in this study, while illustrating the real-life situation in long-term and palliative care, does not permit to focus separately on each disease. Third, the RDW/Hb might population dependent [22]. The advantage of RDW/Hb over RDW in the present study, comprising patients with severe frailty and multimorbidity, might not hold for fit older subjects. Whether or not RDW or RDW/Hb might serve as independent prognostic factors in residents of long-term geriatric and palliative care needs to be assessed in prospective studies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
