
Case Report | DOI: https://doi.org/10.31579/2690-8794/027
1* Brookdale University Hospital and Medical Center, Brooklyn, New York, USA.
2 SUNY Downstate Medical Center, Brooklyn, New York, USA.
*Corresponding Author: Farla Jean-Louis, Brookdale Hospital, Brooklyn, New York, USA.
Citation: Farla J. Louis., Syed A., Upadhya G., (2020) Recurrent Syncope in a patient with Sleep Apnea and Narcolepsy resolved after Permanent Pacemaker Implant, Clinical Medical Reviews and Reports. 2(8); DOI: 10.31579/2690-8794/027
Copyright: © 2020 Farla Jean-Louis, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 August 2020 | Accepted: 29 August 2020 | Published: 06 October 2020
Keywords: syncope; narcolepsy; sleep apnea; pacemaker; atrio ventricular block; sinus arrest
Concomitant narcolepsy and sleep apnea (SA) can be present in the same patient. We present a patient with recurrent episodes of syncope and subsequent falls, which were found to be due to narcolepsy and Obstructive Sleep Apnea (OSA). She was initially treated with continuous positive airway pressure (CPAP) but continued to have symptoms sustaining injury. Her symptoms resolved with placement of a permanent pacemaker (PPM) implant and to date has not had any recurrence.
OSA is characterized by apneic/hypopneic episodes caused by repetitive collapse of the upper airway during sleep. SA is treated with CPAP which prevents these episodes by maintaining positive pharyngeal transmural pressure while stabilizing the upper airway through increased end-expiratory lung volume [1, 2] . Narcolepsy is defined as daytime sleepiness associated with cataplexy, hypnagogic hallucinations and sleep paralysis. It is usually treated with lifestyle modifications such as improved sleep hygiene and health maintenance, but may also require pharmacologic therapy [3, 4]. We present a case of a 41 year old female with a history of OSA, Obesity Hypoventilation Syndrome (OHS), and narcolepsy who presented to the hospital for recurrent episodes of syncope with falls. She was found to have episodes of daytime narcolepsy with intermittent episodes of sinus arrest and third degree atrio-ventricular block (AVB). The patient was compliant with her CPAP at night, however, was still noted to have significant bradyarrhythmias. During hospitalization, she underwent implantation of a PPM with resolution of her syncopal episodes.
This is a case of a 41 year old female with a past medical history (PMHX) of narcolepsy, OHS, OSA (on home CPAP) and hypertension (HTN) who was admitted to the hospital with recurrent episodes of syncope and falls. She was advised to make lifestyle modifications previously for her narcolepsy, but her symptoms persisted. She reported an inability to maintain her work due to her recurrent falls with episodes of syncope.
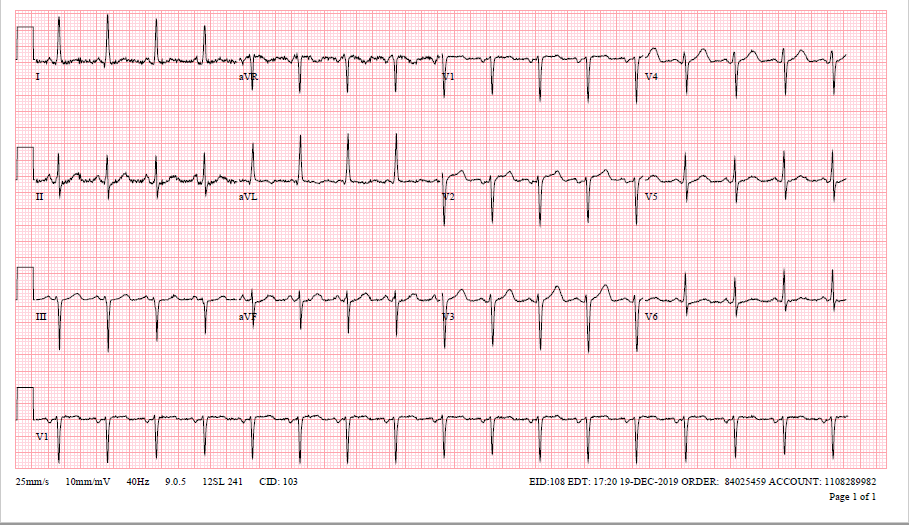
On arrival to the emergency department (ED), her vital signs were stable, and physical examination (including orthostatic blood pressure) unremarkable, with the exception of morbid obesity (weight: 159.9 kg ,body mass index (BMI): 55.9). Her laboratory tests did not demonstrate any electrolyte or endocrine abnormalities. Her arterial blood gas (ABG) was significant for hypercapnia (PCO2: 65.5 mmHg; Normal 35-45 mmHg). Her 12-lead electrocardiogram (ECG) demonstrated normal sinus rhythm (NSR) and left ventricular hypertrophy (LVH), without any significant abnormalities (Figure 1). The patient was admitted to the telemetry unit for continuous cardiac monitoring and further evaluation of her recurrent syncopal episodes.
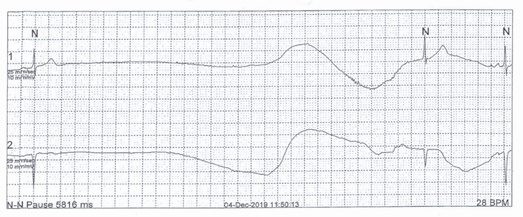
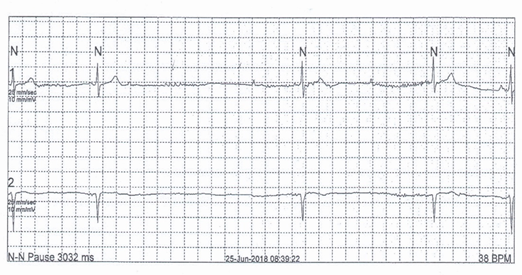
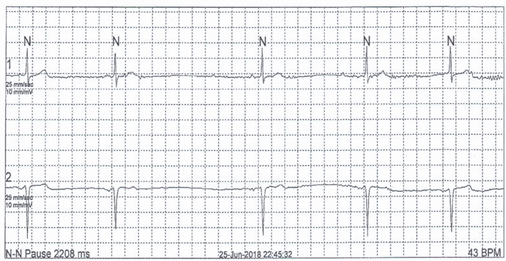
During her hospitalization she had an echocardiogram, which demonstrated a hyper-dynamic left ventricle, without any significant valvular abnormalities. She completed a 24-hour holter monitor, which reported basic sinus rhythm. However, there were episodes of marked bradycardia, down to 40 beats per minute (bpm), with episodes of sinus arrest/pauses during waking hours (Figure 2). The patient had a holter performed about a year prior to this admission which also revealed similar bradyarrhythmias during both daytime and nighttime hours, with the addition of intermittent third degree AVB (Figure 3, 4).
A computed tomography angiography (CTA) of the chest and a venous doppler of the lower extremities were performed which ruled out a pulmonary embolism (PE) and deep vein thrombosis (DVT). Telemetry monitoring also revealed periods of sinus bradycardia, with intermittent sinus pauses and AVB’s during daytime hours. No other reversible etiologies for her bradyarrhythmias were determined. Due to the recurrent episodes of syncope in the presence of sinus arrest with high degree AVB, the decision was made to proceed with PPM implantation. She underwent successful placement of a dual chamber PPM without complications and was discharged home in stable condition.
Since discharge, the patient has been following up routinely at our outpatient cardiology clinic. Six months since placement of the PPM, she has not had any recurrent episodes of syncope nor falls. She has also been able to maintain her current employment without any issues.
Cardiac rhythm disorders have been reported in patients with OSA. Several explanations have been described, such as negative intrathoracic pressure during efforts to breathe, intermittent episodes of hypoxia, and/or surges in sympathetic activity [5]. OSA has a strong positive correlation with an elevated BMI, via chronic obstruction of the upper airways with resultant apneic and hypopneic episodes [6]. These possible explanations for arrhythmias in OSA, may also apply to our patient who was morbidly obese with a BMI of 59.9.
The most common arrhythmia identified in OSA is atrial fibrillation, which is likely related to left atrial dilatation and remodeling [5]. Bradycardia has also been reported to occur in patients with increased vagal tone [5]. More specifically, it may occur during apneic episodes, when the absence of ventilation and resultant hypoxia both stimulate an increase vagal response from the carotid body [7]. One small study involving 6 patients with OSA, found bradycardia to be a consistent arrhythmia, postulated to have been caused by a combination of apnea and hypoxemia [8]. Episodes of heart block have also been reported, especially among patients with severe OSA (greater than 60 apneic and/or hypopneic episodes per hour) [9].
Bradycardia can be present in the setting of narcolepsy. Narcolepsy is often characterized by excessive daytime sleepiness and cataplexy, with early onset rapid eye movement (REM) sleep. Narcolepsy has also been associated with decreased levels of the neuropeptide, hypocretin - 1 (Hcrt - 1) in the cerebrospinal fluid (CSF) [10]. Hcrt-1 deficiency has been found to significantly influence the autonomic nervous system, including resting heart rate [10]. Hcrt-1 fibers are present in the lateral paragigantocellular nucleus, which is responsible for the inhibitory pathway for preganglionic cardiac vagal neurons [10]. It is via this inhibitory pathway, that a deficiency of hcrt-1 leads to an attenuated chronotropic response during both REM and non-REM sleep [10].
Narcolepsy and OSA can be concurrent disorders. One study found that 6% of patients with a positive multiple sleep latency test (MSLT) experienced respiratory issues during sleep, suggestive of both narcolepsy and OSA coexisting [11].
The use of CPAP in our patient did not alleviate her symptoms nor suppress her arrhythmias. Our patient’s OSA was neither amenable to surgical intervention, nor responsive to central nervous system (CNS) stimulants. Our patient’s management was unique as there was complete resolution of symptoms after the implantation of a PPM.
Cardiac rhythm disorders, specifically bradyarrhythmias, are likely a common pathology in patients with narcolepsy and OSA. The coexistence of both of these disorders should be strongly considered as a possible etiology in patients with recurrent episodes of syncope and falls. Thus, when patients with clinically significant arrhythmias, especially bradyarrhythmias, are found in conjunction with OSA and/or narcolepsy, indications for PPM implantation should be investigated if conventional therapies fail.
None to declare.
No funding was received. None of the authors have disclosures relevant to this manuscript.
None to declare.
The manuscript has been sufficiently de-identified to protect the patient.
The corresponding author, FJL and AS, wrote the main manuscript. GU provided additional research data in the introduction and discussion section. AS provided the electrocardiogram (Figure 1). All authors reviewed the final manuscript.
The authors declare that data supporting the findings of this study are available within the article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
