
Case Report | DOI: https://doi.org/10.31579/2578-8868/241
1 Department of Neurology, University of California Irvine, Orange CA
*Corresponding Author: Amit Chaudhari, Department of Neurology, University of California Irvine, Orange CA.
Citation: Sophia Angelides, Amit Chaudhari, Tigran Khachatryan, Wengui Yu, (2022). Recurrent Ischemic Strokes in the Territory of Recurrent Artery of Heubner Presenting in Relation to Facial Swelling and Weakness. J. Neuroscience and Neurological Surgery. 11(4); DOI:10.31579/2578-8868/241
Copyright: © 2022 Amit Chaudhari, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 18 March 2022 | Accepted: 04 April 2022 | Published: 11 April 2022
Keywords: huebner; stroke; neurology; ischemic stroke; case report
Strokes involving the Recurrent Artery of Huebner are quite rare and are often asymptomatic. Here, we describe a rare case of recurrent infarctions involving the right Recurrent Artery of Heubner, likely due to small vessel disease. Our 32-year-old patient presented to the emergency department with sudden onset right-sided facial weakness, numbness, and difficulty with eye closure. A non-contrast head computed tomography scan and magnetic resonance imaging revealed an incidental subacute infarct in the territory of the right Recurrent Artery of Heubner. He was discharged on valacyclovir and prednisone for suspected Bell’s palsy, as well as aspirin, atorvastatin, metformin, and antihypertensives for secondary stroke prevention. Unfortunately, he was noncompliant with medications and lost to follow-up until he presented again more than one year later with a complaint of isolated right facial swelling and ipsilateral weakness. Imaging revealed an incidental new subacute infarct in the territory of the right Recurrent Artery of Heubner. Close follow-up of the patient and guidelines for appropriate management of secondary risk factors are discussed.
The Recurrent Artery of Huebner has been discussed as having many variations in its origin, its course, and the areas which it supplies. It most commonly arises from the anterior cerebral artery within 2 mm of the anterior communicating artery and is known to reliably supply the head of the caudate nucleus, the anterior inferior limb of the internal capsule, the external globus pallidus, the nucleus accumbens, the hypothalamus, the uncinate fasciculus and olfactory regions [3]. Infarctions of the RAH are rare and not often documented, but are classically known to cause contralateral hemiparesis, predominantly in the upper extremity with facial involvement [5]. Other documented symptoms have included abulia, change in affect, delusions, disinhibition, disorientation, dementia, or patients may be asymptomatic [2,7-9]. Here, we describe a rare case of recurrent infarctions involving the right Recurrent Artery of Heubner, likely due to small vessel disease.
This is a case report describing neuroimaging findings from a 32-year-old man who presented to the University of California Hospital System. A typical stroke MRI protocol was used with diffusion, T2/FLAIR and susceptibility-weighted images. All images were acquired on a 1.5T MRI scanner. The patient consented to publication of non-identified data for research purposes, and all research activities were in accordance with the strict guidelines put forth by the University of California Irvine Institutional Review Board.
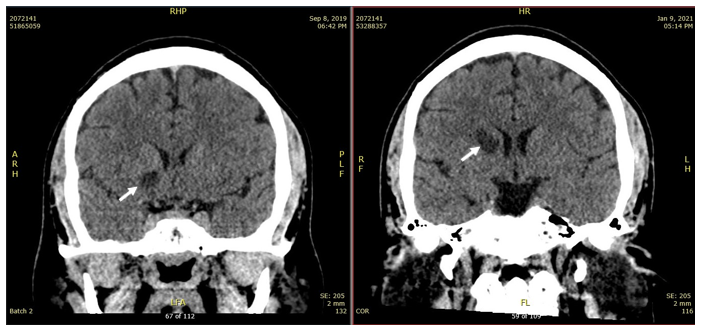
A 32-year-old man presented to the emergency department with sudden onset right-sided facial weakness, numbness, and difficulty with eye closure. His past medical history was significant for poorly-controlled type 2 diabetes mellitus and hypertension, as well as similar presentation to the emergency department with sudden onset right facial weakness in 2013. At the time, a head computed tomography (CT) scan was unremarkable. His symptoms resolved completely within a few hours and the patient was discharged home without further workup. In September 2019, the patient again presented to the emergency department, this time with bilateral facial swelling and weakness. A routine non-contrast head CT showed striatocapsular encephalomalacia (Figure 1).
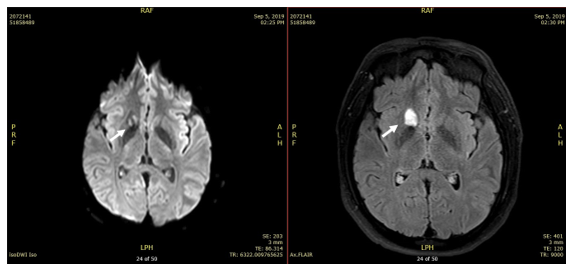
Subsequent magnetic resonance imaging (MRI) showed corresponding diffusion restriction and fluid-attenuated inversion recovery (FLAIR) changes, suggesting a subacute infarct in the right Recurrent Artery of Heubner (RAH) territory (Figure 2).
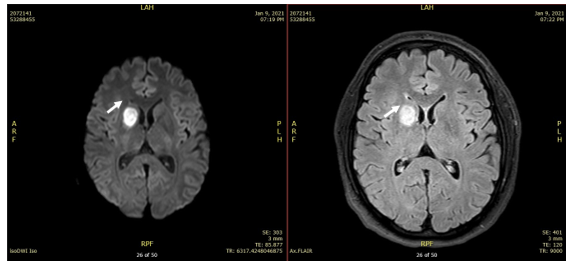
Magnetic resonance angiography (MRA) of the brain and neck was unremarkable.He was discharged on prednisone, valacyclovir for suspected Bell’s palsy, as well as started on aspirin 81mg, atorvastatin, metformin, and antihypertensives for secondary stroke prevention. However, he remained noncompliant with medication use and was lost to follow-up. In January 2021, the patient presented again with sudden onset right sided facial weakness, numbness, and difficulty with eye closure. His glycosylated A1c on arrival was 12.4 and systolic blood pressures were in the 160s. Neurological examination revealed bilateral eye pain without vision loss or diplopia, right sided decreased sensation in the V1, V2 and V3 regions, and right sided upper and lower facial motor weakness. The remainder of the exam was within normal limits and did not identify any left sided deficits. Head CT showed an area of striatocapsular encephalomalacia that was more extensive that the one seen in 2019 (Figure 1). MRI also showed additional areas of diffusion restriction with FLAIR changes, suggesting a second subacute infarct in the same right Recurrent Artery of Heubner territory (Figure 3).
CT angiogram of the head and neck was unremarkable. He was again started on prednisone, valcyclovir, metformin, and anti-hypertensives. He was started on Aspirin 81 daily and Plavix 75 daily for 21 days, with instructions to continue Plavix monotherapy in accordance with the 2013 CHANCE [10] clinical trials. The patient has remained noncompliant with medications and has not responded to two follow-up appointment requests thus far.
Our case describes recurrent infarcts in the Recurrent Artery of Huebner territory, each time presenting with unrelated symptoms of right facial weakness and isolated facial swelling. The MRI in 2019 showed chronic right RAH territory stroke. The location of the infarct does not correspond to the symptoms of ipsilateral facial swelling or weakness [2,5,7-9]. Full metabolic and infectious investigations were unrevealing and the etiology of the facial swelling is not known. This patient’s strokes were considered asymptomatic and were found incidentally when he sought medical care for facial swelling of unknown origin.The etiology of the strokes is most likely due to small vessel disease secondary to uncontrolled diabetes, hypertension, and hyperlipidemia. Given the unremarkable MRA in 2019 and the unremarkable CTA in 2021, the infarct was considered less likely due to large vessel disease or a proximal occlusion, though he did not undergo an angiogram. The exact causes of recurrent strokes are not well understood, but it has been suggested that diabetes, hypertension, and hyperlipidemia increase risk of recurrent strokes [6,1].With asymptomatic stroke, management focuses on modifying risk factors to reduce risk of recurrent stroke. The 2013 CHANCE study [10] and 2017 POINT study [4] investigated the use of dual antiplatelet therapy (DAPT) for secondary prevention after a minor ischemic stroke and revealed a benefit of DAPT for 21 days before continuing with long term therapy with a single antiplatelet agent. SPS3 Investigators suggested a benefit of tight blood pressure control with a systolic blood pressure goal less than 130 compared to 130-149 [11]. After presentation in 2019 this patient was started on aspirin 81 mg. However, despite extensive counseling, he continues to be non-compliant with all medications, placing him at risk for more recurrent lacunar infarcts.There are several limitations of this study, the biggest one being that it is a case report with a sample size of one. Recurrent infarcts in the same vascular territory, without vascular or structural abnormalities, are exceedingly rare. Neuroimaging at the time may incidentally discover these infarcts, though for the most part they may occur unnoticed. Future neuroimaging may be biased towards considering them all as one infarct, though clinicians must always remain aware of the possibility that what they visualize is a culmination of several prior recurrent infarcts in the same vascular distribution. Due to the low sample size, the true incidence of these recurrent infarcts cannot be estimated by this study.
Recurrent infarcts of lacunar arteries, like the recurrent artery of Huebner, are often asymptomatic and missed on imaging. At minimum, a CT-guided angiogram and an MRI should be considered to rule out any vascular or structural abnormalities. If none are present, management should focus on optimization of risk factors of hypertension, diabetes, and others. Dual antiplatelet therapy (DAPT) may be considered in the short term, with Aspirin to follow for life-long secondary stroke prevention.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
