
Case Report | DOI: https://doi.org/10.31579/2641-0419/519
Pediatric Critical Care, Al Qassimi Women and Children Hospital, Emirates Health Services, Sharjah, UAE.
*Corresponding Author: Mahmoud Kamal Moustafa Ahmed, Pediatric Critical Care, Al Qassimi Women and Children Hospital, Emirates Health Services, Sharjah, UAE.
Citation: Moustafa Ahmed MK, Anasalwogud Ahmed, Alddai M. Alnair, Ahmed Ali AH, Elyan Ahmed MS, (2025), Recurrent Cardiac Tamponade as the Initial Presentation of MTO1-Associated Mitochondrial Cardiomyopathy (COXPD10) in a Four-Month-Old Infant: A Case Report, J Clinical Cardiology and Cardiovascular Interventions, 8(14); DOI:10.31579/2641-0419/519
Copyright: © 2025, Mahmoud Kamal Moustafa Ahmed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 August 2025 | Accepted: 24 September 2025 | Published: 30 September 2025
Keywords: mitochondrial disease; mto1; coxpd10; cardiac tamponade; pericardial effusion; hypertrophic cardiomyopathy; infant
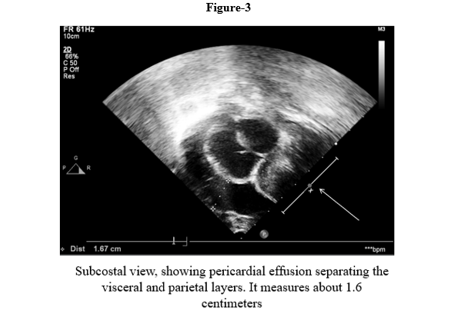
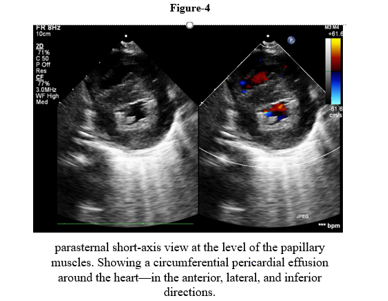
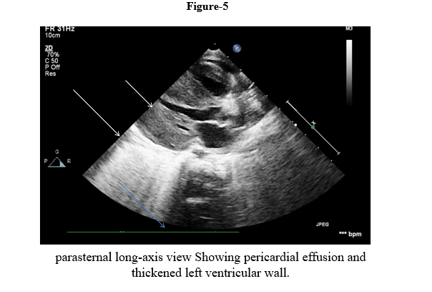
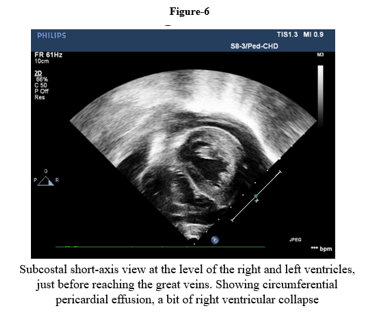
We report a four-month-old girl who presented in sudden cardiorespiratory collapse to illustrate an uncommon cardiac first sign of MTO1-related disease. The infant arrived hypotensive and obtunded with severe metabolic acidosis (pH 6.59; lactate 29 mmol/L). Chest radiograph showed cardiomegaly and bedside echocardiography revealed a large circumferential pericardial effusion producing compression of the right heart together with concentric left-ventricular hypertrophy. Emergency pericardiocentesis drained 120 mL of serous fluid and produced only transient improvement; over a prolonged PICU stay she had recurrent sterile effusions, four failed extubation attempts, refractory lactic acidosis, renal dysfunction and progressive bradycardia. Whole-exome sequencing identified a homozygous pathogenic MTO1 variant (NM_012123.4:c.1232C>T; p. Thr411Ile); both parents were heterozygous carriers. The family history included consanguinity and a sibling who died in early infancy after a similar illness. Despite maximal supportive care, she died on day 40 from cardiogenic shock and multiorgan failure. The case highlights that recurrent sterile pericardial effusion in an infant with hypertrophy and marked hyperlactatemia should prompt consideration of an underlying mitochondrial (MTO1-related) disorder and early genetic testing to guide counselling
Pericardial tamponade is a life-threatening condition in children, with etiologies predominantly including infection, autoimmune disease, renal failure, or malignancy. Infrequently, inborn errors of metabolism, particularly mitochondrial cardiomyopathies, can present with recurrent sterile pericardial effusions. Mutations in the MTO1 gene disrupt the modification of mitochondrial transfer RNA (tRNA), which is critical for the efficient translation of proteins within the mitochondrial respiratory chain. This defect leads to Combined Oxidative Phosphorylation Deficiency 10 (COXPD10) [1, 2].
The clinical phenotype of COXPD10 typically includes severe lactic acidosis, hypertrophic cardiomyopathy, developmental delay, and a generally poor prognosis, especially when presenting in infancy [2–4]. While hypertrophic cardiomyopathy is a well-recognized feature of this disorder, pericardial effusion with tamponade as the primary presenting symptom is exceedingly rare. This case aims to highlight this unusual cardiac manifestation of COXPD10 for cardiologists and intensivists, emphasizing the importance of considering mitochondrial disorders in the differential diagnosis of recurrent sterile effusions in infants.
A 4-month-old girl, born at term by normal vaginal delivery (birth weight 4.2 kg, no neonatal issues), suddenly developed respiratory distress and was found to be unarousable. The parents reported cry for 1 month. There was parental consanguinity and a sister who expired at 3 months with same illness (feeding difficulty, respiratory distress). Two older brothers are healthy. She was shocked with severe acidosis ( pH of 6.59 and lactate of 29 mmol/L) on arrival at the referring hospital. She was intubated and brought to our PICU.
At the referring hospital, she was in shock with severe acidosis (pH 6.59, lactate 29 mmol/L). She was intubated and transferred to our PICU.
Cardiac assessment:
Genetic findings: Whole-exome sequencing showed the presence of a homozygous missense MTO1 variant (NM_012123.4:c.1232C>T; p.Thr411Ile) interpreted as pathogenic. Both parents were heterozygous carriers.

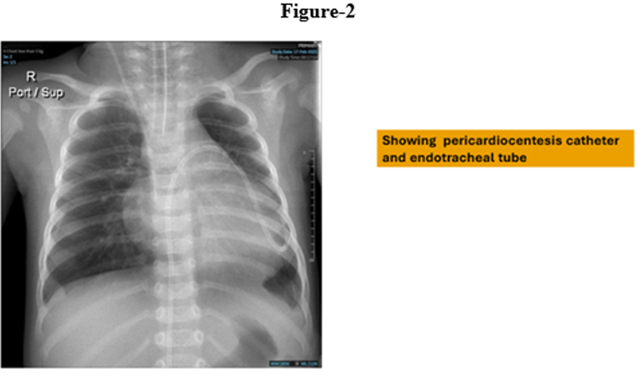
Emergency pericardiocentesis was performed on her with drainage of 120 ml serous fluid. High-dose care included mechanical ventilation, inotropes, repeated bicarbonate infusion and metabolic coenzymatic focus (CoQ10, thiamine, biotin, folinic acid, L-carnitine) [5,6]. Riboflavin and dichloroacetate were also considered but not available [7]. The course was complicated with repeated pericardial effusions, four unsuccessful extubation trials, persistent lactic acidosis, renal failure, and progressive bradycardia. The patient had recurrent tamponade, despite multiple pericardiocenteses. Following multidisciplinary discussion of the dire prognosis and lack of disease-modifying therapy, a DNR was accepted by family. Day 40 she succumbed to cardiogenic shock.
MTO1-related COXPD10 is a rare mitochondrial disorder due to biallelic MTO1 mutations. MTO1 variants cause combined deficiency of respiratory chain, predominantly in complexes I and IV. MTO1 is responsible for mitochondrial protein translation and modification of mitochondrial tRNAs [1,2]. From the clinical point of view, COXPD10 is characterized by lactic acidosis, cardiomyopathy, and neurological disease and has generally a poor outcome [2].
This case illustrates tamponade as the initial cardiac manifestation of COXPD10. In infants, large effusions leading to tamponade should typically give rise to strong concerns for an infected, malignant, autoimmune, or post-surgical cause. Sterile recurrent effusions in addition to hypertrophic cardiomyopathy, in our patient, were suggestive of a metabolic cardiomyopathy.
Cardiomyopathy is a hallmark of COXPD10: O’Byrne et al. reported lactic acidosis in all 35 patients and cardiomyopathy in ~79% [2]. Zhou et al. described an infant with acidosis and early death [3], and Luo et al. reported another with compound heterozygous MTO1 variants and HCM [4]. Our case aligns with this phenotype but our case is distinctive in that it highlights pericardial tamponade as the critical event. The recurring effusions support a role of mitochondrial energetic failure in the development of capillary leak and edema. Within combined oxidative phosphorylation deficiencies, COXPD10 and COXPD23 (GTPBP3 mutations) in the audio-metabolic spectrum, both manifest with life-threatening HCM and acidosis age of onset of 1 year [8]. In contrast, COXPD1 (GFM1) and COXPD4 (TUFM) frequently present with hepatic failure and encephalopathy [9,10]; COXPD7 (C12orf65) has a later onset and symptomatology of neuro-ophthalmologic disease and uncommon cardiac disease [8]. So, in the setting of HCM and a sterile effusion, mitochondrial translation defects, in particular MTO1 and GTPBP3, should be considered by the cardiologist. Pericardiocentesis is life-saving for tamponade, but does not address the etiology, and recurrences occur in over 50%. The so-called mitochondrial contraceptive "cocktail" is widely utilized, though without evidence of aneuropathy efficacy in COXPD10 [2,4]. Dichloroacetate may also decrease lactate temporarily, but does not affect outcome [2,12]. Current approaches therefore do not alter disease course, and aggressive supportive care and counseling are issues of central management.
Our patient’s course—rapid deterioration despite maximal PICU care—is consistent with most reported outcomes of infantile COXPD10 [2–4]. A minority of longer-term survivors exist but usually with profound neurologic and cardiac morbidity [2,8].
Looking forward, emerging strategies aimed at enhancing mitochondrial quality control, such as the activation of Sirtuin 1 (SIRT1) to promote PGC-1α-mediated mitochondrial biogenesis and mitophagy, represent a promising therapeutic avenue for future investigation in severe mitochondrial cardiomyopathies like COXPD10, moving beyond supportive care toward targeted pathway modulation [13].
While longer-term survivors exist, they generally are left with severe neurologic and cardiac morbidity. Cardiac tamponade This case report shows that may be the first event of mitochondrial cardiomyopathy. In patients with HCM and recurrent sterile effusions, this presentation should raise clinical suspicion among the treating cardiologists for a metabolic etiology manifesting as COXPD10. Early genetic testing provides the patient with a specific diagnosis, counseling, and estimation of the recurrence risk. Treatment is supportive, and prognosis remains bleak, emphasizing the critical need for therapies directed at mt tRNA modification.
Ethical Approval and Consent:
The patient's family provided written and verbal consent for publication of the case. All patient identifiers were removed in compliance with confidentiality regulations.
Conflicts of Interest:
The authors declare no conflicts of interest.
Funding:
The research received no financial backing from outside organizations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
