
Case Report | DOI: https://doi.org/10.31579/2690-4861/706
Department of General Surgery, Bartin State Hospital, Turkey
*Corresponding Author: Yüksel Doğan, Department of General Surgery, Bartin State Hospital, Turkey
Citation: Yüksel Doğan, Semra Salimoğlu, Fatma Dikişer, Ekrem Kocatürk, (2025 Rectus Sheath Hematoma Causing Intraperitoneal Hemorrhage: An Atypical Emergency Diagnosis, International Journal of Clinical Case Reports and Reviews, 23(5); DOI:10.31579/2690-4861/706
Copyright: © 2025, Yüksel Doğan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 February 2025 | Accepted: 18 February 2025 | Published: 28 February 2025
Keywords: rectus sheath hematoma; trauma; bleeding
Rectus sheath hematoma (RSH) is a rare but notable cause of abdominal pain, commonly associated with trauma or anticoagulation therapy. It occurs due to the rupture of a branch of the inferior epigastric artery at its attachment to the rectus abdominis muscle, often without effective hemostasis. Diagnosing RSH can be challenging, as it frequently mimics other intra-abdominal conditions. Preoperative identification is uncommon, with most cases diagnosed intraoperatively, and only a limited number of cases reported in the literature. Here, we present the case of a 57-year-old male who developed RSH following blunt trauma to the left lower abdomen caused by a motorbike rim during repair work. The patient reported left lower paraumbilical pain, and intraperitoneal bleeding was confirmed via clinical evaluation and CT imaging. This case highlights the diagnostic complexities of RSH in acute abdominal presentations and emphasizes the importance of thorough examination and imaging for timely diagnosis and management.
Rectus sheath hematoma (RSH) is a rare but increasingly recognized cause of acute abdominal pain, often resulting from blunt trauma or anticoagulation therapy.1 Its incidence appears to be rising with the growing use of anticoagulants. RSH typically arises from the rupture of an epigastric artery or a tear in the rectus abdominis muscle, often triggered by direct trauma 2 or excessive muscle contraction. Despite its rarity, RSH presents significant diagnostic challenges, frequently mimicking critical conditions such as bowel perforation, ruptured aneurysms, or internal bleeding. Early recognition through clinical examination and imaging is vital to avoid misdiagnosis and ensure effective patient care.
A 57-year-old male presented to our emergency department with left-sided lower groin pain and swelling following blunt abdominal trauma
caused by a motorbike rim piece during a repair incident. On examination, his vital signs were stable, including a sodium level of 78 mmol/L, blood pressure of 112/84 mmHg, and oxygen saturation of 95%. A 5 mm laceration was observed in the lower left abdomen, approximately 4 cm from the umbilicus. The patient exhibited localized tenderness and a palpable mass in the left groin without peritoneal irritation signs such as rebound tenderness or guarding.
Laboratory tests revealed an elevated white blood cell count of 15.2 × 10⁹/L (reference: 4-10 × 10⁹/L), C-reactive protein of 28 mg/L (<5>(Figure 1).

Figure 1: Abdominal Pelvic Computed Tomography showing foreign body in left rectus sheath
Initially, the patient’s stable condition warranted observation in the emergency department. However, during monitoring, the patient developed tachycardia. Repeat blood tests revealed a hemoglobin drop to
10.9 g/dL and hematocrit to 31.8%. Follow-up tomography showed a hematoma in the left rectus sheath with evidence of intra-abdominal bleeding (Figure 2). As the patient’s condition worsened, including hypotension, an urgent exploratory laparotomy was performed.

Figure 2: Left Rectus sheath hematoma leaking to intrabdominal on Abdominal Pelvic Computed Tomography.
Intraoperative findings showed intact small intestine, colon, spleen, and other abdominal organs. A large hematoma in the left rectus muscle extended into the peritoneal cavity. Hemostasis was achieved by suturing the bleeding vessels within the rectus muscle. A Jackson-Pratt (JP) drain was placed between the muscle planes, and a silicone drain was positioned in the pelvic region. During surgery, the patient received two units of erythrocyte suspension and one unit of fresh frozen plasma and was transferred to the intensive care unit (ICU) for postoperative monitoring. During the surgery, the foreign body was removed from the sheath hematoma. Postoperatively, hemoglobin dropped to 7.6 g/dL, and hematocrit fell to 22.2%. While the JP drain remained inactive, the pelvic silicone drain collected 500 cc of hemorrhagic fluid. Despite this, the patient remained stable and received further transfusions. A follow-up CT on postoperative day 3 showed regression of the hematoma (Figure 3), The patient gradually improved and remained hemodynamically stable throughout the ICU stay.
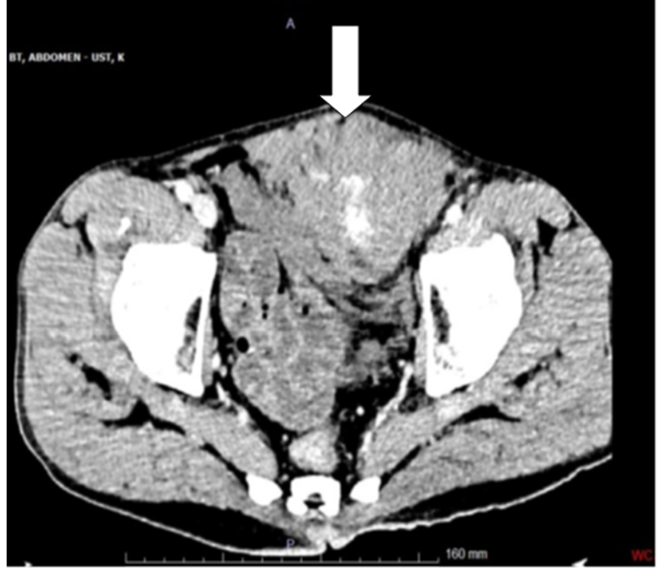
Figure 3: Resolution in Left Rectus sheath hematoma after surgery
Rectus sheath hematoma (RSH), though rare, is a critical cause of acute abdominal pain and often difficult to diagnose in emergencies. It can mimic serious conditions like appendicitis, bowel perforation, or ruptured aneurysm, leading to misdiagnosis or delays in treatment, potentially resulting in poor outcomes.
RSH usually results from ruptured epigastric arteries or tears in the rectus abdominis muscle due to forceful contractions.3 The prevalence of RSH associated with trauma remains low, but it poses significant diagnostic and treatment challenges. While RSH accounts for less than 2% of acute abdominal pain cases, its incidence has increased with the expanded use of oral anticoagulants and non-vitamin K antagonist oral anticoagulants (NOACs). While direct trauma (4 and anticoagulation are known risk factors, RSH can also occur after non-contact exercises, minor movements, or sudden muscle strains.5 Studies show that anticoagulants are involved in up to 70% of RSH case .
A thorough history and focused physical exam help distinguish RSH from other abdominal conditions, avoiding unnecessary surgery. Ultrasound is valuable for bedside assessment, while CT scans offer nearly 100% sensitivity, accurately pinpointing hematoma location.6
In this case, RSH developed after trauma from a motorbike rim during repair, rupturing a branch of the inferior epigastric artery and extending into the peritoneal cavity, causing rare intraperitoneal bleeding. Early diagnosis was challenging due to non-specific symptoms, stable vital signs, and an unremarkable abdominal exam. CT confirmed the diagnosis and revealed intraperitoneal extension, necessitating surgery. Ultrasound is valuable for bedside assessment, while CT scans offer nearly 100% sensitivity, accurately pinpointing hematoma location.7 Intraperitoneal bleeding in RSH often requires surgical intervention, as with this patient.
Diagnosing RSH is difficult due to its rarity and non-specific symptoms, accounting for less than 2% of acute abdominal pain cases. Initial localized pain and swelling in our patient were managed conservatively, but rapid deterioration with tachycardia and hypotension required urgent surgery. 8,9 Imaging, especially CT 10, is crucial for accurate diagnosis, offering high sensitivity and localization.
RSH management depends on hematoma severity and patient stability. Most cases are treated conservatively 11, but surgery is required for instability, large hematomas, or intraperitoneal rupture. 12,13. This case highlights the importance of detailed history, physical exams, and imaging to distinguish RSH, prevent unnecessary surgery, and ensure timely treatment. Intra-abdominal spread: Rare but serious, as in this case. Other reports emphasise complications such as abdominal compartment syndrome or necrosis of the rectus muscle12,13.
Intraoperatively, the hematoma was found to have breached the peritoneum, a rare but serious complication requiring immediate hemostatic intervention. Surgical exploration is typically reserved for cases with significant hemodynamic instability or imaging indicating active bleeding, as in this patient. RSH management depends on hematoma severity, patient stability, and ongoing bleeding. Conservative measures, like observation and transfusions, may be sufficient in stable cases. However, in this instance, the patient's tachycardia, hypotension, and significant hemoglobin drop necessitatedsurgical intervention to prevent further hemorrhage and ensure survival. Postoperatively, the patient experienced a persistent but regressing hematoma, as seen on the followup CT scan. This case highlights the need for close monitoring after surgery, as RSH patients can face delayed complications like hematoma reaccumulation, infection, or abdominal compartment syndrome. The patient remained hemodynamically stable with appropriate transfusions and intensive care support, and minimal drainage from the JP drain indicated effective hemostasis in the rectus sheath regio.
This case underscores the need for a high suspicion of RSH in patients with abdominal pain and a trauma history, especially with anticoagulation or other risk factors. Timely imaging and intervention can avert severe complications like intraperitoneal bleeding. It also highlights the importance of careful monitoring in stable patients, as sudden clinical deterioration can occur. The patient was monitored in the ICU, and on postoperative day 3, a follow-up CT scan showed regression of the rectus muscle hematoma(Figure 3), though it had not fully resolved. Throughout the ICU stay, the patient remained hemodynamically stable and showed gradual improvement. This case intersects with other specialties like radiology, hematology, or critical care, and underscores the need for high suspicion of RSH in trauma cases, timely intervention to prevent complications, and vigilant monitoring during recovery. The need for protocols to diagnose and manage atypical RSH presentations and further investigation are recommended. When deciding between surgery and conservative treatment for rectus sheath hematoma (RSH), patient stability and the extent of bleeding are key factors:
Conservative treatment is preferred in hemodynamically stable patients with no evidence of active bleeding or significant hematoma progression. Management includes observation, analgesics, and possible blood transfusions.
Surgery is indicated in cases with hemodynamic instability, ongoing bleeding, large or expanding hematomas, or intraperitoneal extension.
In this case, surgery became essential due to worsening tachycardia, hypotension, and significant hemoglobin drop, emphasizing timely intervention to prevent life-threatening complications. Written informed consent was obtained from the patient.
There are many publications and case reports on rectus sheath hematoma but very rare in combination with intraperitoneal hemorrhage, this case underscores that rectus sheath hematoma (RSH), though rare, should be considered in the differential diagnosis of acute abdomen in patients with trauma or anticoagulationhistory. Early diagnosis and timely intervention-either conservative or surgical-are essential forimproving outcomes and preventing serious complications. Ongoing awareness and documentation of RSH cases are vital for optimizing management strategies
Informed Consent
The patient was monitored in the ICU, and on postoperative day 3, a follow-up CT scan showed regression of the rectus muscle hematoma (Picture2b), though it had not fully resolved. Throughout the ICU stay, the patient remained hemodynamically stable and showed gradual improvement.
Written informed consent was obtained from the patient.
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed. A signed consent form is available from the authors.
Presentation(s) or Awards at a meeting: NO
NO
None declared.
None.
SS,EK: Data collection, data improvement, original draft writing, review writing, and editing, final approval. FD, YD: Data collection, software, data improvement, review writing and editing, and final approval. Each authors have approved the submitted version (and any substantially modified versionthat involves the author's contribution to the study);
Each authors have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. X(TWİTTER) @drydogan49
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
