
Research Article | DOI: https://doi.org/10.31579/2693-7247/212
1Head Medical affairs Indoco Remedies Mumbai.
2MD. Diabetologist, Akshay Hospital, Erandwane, Pune.
3Medical Advisor Indoco Remedies Mumbai.
*Corresponding Author: Abhijit Trailokya, Head Medical affairs Indoco Remedies Mumbai.
Citation: Abhijit Trailokya, Suhas Gopal Erande, Amar Shirsat, (2024), Real world evidence of Alogliptin on the continuous glucose monitoring in Indian type II diabetes mellitus patients in a retrospective, observational case-based studies, J. Pharmaceutics and Pharmacology Research, 7(10); DOI:10.31579/2693-7247/212
Copyright: © 2024, Abhijit Trailokya. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 August 2024 | Accepted: 30 August 2024 | Published: 03 September 2024
Keywords: CGM; time in range; time above range; time below range; HbA1c; Alogliptin CGM; time in range; time above range; time below range; HbA1c; Alogliptin
Aim: To determine the safety and efficacy of Alogliptin on parameters of continuous glucose monitoring (CGM) in type 2 diabetes mellitus (T2DM) patients in a retrospective, observational, real-world settings.
Materials and Methods: Two patients (Case 1 and Case 2) with T2DM from a single center in India who received Alogliptin as a add on therapy to existing oral antidiabetic drugs (OADs) were retrospectively analyzed in the study. CGM was done approximately two weeks prior to the addition of Alogliptin and repeated again after three weeks of adding Alogliptin to the existing OADs for a period of 15 days. Average glucose level, percentage time in target range (70-180 mg/dl), percentage time above target and percentage time below target were determined before and after adding Alogliptin to the existing treatment regimen.
Results:
After addition of Alogliptin 25mg to existing anti-diabetic drugs, there was a reduction in the average blood glucose level from 196 mg/dl to 149 mg/dl in case 1 and from 158mg/dl to 125mg/dl in case 2 after approximately five weeks. Improvement was seen in the percentage time in target range (70-180mg/dl) from 45% to 75% in case 1 and from 67% to 91% in case 2 after approximately five weeks of adding Alogliptin to existing OADs. Percentage time above target decreased from 55% to 23% in case 1 and from 32% to 7% in case 2 after five weeks of adding Alogliptin to existing OADs. Also, there was a reduction in HbA1c from 8.8% to 8.3% in case 1 and from 8.4% to 7.2% in case 2 after a period of five weeks of Alogliptin addition to the existing antidiabetic regimen.
Conclusion: Alogliptin was found to be effective in reducing glycemic fluctuations in patients who were uncontrolled on other oral anti-diabetic medications. There were improvements in CGM parameters like increase in percentage (%) time in Target range (70-180 mg/dl) and decrease in percentage (%) time above target range after adding Alogliptin to the existing anti-diabetic medications.
Diabetes mellitus is a chronic condition causing metabolic derangement and is characterized by hyperglycemia which is persistent. Chronic hyperglycemia can lead to microvascular complications like retinopathy, nephropathy, and neuropathy and macrovascular complications which increases the risk of cardiovascular diseases by several folds.1 In the patients suffering from T2DM the primary predictor for the development and progression of microvascular complications remains the HbA1c levels. The recent evidences suggest an association in the diabetes related microvascular complications and the time in range (TIR).2 Recent clinical data indicate that glycemic variability (GV) is associated with increased risk of hypoglycemia, microvascular and macrovascular complications, and mortality in patients with diabetes, independent of glycated hemoglobin level. The use of continuous glucose monitoring device has markedly improved the assessment of GV in clinical practice and facilitated the assessment of GV as well as hypoglycemia and hyperglycemia events in patients with diabetes.3
Incretin-based therapies are one of the preferred oral antidiabetic agents in the management of type 2 diabetes due to lower incidence of hypoglycemia and weight-neutral or weight losing potential of these drugs. Alogliptin is a highly selective DPP-4i approved by USFDA/ EU (2013), DCGI (2014) to improve glycemic control along with diet and exercise in T2DM.4 Alogliptin has the time to maximum concentration (Tmax) of 1-2 hours with a half-life (t1/2)of ~ 21 hours and bioavailability of 100%. Alogliptin has a long intrinsic half-life (21 hours) and therefore it is eliminated slowly, and has a sustained DPP-4 inhibition (≥ 75$ hours post dose) facilitating convenient once daily dosage (OD)(25mg OD).5 Alogliptin is 100,000 fold more selective for DPP-4 than other related enzymes like DPP-8 and DPP-9.6 In Asian patients, Alogliptin reported a higher efficacy and good tolerability, as compared to Non-Asian patients with diabetes mellitus.7
The objective of this study was to determine safety and efficacy of Alogliptin through continuous glucose monitoring (CGM) in patients with T2DM in a retrospective observational case based studies.
The baseline characteristics of the two Indian patients with type 2 diabetes included in this study are summarized in Table 1. Data of the two patients who received Alogliptin as routine clinical practice in management of T2DM was analyzed retrospectively from the single center. Data was collected from the past medical records of these two patients. Free Style Librepro 1.0.6 was used for CGM. CGM was done approximately two weeks prior to addition of Alogliptin and repeated again after three weeks of adding Alogliptin to existing OADs for a period of 15 days. Average blood glucose level, Percentage time in target range (70-180mg/dl), Percentage time above target and Percentage time below target were determined prior to and after addition of Alogliptin to the existing antidiabetic treatment regimen.
| Demographic parameter | Case no 1 | Case no 2 |
| Age | 54 years | 32 years |
| Sex | Female | Male |
| Fasting blood glucose (mg/dl) | 162 | 111 |
| Post prandial blood glucose (mg/dl) | 189 | 148 |
| HbA1c % | 8.8 | 8.4 |
Table 1: Baseline Characteristic of the patients
Result:
In case 1, there was a reduction in the average blood glucose level from 196mg/dl to 149 mg/dl after five weeks of adding Alogliptin to the existing antidiabetic treatment regimen. (figure 1A). The percentage time in target range (70-180 mg/dl) increased from 45% to 75%, percentage time above target decreased from 55% to 23% (refer table 2, figure 2A, 2B, 3A and 3B) after adding Alogliptin 25mg to the existing antidiabetic treatment regimen. HbA1c was reduced from 8.8% to 8.3% (fig 6A) after five weeks of Alogliptin addition to the existing antidiabetic therapy. The percentage time below target was 0% and 2%, before and after addition of Alogliptin to existing therapy respectively (after five weeks). (refer table 2,3, figure 2A, 2B, 4A,4B.)
In case 2, there was a reduction in average blood glucose level from 158 mg/dl to 125mg/dl after five weeks of adding Alogliptin to existing OADs (figure 1B). The percentage time in target range (70-180 mg/dl) increased from 67% to 91%, percentage time above target decreased from 32% to 7% (refer table 3, figure 4A, 4B, 5A, 5B) after adding Alogliptin 25mg to the existing antidiabetic treatment regimen. HbA1c was reduced from 8.4% to 7.2% (refer figure 6B) in case 2 after five weeks of add on therapy of Alogliptin addition to the existing antidiabetic therapy. The percentage time below target was 1% and 2%, before and after addition of Alogliptin to existing therapy respectively (after five weeks). (Refer table 2,3, figure 2A, 2B, 4A,4B.) There were no episodes of hypoglycemia noted in both patients during this five weeks study period. This retrospective data demonstrated the efficacy of Alogliptin after addition to existing therapy in terms of improvement in glycemic variability.
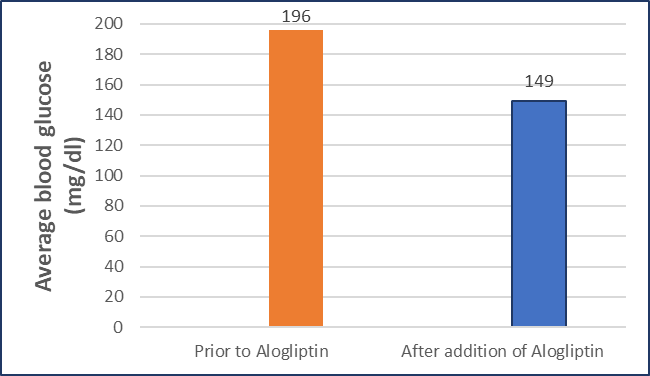
Figure 1 A: Average blood glucose prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy in Case 1
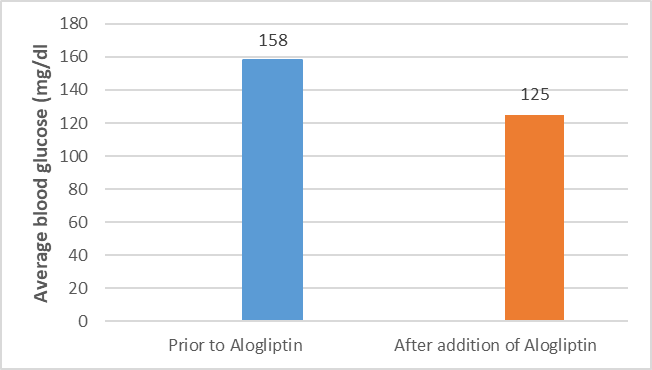
Figure 1 B: Average blood glucose prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy in Case 2
| Case no 1 | Prior to Alogliptin | After addition of Alogliptin (after five weeks) |
| Time in range | 45% | 75% |
| Time below range | 0% | 2% |
| Time above range | 55% | 23% |
Table 2: Time in range, Time below range and Time above range prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy in Case 1
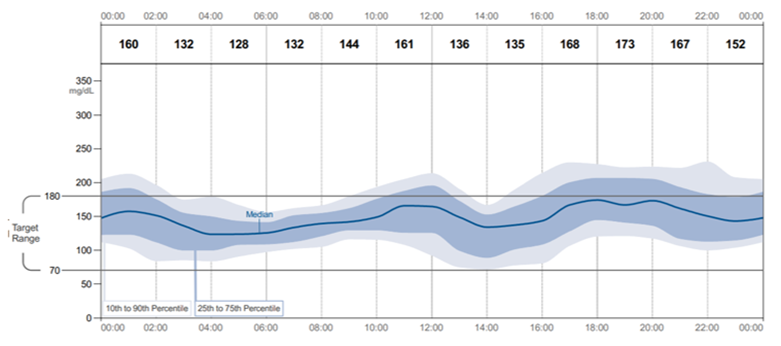
Figure 2: CGM data of case 1 prior to Alogliptin and after addition of Alogliptin (for 15 days) to the existing therapy
Figure 2A: CGM data (14 days) of case 1 prior to treatment with Alogliptin
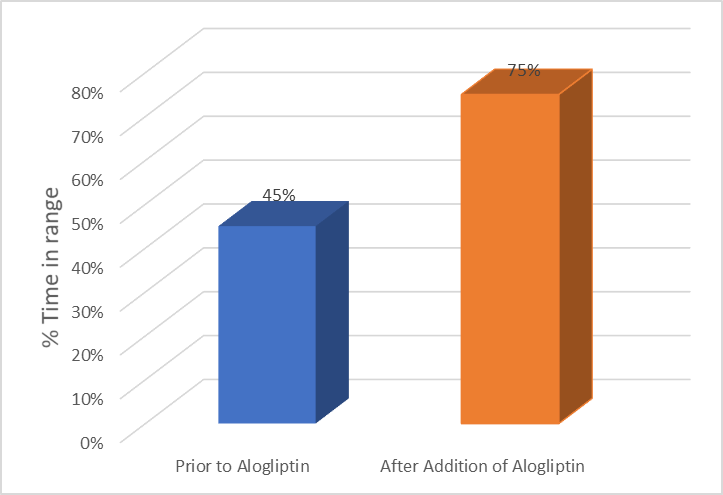
Figure 3: Percentage (%) time in range and Percentage (%) time above range with CGM data in Case 1 prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy
Figure 3A: Percentage (%) Time in range in case 1 prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy
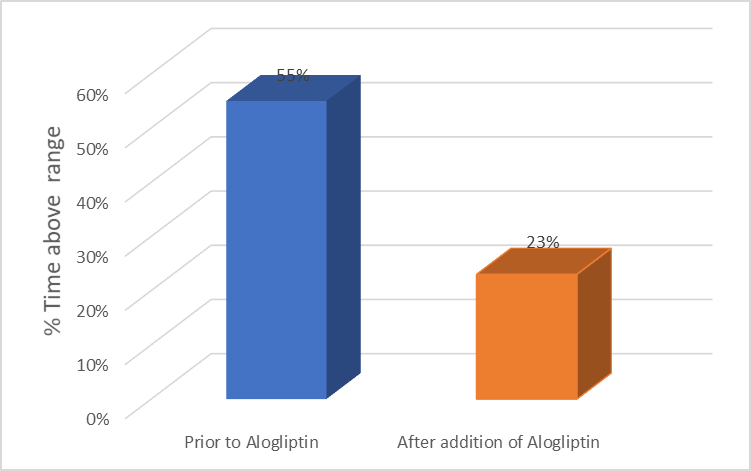
Figure 3B: Percentage (%) Time above range in case 1 prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy
| Parameter | Prior to Alogliptin | After addition of Alogliptin (after five weeks) |
| Time in range | 67% | 91% |
| Time below range | 1% | 2% |
| Time above range | 32% | 7% |
Table 3: Time in range, Time below range and Time above range prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy in Case 2
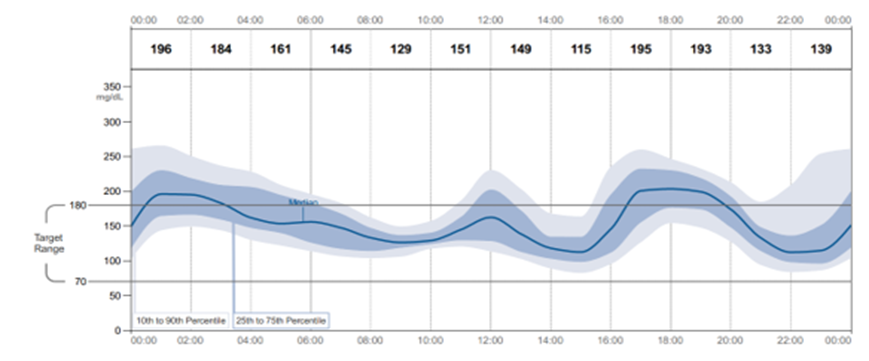
Figure 4: CGM data of case 1 prior to Alogliptin and after addition of Alogliptin to the existing therapy (for 15 days)
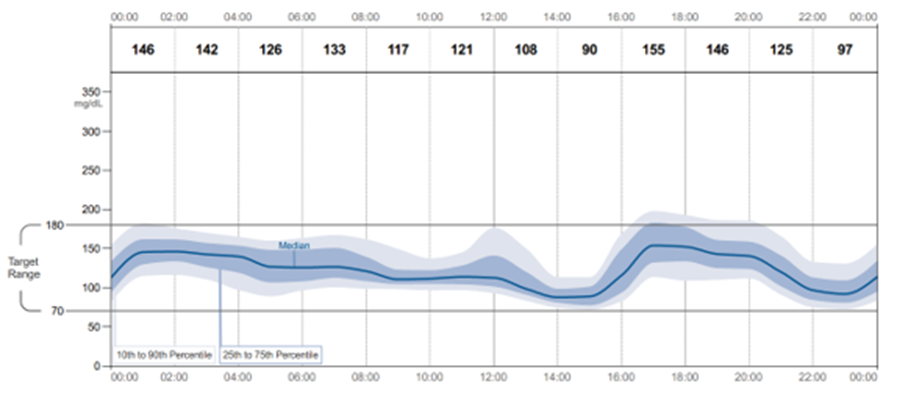
Figure 4A : CGM data of case 2 prior to treatment with Alogliptin (for 14 days)
Fig 4B: CGM data of case 2 after addition of Alogliptin (for 15 days) to the existing therapy
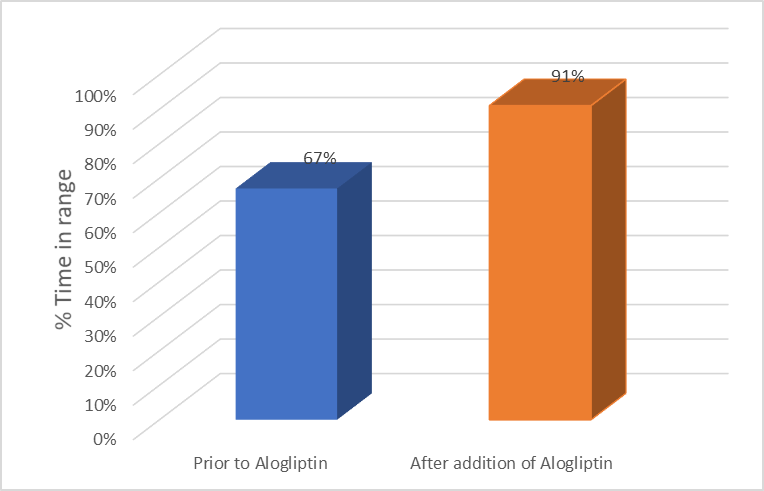
Figure 5 : Change in Percentage (%) time in range and Percentage (%) time above range with CGM data in Case 2 prior to Alogliptin and after five weeks of addition of Alogliptin to the existing therapy
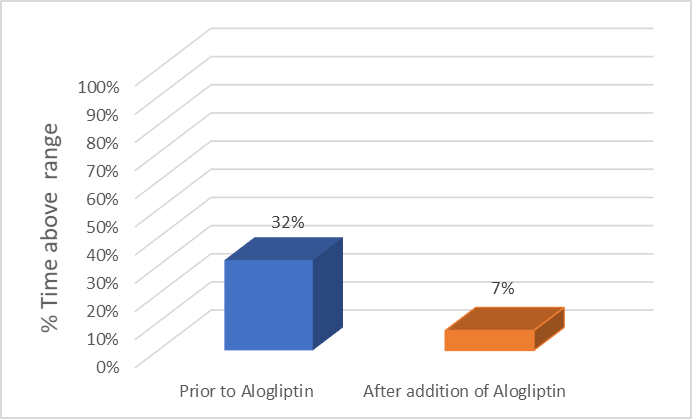
Figure 5A: Percentage (%) Time in range in case 2 prior to Alogliptin and after five weeks of addition of Alogliptin to existing therapy
Figure 5B: Percentage (%) Time above range in case 2 prior to Alogliptin and after five weeks of addition of Alogliptin to existing therapy
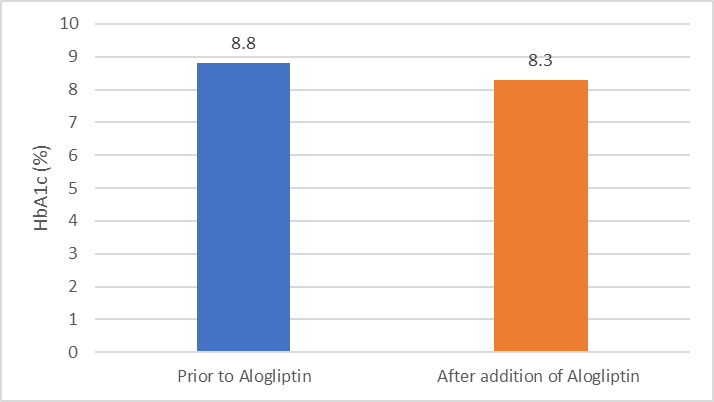
Figure 6: Change in HbA1c % prior to Alogliptin and after five weeks of addition of Alogliptin to existing therapy in Case 1 and 2
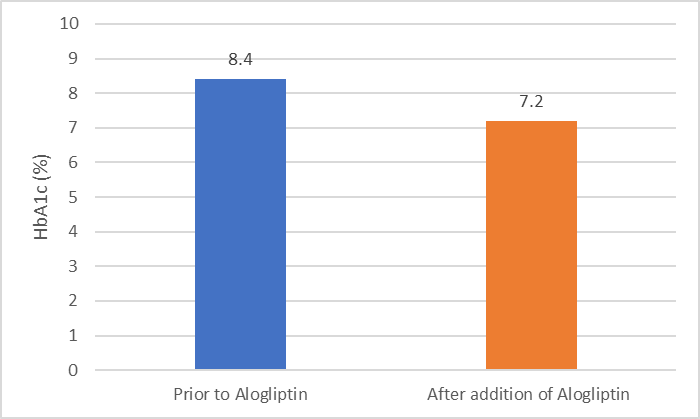
Figure 6A: Change in HbA1c % prior to Alogliptin and after five weeks of addition of Alogliptin to existing therapy in Case 1
Figure 6B: Change in HbA1c % prior to Alogliptin and after five weeks of addition of Alogliptin to existing therapy in Case 2
HbA1c realistically captures the average glycemic control in the retrospect, it is limited in assessing short-term outcomes and day-to-day glucose fluctuations. CGM devices provide a broad spectrum of additional glucose management metrics, including proportions of time in range (TIR), time below range (TBR), time above range (TAR), and glucose variability (GV).
The principal goal for all children and adults with type 1 diabetes and type 2 diabetes is to maintain:- At least 70% of TIR (70–180 mg/dL / 3.9–10 mmol/L), while at the same time minimizing both TBR and TAR: - less than 4% (1 h per d) of TBR (< 70> 180 mg/dL / 10 mmol/L). Targets should be individualized and in line with personal needs and circumstances. Each incremental 5% improvement in TIR is associated with clinically significant benefit.
Various studies have shown that frequent or large glucose fluctuations may lead to diabetes-related complications especially increased cardiovascular (CV) events due to the postprandial spikes in the blood glucose level as well as hypoglycemic events8. Strict HbA1c control alone is insufficient for preventing diabetes related complications, particularly the CV events caused by the long-term high GV. DPP4 inhibitors have the potential to improve glycemic control and to reduce glucose fluctuations, by increasing the active serum GLP-1 and GIP concentrations via glucose-dependent insulin secretion9. In a long term study of about 3.5 years in Japanese T2DM patients by Takebayashi K et al, it was found that Alogliptin once daily along with other OADs demonstrated a significant reduction in HbA1c (p = 0.0001)10. In another study by Kishimoto M et al it was observed that Alogliptin alone as well as in combination with Metformin reduced glycemic fluctuation in patients with T2DM11. In the present study, the administration of Alogliptin to existing anti-diabetic drugs decreased average blood glucose levels and reduced GV to a similar extent in patients with T2DM, as seen with improvement in percentage time in target range, percentage time above range and reduction in HbA1c after five weeks. There was no documented symptomatic hypoglycaemia during the study period of five weeks. This retrospective data demonstrated the efficacy of Alogliptin after addition to existing therapy in terms of improvement in glycemic variability.
In Indian T2DM patients inadequately controlled on other oral anti-diabetic drugs, co-administration of Alogliptin reduced glycemic fluctuations without any episodes of hypoglycemia. There were improvement in CGM parameters resulting in an increase in percentage (%) time in target range (70-180mg/dl) and decrease in percentage (%) time above target range due to addition of Alogliptin to existing OADs. Also the reduction in average blood glucose and HbA1c were seen in these patients after addition of Alogliptin to the existing antidiabetic regimen. This retrospective data demonstrated the efficacy of Alogliptin after addition to existing therapy in terms of improvement in glycemic variability.
Limitation of the study was it was a retrospective, observational data obtained from a small number of case based studies. Further studies with larger numbers of patients at multiple sites are necessary to provide a more complete understanding of the improvement in glycemic parameters in T2DM patients due to Alogliptin.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
