
Mini Review | DOI: https://doi.org/10.31579/2641-8975/003
*Corresponding Author: Sanjay Chatterjee, MD Consultant Diabetologist, Apollo Gleneagles Hospital, Kolkata, India.
Citation: Sanjay Chatterjee, Majumder A, Ray S and Bhattacharjee K, Real Time Clinical Safety and Effectiveness of Long Term Use of Saroglitazar in Indian Patients with Diabetic Dyslipidemia Having Abnormal Metabolic Parameters. J Diabetes and Islet Biology, DOI: 10.31579/2641-8975/003
Copyright: © 2018 Sanjay Chatterjee. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 December 2018 | Accepted: 21 December 2018 | Published: 27 December 2018
Keywords: Keywords
Abstract
Indian patients with type 2 diabetes (T2DM) usually suffer from multiple metabolic abnormalities, such as overweight, obesity, high triglycerides (TG), low HDL-C, increased blood pressure, along with insulin resistance. In India, Saroglitazar is being used in the management of diabetic dyslipidemia since 2013. Randomized controlled clinical trials of Saroglitazar (PRESS V & PRESS VI studies) 1, 2 have established safety and efficacy of Saroglitazar in T2DM patients with dyslipidemia. But the question is “What is the real time clinical safety and effectiveness of Saroglitazar in Diabetic dyslipidemia, if it is used for more than a year?
Review scope: This article reviews the observational study and retrospective analysis of 58 weeks safety and effectiveness data of Saroglitazar in Indian patients having diabetic dyslipidemia [3].
Objective of this review: Phase III randomized controlled clinical trials of Saroglitazar have evaluated the safety and efficacy of this drug for 12-24 weeks follow-up [1, 2]. Previously published post-marketing studies evaluating the clinical safety and effectiveness of Saroglitazar in diabetic dyslipidemia had a shorter duration of follow-up (less than 1 year) [4-6]. We conducted a retrospective analysis of safety and effectiveness data of Saroglitazar 4 mg once daily in Indian patients with T2DM, having metabolic abnormalities (like high TG and low HDL). This analysis included the data from the patients with a mean follow-up duration of 58 weeks [3]. The main objective of this retrospective analysis was to evaluate long-term safety and effectiveness of Saroglitazar in diabetic dyslipidemia.
Methods: We identified 158 patients having type 2 diabetes and dyslipidemia (TG >150 mg/dl) who had been prescribed Saroglitazar 4 mg once daily as per the prescribing information and the follow-up results were available for 58 weeks duration. Data of only those patients were considered for final evaluation having both baseline and follow-up values of fasting plasma glucose (FPG), post-prandial plasma glucose (PPPG), glycated hemoglobin (HbA1c) and lipid profile. Descriptive data analytics has been carried out in the present study and were analyzed by appropriate statistical tests. A p value of <0.05 was considered as statistically significant.
A total of 158 patients’ data was analyzed in this observational study with variable co-morbidities and all were T2DM patients, with high TG (TG>150 mg/dl). A total of 53.16% patients were overweight/ obese and 58.86% patients were hypertensive. After 58 weeks, the mean blood pressure was significantly reduced, both systolic (-4 mmhg, P= 0.004) and diastolic (-2 mmhg, P=0.001).
At end of 58 weeks, metabolic parameters like TG, TC, LDL-C, FPG, PPPG, HbA1c, non HDL-C were reduced significantly from baseline (Table). Significant drop in non HDL-C may have beneficial impact on residual CV risk, while a reduction of both triglyceride and TG/HDL ratio makes a shift of the small dense LDL particles to more buoyant and larger LDL particles which are less atherogenic.
Regarding safety analysis, Saroglitazar was to be found safe without having any major/serious adverse events during 58 weeks of therapy. Liver enzymes ALT and AST were both reduced from baseline, the ALT reduction at 58 weeks was found to be statistically significant (P<0.001). Serum creatinine level was not adversely affected during this observational study. The change in body weight at 58 wees follow-up was found to be statistically significant (increased from 70.61 kg at baseline to 71.69 kg at 58 weeks; p=0.002) in this retrospective analysis.
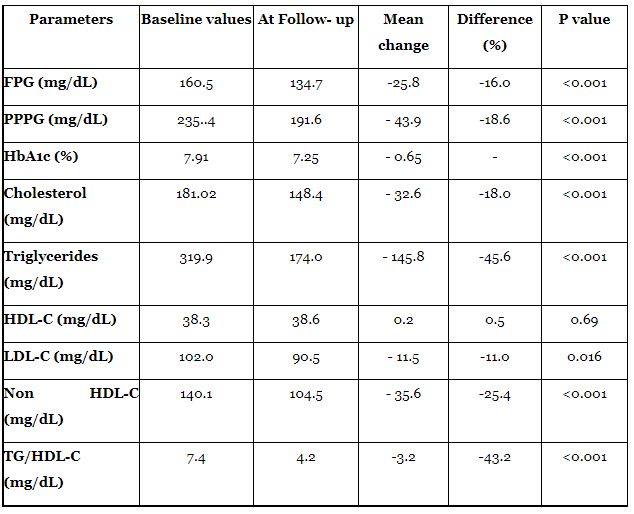
HDL-C: High density lipid cholesterol, LDL-C: Low density lipid cholesterol, TG: Triglyceride, FPG: Fasting plasma glucose, PPPG: Post-prandial plasma glucose, HbA1c: glycated hemoglobin
High TG is considerably associated with diabetes mellitus and it is of utmost importance to reduce TG when it is more than >200 mg/dl. The results of this analysis showed that 58 weeks use of Saroglitazar significantly improves the metabolic abnormalities (lipids and glycemic parameters) in Indian diabetic patients with good safety and tolerability profile.
Various recently published large observational and epidemiological studies have strongly established the positive association of High TG (>150 mg/dl) with elevated CV risk [7-9].
The results from 22 year follow-up of the Bezafibrate Infarction Prevention (BIP) study and registry showed that in patients with established CHD, the increased levels of serum triglycerides (TG> 500mg/dL) is associated with a long-term increased risk of mortality by 68% [7]. The results from Strong Heart Study established that in American Indian patients with high TG (>150 mg/dL), Diabetes and low HDL had 54% increased risk of CHD and 2.13 times higher risk of stroke compared to diabetic patients with normal TG and HDL values [8]. So management of high TG is important and as per guidelines recommendations, statins are first line therapy while non-statin TG lowering therapies (Saroglitazar, Fibrates, Niacin, Omega-3 fatty acid) may be considered as add on therapy only in those high risk patients who do not achieve their lipid targets (TG and non HDL-C) in spite of optimal statin therapy.
Studies have also established that even mild to moderate elevation of TG levels are associated with significant increase in the risk of acute pancreatitis [10]. The latest consensus statement by American Association of Clinical Endocrinologists and American College of Endocrinology (AACE/ACE) advocates reducing triglyceride levels when severely elevated (>500 mg/dL) to prevent pancreatitis [11].
Saroglitazar is a dual PPAR α and γ agonist approved in India for the treatment of hypertriglyceridemia in patients with T2DM uncontrolled with statin therapy. In two phase 3 trials, Saroglitazar 4 mg once daily showed significant decrease in triglyceride levels (-45 to 46.7%), non HDL-C (-32.5%) and HbA1c (-0.3%) with better safety and tolerability profile over the period of 12-24 weeks follow-up[1, 2]. In one Indian post-marketing, observational study, at 3 months follow-up, Saroglitazar 4 mg led to significant reduction in TG (-35.8%), LDL-C (-16.4%), total cholesterol (-19%), non HDL-C (-23.4%) and significant 0.9% absolute reduction in HbA1c (As an add on to anti-diabetic medications) with no serious adverse events reported [4].
A part of Chatterjee S et al 2018 study of 158 patients with follow-up of 58 weeks is a continuation of earlier published data with follow-up data of only 34 patients for a period of 14 weeks [3, 5]. In 58 weeks follow-up study, it was observed that Saroglitazar 4 mg significantly improves various metabolic parameters (lipid and glycemic parameters) along with favorable effects on serum ALT level and no significant change in serum creatinine level. These 58 weeks follow-up results are in consistent with previous 14 weeks and 40 weeks observational data analysis [5, 6]. Unlike previous observations (of no weight gain associated with Saroglitazar), in this study with much longer duration, the weight-gain has reached a level of statistical significance. However, it should be noted that many patients were on sulfonylureas and/or insulin, which are known to cause weight gain; hence the weight-gain cannot be solely attributable to Saroglitazar alone.
Unique strength of this study is long duration of therapy of 58 weeks but lack of vigilance of control group and small sample size (158 patients) are limitations of it. Larger and more comprehensive randomized controlled clinical trials are required to establish and further validate these findings.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
