
Case Report | DOI: https://doi.org/10.31579/2690-8808/165
1 Cardiovascular Surgeon-Hospital G. A. Dr. Cosme Argerich, CABA. Professor of Medicine. Specialist in Phlebology (UBA).
2 General Surgeon (MAAC)-Hospital G. A. Dr. Teodoro Álvarez, CABA. Phlebology and Lymphology (UCA).
3 Cardiovascular Surgeon- Hospital G. A. Dr. Cosme Argerich, CABA. Deputy Director of the Specialization Program in Cardiovascular Surgery, Argerich Site, School of Medicine of the University of Buenos Aires. Specialist in Phlebology and Lymphology (UCA).
*Corresponding Author: Paola Belsito Malaspina, Cardiovascular Surgeon- Hospital G. A. Dr. Cosme Argerich, CABA. Deputy Director of the Specialization Program in Cardiovascular Surgery, Argerich Site, School of Medicine of the University of Buenos Aires. Specialist in Phlebolog
Citation: Yamil N. Ponce, Sandra P. Raznovich, Paola Belsito Malaspina, (2023), Unique Approach to Management of Hypertrophic Obstructive Cardiomyopathy within a Resource-Limited Hospital. J, Clinical Case Reports and Studies, 4(3); DOI:10.31579/2690-8808/165
Copyright: © 2023 Paola Belsito Malaspina, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 February 2023 | Accepted: 10 February 2023 | Published: 20 February 2023
Keywords: pseudoaneurysm; brachial artery; thrombin injection
With the increased use of endovascular procedures, a rise in the number of cases of pseudoaneurysms has been seen. They have a low incidence, being its etiology traumatic or iatrogenic. Potential complications are edema, pain, hemorrhage and ischemia of the affected limb, which can even lead to loss of the fingers.
We report a clinical case of a patient with brachial artery pseudoaneurysm after coronary angioplasty, which was resolved with Doppler ultrasound- guided puncture with thrombin injection.
Pseudoaneurysms or false arterial aneurisms are defined as cavities in which a rupture of the vascular wall permits blood extravasation, which leads to pulsatile hematoma [1]. Said hematoma is surrounded by a pseudo-sac formed by adjoining tissues, which means that this pseudo-sac is not formed by elements of the vascular wall. Its etiology can be infectious, traumatic [1] or iatrogenic. The latter has seen an increase given the advances in interventional medicine with increased use of diagnostic and therapeutic methods.
An incidence of post-puncture complications has been described, ranging from 0.2 to 7% [2], whereas other studies report up to 9%. Pseudoaneurysm accounts for 1.5% of post-angiography complications and up to 6% of post therapeutic procedures complications [3].
It is well known that brachial artery pseudoaneurysms have a low incidence, although it has increased in recent years as a result of the greater use of upper limbs in endovascular procedures. Given their potential complications, i.e. hemorrhage, edema, pain, limb ischemia, pseudoaneurysms must be treated promptly.
We report a clinical case of brachial artery pseudoaneurysm diagnosed by doppler ultrasound and treated with ultrasound-guided thrombin injection. The study allowed for early diagnosis and satisfactory treatment, reducing morbidity as it is a method that does not require the use of nephrotoxic contrast agents or radiation, allowing for real time evaluation and reducing hospitalization time and related costs.
Male, 69 year-old patient, with a history of coronary angioplasty of 7 days of evolution. The approach pathway was the brachial artery of the right upper limb. Ecodoppler was performed, diagnosing brachial artery pseudoaneurysm (Figure 1). It was decided to attempt to compress it on two occasions, not obtaining the expected result.
The ecodoppler revealed a patent brachial artery, with preserved flow pattern and the presence of a 15.8 mm diameter pseudoaneurysm with the typical ying-yang pattern, patent 2.4 mm diameter and 11 mm long neck, with a high-speed and resistance flow pattern.
Thrombin was injected in the bottom of the sac with the aim of thrombosing, not reaching the neck in order to avoid migration of the product as it might cause arterial thrombosis. Being this a real-time procedure, once thrombosis in the sac was observed it was decided not to continue injecting thrombin although the neck remained patent, since as there is no cavity to receive the blood, the neck would thrombose. In order to prove that this was the case, the patient was seen at 24 hours for ecodoppler control (Figure 2). Neck and pseudoaneurysm sac thrombosis was observed. Even so, the patient was seen for a second control with ecodoppler 7 days after the procedure, evidencing complete exclusion of the pseudoaneurysm.
Brachial artery pseudoaneurysms are infrequent but, given their potential complications, they are considered a vascular emergency.
Treatments range from a watch and wait approach, manual compression, endovascular procedures to conventional surgery. Endovascular procedures with stent placement use nephrotoxic iodine agents that also imply a high cost, whereas conventional surgery requires anesthesia and hospitalization.
Thrombin injection has proven to be effective and does not require iodine contrast agents or anesthetics, does not expose the patient to radiation, can be administered in an outpatient procedure with few hours of stay in the medical center and allows for arterial hemodynamic control of the treated limb. This method also makes it possible to prove effectiveness of the procedure and arterial patency in real time and, finally, it also reduces treatment costs [3].
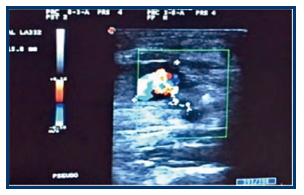
Figure 1. Pseudoaneurysm. Measurement of the cavity, neck diameter and length and jet speed

Figure 2. Obliteration of the sac, control 24 hours after the procedure.
Vascular ecodoppler is a fundamental diagnostic tool (94% to 97% sensitivity) [4]. It permits evaluation of the lesion features (number of cavities, dimension, presence of thrombi, internal septa), the relation with neighboring structures, study of the arterial tree (walls and flows) and the presence of thrombi in vascular structures. With this method it is possible to establish differential diagnosis, namely: true aneurysm, hematoma, arteriovenous fistula, lipoma, neoplasia or abscesses. On the other hand, it is a low cost, reproducible method that can be performed on the bed side, not using radiation or nephrotoxic contrast media. It has been proven that ultrasound-guided percutaneous thrombin injection is safe and efficacious [5,6].
It must be noted that when an endovascular procedure is required, it is necessary to consider that there are predisposing factors for the development of an aneurysm, including anticoagulation, age older than 60, use of larger diameter catheters, obesity, non-effective compression in the puncture site or technical errors during the procedure.
We conclude that ecodoppler is a fundamental tool in the diagnosis and treatment of vascular procedures.
The authors have no disclosures to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
