
Research Article | DOI: https://doi.org/10.31579/2641-0419/110
1 Director of research, The Heart and Vascular Institute, Germantown, TN USA
*Corresponding Author: Gary L Murray, The Heart and Vascular Institute, 7205 Wolf River Blvd, Germantown,
Citation: Gary L Murray (2020) Re-print-Ranolazine may be the Best and Safest Pharmacologic Therapy For Congestive Heart Failure, And Safe, Effective For Ventricular And Atrial Arrhythmias. J, Clinical Cardiology and Cardiovascular Interventions, 3(12); Doi:10.31579/2641-0419/110
Copyright: © 2020 Gary L Murray, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 November 2020 | Accepted: 27 November 2020 | Published: 08 December 2020
Keywords: ranolazine; congestive heart failure; ventricular arrhythmia; atrial arrhythmia
Background: Ranolazine (RAN) reduces cardiac sodium channel 1.5’s late sodium current(INaL ) in congestive heart failure (CHF), reducing myocardial calcium overload, potentially improving left ventricular ejection fraction(LVEF) and reducing arrhyth- mogenic after potentials. RAN blocks neuronal sodium channel 1.7(Nav 1.7), potentially altering parasympathetic and sympathetic (P&S) activity. RAN also selectively blocks inactivated atrial Nav 1.8, as well as ventricular IKr and ICaL, affecting atrial and ventric- ular arrhythmias.
Methods:
(1)Matched CHF patients were given RAN (1000 mg p.o. b.i.d.) added to guideline-driven therapy (RANCHF, 41 systolic, 13 diastolic) or no adjuvant therapy (control, NORANCHF, 43 systolic, 12 diastolic). Echocardiographic LVEF and P&S measures were obtained at baseline and follow-up (mean 23.7 months).
(2)A total of 59 patients with symptomatic PVCs were identified from full-disclosure Holters. Doses of 500 - 1,000 mg RAN b.i.d. were given to 34% and 66% of patients, respectively, and Holters were repeated (mean 3.1 months). Congestive heart failure (CHF) was defined as symptoms including dyspnea, orthopnea, paroxysmal nocturnal dyspnea, and edema, with a brain natriuretic peptide
> 400. Systolic heart failure with reduced ejection fraction (HFr EF) vs. diastolic CHF (HFpEF) depended upon LVEF≥ 40%.
Results:
(1)LVEF increased in 70% of RANCHF patients, an average of 11.3 units. Mean LVEF remained unchanged in NORANCHF pa- tients. P&S measures indicated cardiovascular autonomic neuropathy (P<0.10 bpm2) in 20% of NORANCHF patients at baseline and 29% at follow-up (increasing in both groups). At baseline, 28% of patients had high sympathovagal balance (SB), RAN normalized SB in over 50% of these; in contrast, the NORANCHF group had a 20% increase in patients with high SB.
(2)Upon repeat Holters at a mean of 3.1 months after initiating RAN, 95% (56/59) of the patients had their PVC count reduced: 24% (14/59) had more than 90% decrease, 34% (20/59) had 71 to 90% decrease, and 17% (10/59) had 50 to 70% decrease. In the entire group, RAN reduced PVCs by 71% (mean 13,329 to 3,837; p < 0.001). Ventricular bigeminy was reduced by 80% (4,168 to 851; p < 0.001), ventricular couplets were reduced by 78% (374 to 81; p < 0.001), and ventricular tachycardia (VT) was reduced by 91% (56 to 5; p < 0.001). The PVC reduction was dose dependent without proarrhythmia.
Conclusions:
(1)RAN preserves or improves LVEF and decreases high SB in CHF.
(2)RAN offers an effective and safe pharmacologic treatment for symptomatic PVCs.
Despite advances in pharmacologic management [1-5] and device therapy [6], improvement in left ventricular (LV) function in congestive heart failure (CHF) patients, while statistically significant, remains relatively mild in many subjects. The late sodium current (INa) present in CHF causes an intramyocardial calcium (Ca++) overload that results in diastolic dysfunction and micro vascular compression that can worsen LV function [7]. RAN binds to amino acid F1760 of the cardiac sodium channel 1.5 (Nav1.5), thereby reducing the late INa. In a therapeutic concentration (6 μmol), intramyocardial Ca++ overload is reduced 50%. Additionally, RAN blocks neuronal sodium channel 1.7 (Nav1.7) in a strongly use-dependent manner via the local anesthetic receptor [8, 9]. Therefore, RAN may directly alter function of the parasympathetic and sympathetic (P&S) branches of the autonomic nervous system (ANS). We postulated these actions of RAN should result in favorable changes in LV function and P&S measures in CHF.
RAN’s inhibition of the late sodium current (INa), results in suppression of early and delayed after depolarization’s (EAD/ DAD), thereby reducing triggered ventricular ectopy. An increase of the late INa induces EAD/DAD resulting in triggered activity. The diastolic transient inward current in the long QT syndrome is caused by calcium overload and is inhibited by RAN. Because RAN has no known proarrhythmic effects and, to the contrary, protects against torsades de pointes, we hypothesized that RAN could be an effective and safe pharmacologic treatment for symptomatic premature ventricular contractions (PVCs).
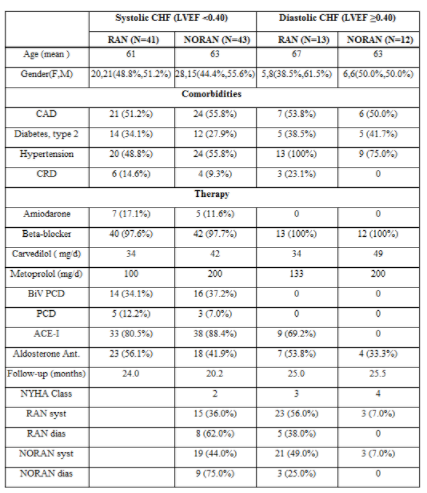
(1) One hundred and nine systolic or diastolic, New York Heart Association(NYHA) class2-4CHFpatientswereincludedinthisstudy. They were treated according to standard heart failure guidelines [10]. In an open-label,unblinded fashion, patients were prescribed Ranolazine (RAN, 1000 mg po-bid) in addition to standard heart failure therapy (RANCHF, 41 systolic,13 diastolic) or no adjuvant therapy (control, NORANCHF, 43 systolic, 12 diastolic). Patients were matched for age, gender and history. Patient demographics are presented in Table I. Since patients were on maximally tolerated doses of beta-blocker and angiotensin-converting enzyme inhibitor (ACE-I) or angiotensin receptor blockers (ARBs), only the diuretic dose was adjusted as needed. Diastolic CHF is defined as CHF with LV ejection fraction (LVEF) ≥0.40. Baseline 2D-echocardiograms were obtained and the LVEF calculated as the average of the apical 2 and 4 chamber Simpson’s method [11], and studies were repeated within 36 months (mean follow-up for RANCHF patients is 24.5 months and for NORANCHF 22.8 months, Table-II). The accuracy of the initial echocardiographic LVEF was confirmed by being within 5 ejection fraction units (EFUs) of the LVEF as measured by nuclear multigated acquisition. Serial changes in any patient of ≥±7 EFUs are considered clinically significant [12]. Other measurements are per American Society of Echocardiography guidelines [13]. CHF is classified as systolic or diastolic, rather than CHF with preserved (normal) LVEF or reduced LVEF, because the RANCHF group only had one subject with a normal LVEF.
Another 30 subjects without CHF or an indication for RAN (20 male, 10 female, average age 61 years) with “CHF-like” abnormal P&S activity with high SB (25/30, 83%), CAN (1/30, 3%) or both(4/30, 13%) were identified. Twenty (67%) had a history of coronary disease, but only 5 (17%) were not completely re- vascularized, and 3(10%) had a positive nuclear stress test. Sixteen (53%) were hypertensive, 11 (31%) were diabetic and 4 (13%) were on a beta-blocker. The causes of their abnormal P&S included chronic pain or anxiety, diabetes and hypertension. RAN 500-1000 mg bid was prescribed, and the P&S testing repeated on the 5th day. No subject had high BNP or low LVEF.
P&S function in response to Ewing challenges [14] was assessed noninvasively using the Physio, PS, Inc., Atlanta, GA, and ANX 3.0 Autonomic Function Monitor.
P&S activity was computed simultaneously and independently based on concurrent, continuous time-frequency analyses of respiratory activity (RA) and heart rate variability (HRV) [15-19]. Parasympathetic activity (measured as the respiratory frequency area, RFa) is defined as the spectral power within a 0.12 Hz-wide window centered on the fundamental respiratory frequency (FRF) in the HRV spectrum. FRF is identified as the peak spectral mode from time-frequency analysis of RA. Effectively, FRF is a measure of vagal outflow as it affects the heart (a measure of cardio vagal activity). Sympathetic activity (low-frequency area, LFa) is defined as the remaining spectral power, after computation of RFa, in the low-frequency window (0.04-0.15 Hz) of the HRV spectrum. High sympathovagal balance (SB = LFa/RFa) is defined as a resting LFa/RFa ratio >2.5. P&S activity was recorded from a standard autonomic test, including 5 minutes rest; 1 minute paced breathing (6 breaths/min), a Valsalva challenge (including a 15-sec Valsalva maneuver) and a quick stand followed by 5 minutes of quiet stand. The average SB reported is the average of the ratios recorded during the sampling period, not a ratio of averages. Cardiovascular autonomic neuropathy (CAN) was defined in standard fashion [20, 21], reflecting very low, resting RFa (<0.10 bpm2) [22]. The P&S method is valid regardless of challenge or patient state or history. Normal SB is 0.42.5 and CAN define a high mortality risk, including silent MI, sudden cardiac death and acute coronary syndrome (ACS) [23-25]. Records including high-quality arrhythmia are omitted. P&S and HRV measures are correlated with outcomes. While the patient population is underpowered to make final health outcome assessments, we determined the occurrence of major adverse cardiac events (MACE), defined as cardiac death (determined from hospital records or death certificates), heart failure hospitalization and ventricular tachycardia or fibrillation (as determined by defibrillator therapy, or administration of intravenous amiodarone for arrhythmia termination) alone or as a composite endpoint. All subjects signed appropriate informed consent forms for the studies and treatments rendered.
Continuous data were assessed for normality with normally distributed data analyzed using Student t-tests and non-normally distributed data assessed using a Mann-Whitney test. Dichotomous data were analyzed using the Chi-square test or Fischer’s Exact Test. A p-value of ≤0.05 was considered significant. We determined that we needed 50 patients per group to have a sufficient sample size using an alpha of 0.05, difference of means of 6 units and expected standard deviation of 15 units with a power of 80%. All statistics are performed under SPSS v 1.4. Student t-tests are performed as two-tailed with equal variance. Significance values are determined on the null hypothesis that pre- and post-treatment values are equal.
(2) Using full-disclosure 24-hour Holters (Burlick), 59 adult patients with highly symptomatic, frequent PVCs were identified during routine outpatient clinic visits. The PVCs met criteria for “ventricular Para systole” (VP): non-fixed coupling, fusion, interpolation, and a mathematical relationship with R-R intervals. Doses of 500 and 1,000 mg b.i.d. were given to 34% and 66% of patients, respectively, depending on tolerability, without the side effects of headache, dizziness, nausea, or constipation, or the patients’ symptomatic improvement. Holters were repeated at 1 week and up to 2 years (mean: 3.1 months) and were compared. Response was defined as at least 50% reduction in PVC count and/ or at least 70% reduction in complex PVCs. All statistics, including means, standard deviations, and Student’s t-tests, were performed under SPSS v 14.1 (IBM). Student’s t-tests were performed as two- tailed tests with equal variance. Significant values were determined on the null hypothesis that the pre- and post-treatment values were equal. All patients were informed that RAN administration for PVCs was not approved by the U.S. Food and Drug Administration, hence it was off-label use, and gave appropriate informed consent
CHF
Overall, 109 age-, gender- and history-matched CHF patients treated according to standard heart failure guidelines [10] were included in the study, with 54 patients receiving RAN and 55 patients in the control group. Demographic comparisons are provided in Table-I and are similar between groups: 93% of the patients are evenly divided between NYHA class 2 and 3; 98% are on a beta-blocker (NORANCHF subjects at a slightly higher dose). Slightly more diastolic RANCHF patients have hypertension and chronic renal insufficiency.
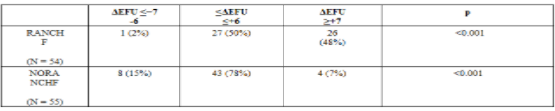
Left ventricular ejection fraction
On follow-up, RANCHF patients had significantly higher LVEF (Table-II; systolic CHF: p<0.001, diastolic CHF: p = 0.003). Controls had no significant change in the mean LVEF. When viewed dichotomously (Table-III), 26/54 (48%) RANCHF patients experienced a clinically significant increase in LVEF (≥+7EFU) as compared to 4/55 controls (7%, p<0.001, Table-III).From the systolic RANCHF subgroup, 17/41 (41%) subjects experienced a clinically significant increase (>7 EFUs) in LVEF as compared to 9/13 (69%) diastolic RANCHF patients (p<0.001). Final LVEF in cohort patients experiencing MACE was significantly lower than in those who were MACE-free (Table-IV and Table-V, p = 0.005). In the RANCHF group MACE subpopulation, the initial to final LVEF increase was less than in patients without MACE, 6 EFUs vs. 9 EFUs (Table-IV, p<0.020).In control patients, insignificant changes in LVEF occurred regardless of MACE or not (p>0.050).


Other echocardiographic data
Systolic RANCHF patients demonstrated a decrease in left ventricular internal dimension in systole (LVIDs). Diastolic RANCHF patients demonstrated a slight increase in LVID diastole (LVIDd) coupled with a slight decrease in LVIDs. Baseline LVID (Table-II) trended similar between groups (p>0.050). LVIDd averaged 5.88 and 6.09 cm for systolic RANCHF and NORANCHF patients, and 5.16 and 5.28 cm for diastolic RANCHF and NORANCHF patients, respectively. LVIDs averaged 4.94 and 5.21 cm for systolic RANCHF and NORANCHF patients, and 4.08 and 4.03 cm for diastolic RANCHF and NORANCHF patients, respectively. RANCHF vs. NORANCHF Patients had significantly lower LVIDs at follow-up (>0.36 cm,p<0.001, Table-II). No significant differences (p>0.050) in baseline or follow-up LVIDd or LAD occurred between experimental groups, although LAD tended to decrease in the systolic RANCHF cohort (4.6 to 4.3 cm, Table- II, p = 0.084).
Autonomic (P&S and HRV) measures
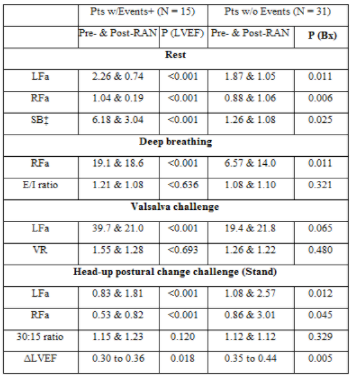
Arrhythmia-free, P&S studies were accomplished every 6 months for 95/109 (87%) patients; 13% of the patients (8 RANCHF and 6 NORANCHF) had arrhythmias precluding a complete assessment. While P&S measures are readable [26], HRV analyses are contraindicated for arrhythmia [27]. Autonomic measures of the RANCHF and control groups are presented in Table VI. The average RANCHF patient demonstrated significant P&S responses to RAN (p≤0.050), except for paced breathing RFa (a parasympathetic stimulus; p = 0.065).This included significant reductions in absolute and relative measures of sympathetic activity. None of the Time Domain Ratio responses to RAN were significant (p≥0.050). The absolute and relative resting sympathetic changes from baseline to follow-up in the control patients were also significant. Sympathetic activity remained high for cohort patients with events (Table-IV and Table-V), even though SB demonstrated a relative decrease from 6.25 to 4.86 (unit less). The high pre-RAN SB (higher than the ratio of the averages might suggest, (Table-IV) is due to two patients with severe CAN. Post-RAN, these patients were found to no longer be in CAN and demonstrated an increase of ≥7 EFUs, on average (p = 0.0002). The parasympathetic response to deep breathing is slight. The change in RFa is well correlated with the changes in LVEF (p<0.001). The exhalation to inhalation (E/I) ratio decreases (not significant). The sympathetic (LFa) decrease with Valsalva challenge. The VR decreases (not significant).The Valsalva challenge responses are well correlated with the changes in LVEF (p<0.001).
Sympathetic withdrawal (SW) was demonstrated by 9/15 RANCHF patients. These patients all demonstrated an abnormal BP response to standing. Upon follow-up, these patients demonstrated an average increase in sympathetic activity (a normalized response) as compared with rest, with improved standing BP, Only four RANCHF patients continued to demonstrate SW. The stand responses are well correlated with changes in LVEF (p<0.001).For NORANCHF cohort patients (Table-V), the relative sympathetic measure (SB) increased (p<0.05). In the RANCHF group without events (Table-IV), the relative measure (SB) decreased. These SB changes are significantly associated with changes in LVEF (p<0.001). The associated average increase in LVEF is more than +9 EFUs. The patients without events started in balance (normal SB) and remained in balance. The resting changes are well correlated with the changes in LVEF (p<0.001). The pre- and post-RAN resting P&S responses in both the subpopulations with and without events are significant (p≤0.025). The pre- and post-RAN deep breathing parasympathetic measures (RFa) in both the subpopulations with and without events are significant (p≤0.011), but not the increases in E/I ratio (p>0.321). Nearly half (14/27) of the pre-RAN event patients demonstrated SW in response to stand, indicating orthostatic dysfunction. These findings are associated with abnormal blood pressure responses to stand. Post-RAN, the average patient without events reversed their SW. This is a normalized response. Only six patients continued to demonstrate SW after history of RAN. The pre- and post- RAN autonomic responses to stand in both subpopulations are significant (p≤0.045).
Table-V presents baseline and follow-up P&S measures and LVEF in the NORANCHF patients with and without events. P&S changes were significant (p≤0.050) for patients with events. Their SB started high and increased upon follow-up. The patients without events demonstrated opposite absolute changes upon follow-up. However, the net result was an increase in SB to above normal. Only the E/I ratio change for the patients with events was significant (p = 0.013).
Five days of RAN administered to 30 subjects without CHF or angina, but with “CHF- like” dysautonomia improved high SB and CAN in 27/30 (90%), normalizing SB and CAN in 20/30 (67%) of subjects (Table-VII). P&S responses returned to baseline after discontinuing RAN.

Health outcome assessment
The composite MACE endpoint occurred in 17/54 (31.5%) RANCHF patients and 21/55 (38.2%) control patients. When evaluated separately, each MACE endpoint was lower in the RANCHF patients.
RESULTS-(2) PVCS
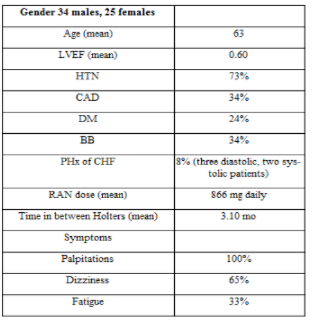
Patient demographics are summarized in Table VIII. Mean age was 63 years, 58% were males, mean left ventricular ejection LVEF was 0.60 with only 8% having a history of CHF( two systolic, three diastolic), 73% were hypertensive, 34% had coronary artery disease (CAD; all re-vascularized), 34% were taking a beta blocker, and the mean RAN dose was 866 mg per day. All patients experienced palpitations, 65% had dizziness, and 33% complained of fatigue.

Ninety-five% (56/59) of patients had their ventricular ectopy reduced by RAN. Over 40% of patients had at least 10,000 PVCs, and over 25% had greater than 20,000 PVCs. In the entire group, RAN reduced PVCs by 71% (mean: 13,329 to 3,837; p < 0.001). Approximately 24% (14/59) of patients had more than 90% decreases in PVCs, 34% (20/59) had 71 to 90% decrease, and 17% (10/59) had 50 to 70% decreases. Ventricular bigeminy was reduced by 80% (4,168 to 851; p < 0.001), couplets were reduced by 78% (374 to 81; p < 0.001), and ventricular tachycardia (VT) reduced by 91% (56 to 5; p < 0.001). The maximum reduction in PVCs was from 47,211 with 29,573 ventricular bigeminy to 13 PVCs per 24 hour, and no bigeminy, accompanied by a robust resolution of the patient’s incapacitating fatigue. This patient stated: “My life has been returned to me. I can return to work”. No proarrhythmia was observed, and there were no significant side effects of treatment. Approximately 6% of patients reported one or more of the following side effects: Constipation, dizziness, nausea, or headache. One of the initial three non-responders had response 1.5 years later with 16,890 PVCs and 10,114 ventricular bigeminy reduced to only 3 PVCs per 24 hours.
Discussion-(1)
In the past 30 years, improvements in LV function and outcomes in systolic CHF have been attributed to pharmacologic therapy addressing the neurohumoral paradigm, together with the advent of device therapy [1-6]. However, even more Improvement is needed. This has triggered stem cell trials [28] and a search for new pharmacologic agents. To date, no therapy in diastolic CHF has shown improved survival. RAN is a first in class drug. It reduces the late sodium current (INa) resulting in a 50% reduction of the intramyocellular Ca++ overload caused by the late INa via the Na+/Ca++ exchanger [7].This improves diastolic and micro vascular dysfunction [29], and should result in improved LV systolic function. Since LVEF is widely accepted as one of the most important prognostic indicators in CHF [30], we focused on its changes after RAN was added to guideline-driven therapy.
In therapeutic concentrations (2-6 μmol), RAN also inhibits neuronal Nav1.7 via the local anesthetic receptor in a use-dependent fashion [8, 9]. Consequently, RAN potentially can alter ANS function directly, improving P&S measures. High sympathetic tone (high SB) with critically low parasympathetic activity (CAN) indicates high mortality risk, and has been associated with sudden cardiac death, CHF and ACS [20-25, 31]. This study is the first to correlate CHF outcomes with changes in both LVEF and P&S measures.
We found RAN significantly increased LVEF by 6.4 EFUs in systolic CHF patients and 9.5 EFUs in diastolic CHF (Table-II). In the NORANCHF group, final LVEF fell 1 EFU in the systolic CHF patients and 0.5 EFU in the diastolic CHF patients (Table- II). These LVEF changes represent mean values of the cohort groups. In the systolic RANCHF patients, the increase in LVEF was solely due to a decrease in LVIDs (Table-II). In diastolic RANCHF patients, the increase in LVEF was due to a slight increase in LVIDd (suggesting increased diastolic filling) coupled with a slight decrease in LVIDs (suggesting improved systolic emptying; Table-II). Individually, only 1/54 (2%) RANCHF patients decreased LVEF by ≤−7 EFUs and 26/54 (48%) RANCHF patients increased LVEF by ≥+7 EFUs, with the remaining 50% of patients showing little LVEF change (p<0.001, Table-III). Increases in the RANCHF patients’ LVEF were sufficient to avoid defibrillator implantation in 10 subjects, resulting in substantial cost savings. In the control group, 8/55 (15%) decreased LVEF by ≤−7EFUs, and only 4/55 (7%) patients increased LVEF by ≥+7EFUs, with the remaining 43/55 (78%) demonstrating little change (Table. III). Therefore, LVEF is more than 6 times as likely to increase and 1/8TH as likely to decrease following RAN therapy in CHF patients. LVEF can increase regardless of the initial LVEF. RAN increased LVEF by ≥+7 EFUs in 17/41 (41.5%) systolic CHF patients vs. 9/13 (69%) diastolic CHF patients (p<0.001). Furthermore, when RAN increased LVEF by ≥+7 EFUs, 9/26 (35%) patients had a history of CAD, whereas 17/26 (65%) did not (p<0.001). Since almost 80% of the CAD patients were re-vascularized, and only 14% had a positive stress test, we feel the smaller increases in LVEF in CAD patients were due to LV scarring secondary to remote myocardial infarctions. Finally, whether or not LVEF increased by ≥+7 EFUs did not depend upon the maximum tolerated dose of beta-blocker (94% took carvedilol), as the mean daily dose differed by only 0.5 mg. Autonomic (P&S and HRV) measures have been documented to be associated with LVEF and cardiovascular risk (32).Table VI presents the P&S and LVEF data without regard to clinical outcomes. RANCHF patients demonstrated a decrease in SB from 2.42 to 1.98 (p = 0.019) mainly resulting from a reduction in LFa, for example, a sympatholytic effect. Sympatholytic, such as beta-blockers, are known to be cardio protective. This protection is at least in part due to a decrease in SB (balance) toward 1.0 indicating less sympathetic activity and a relative Increase in parasympathetic activity [33]. And it is associated with reduced CAN risk. NORANCHF patients almost doubled their initially high-normal SB as a result of a marked increase in LFa with only a small increase in RFa, increasing the risk for MACE. The ANS responses to standing were more normal after RAN, indicating improved ANS function and reduced risk of orthostasis. Orthostasis not uncommonly limits the doses of beta- blockers and ACE-Is/ARBs CHF patients can tolerate. Conversely NORANCHF patients on average displayed a more abnormal standing response during follow-up, resulting from a decrease in LFa (SW) consistent with worsening of ANS function, increasing the risk for orthostatic. In contrast to the dramatic LFa changes noted in both groups, RFa (parasympathetic) Activity changes were very small, consistent with the lack of significant changes in the Time Domain Ratios, and CAN was not, on average, improved. The lack of a significant impact upon CAN means RAN’s reduction of SB might be an important mitigating factor reducing the CV risk of CAN. Differences in ANS measures in patients with or without events are presented in Tables-IV and Table-V.
While this study was an open enrollment (nonrandomized) trial and underpowered to make final health outcome assessments, we found a qualitative reduction in the composite endpoint of cardiac death, CHF admissions and therapies for Ventricular Tachycardia and Ventricular Fibrillation (VT/VF) in the RANCHF group. There was a 40% event reduction, with 57% fewer deaths, 60% fewer VT/ VF therapies, and 20% fewer CHF hospitalizations. The initial LVEF was lower in MACE patients than in non-MACE patients (Table-V and Table- VI). Only the RANCHF group increased LVEF during follow-up, and the increase was more in patients without events. The increase in MACE patients’ LVEF (Table-IV) was the same as the LVEF increase of the entire systolic RANCHF group (Table- II), yet RANCHF patients had 40% fewer events. Therefore, high sympathetic activity as indicated by high SB was more predictive of MACE than a change in LVEF. When SB was ≤2.5 or LVEF was ≥0.32, 81% or 79% of subjects, respectively, were MACE free; when SB was >2.5, 59% of patients suffered MACE vs.50% of patients when LVEF was <0.32. Since 5 days of RAN administration to patients without CHF (or angina) resulted in similar P and S changes to the CHF patients, this strongly suggests a direct effect of RAN upon P and S independent of hemodynamics.
Discussion-(2) PVCS
RAN has several electrophysiological effects with no known proarrhythmia [34-35]. IKr and late INa are inhibited at concentrations within therapeutic range. In addition, RAN has been shown to inhibit the diastolic transient inward current [36] resulting in suppression of after depolarization. Although the QT interval is prolonged by approximately 6 ms due to IKr inhibition, there is no trans mural dispersion of repolarization, and RAN is protective against torsades de pointes [37].
EAD/DAD is causes of triggered ventricular ectopy [38-39] and can be induced by late INa that RAN inhibits. DAD are due to spontaneous release of Ca++ from the sarcoplasmic reticulum, and EAD are directly due to Ca++ entry through the Ca++ window current, except in Purkinje fibers where EAD are due to late INa window current(35,39) Some clinical scenarios of EAD/DAD- mediated ventricular arrhythmias include CHF [40], catechol aminergic polymorphic VT(41) hypokalemia [42] left ventricular hypertrophy (LVH) [43] long QT syndrome [44] and cocaine use [45] Our patients met criteria for VP [46-47] This is the second study reporting effects of RAN on PVCs in humans, but the first focusing exclusively on triggered ventricular ectopy.
VP (PVCs with variable coupling, fusion, interpolation, and a mathematical relationship with R-R intervals) occurs in 1 of 1,300
patients and can be a highly symptomatic arrhythmia, which is thought to be caused by EAD/DAD [46-47]. Prognosis depends upon any coexisting cardiac disease. Rarely does ventricular fibrillation or syncope occur, and VT is slower than reentrant VT. Several drugs have been tried as treatment for VP. Verapamil produced a satisfactory response in 18% of treated patients A report of two patients responding to adenosine has been published Dilantin was successful in one patient Cardiac pacing succeeded in two patients [48-51]. Amiodarone produced good results in nine patients only 33% of patients with VP responded to the usual sodium channel blockers [52].
Activation of late INa (for example, by phosphoralization by Ca++/calmodulin kinase ll), may be a common myocardial response to stress. Therefore, RAN may have a therapeutic role in treating many cardiac conditions, including unstable ischemic patients with PVCs and patients with atrial fibrillation [53].
RAN was very well tolerated, with only 6% of patients experiencing headache, dizziness (not BP-related, but a direct CNS effect), nausea, or constipation, with no known organ toxicity except in DMII patients with class 4, 5 renal failures. Patients’ symptoms improved proportionally to PVC reduction. In canine ventricular wedge preparations, RAN did not induce torsades de pointes, reduced the action potential duration of M cells, and suppressed EAD induced by d-sotalol and hypoxia [54-55]. These are potential explanations of why RAN administration caused no proarrhythmia in this study. RAN is metabolized by CYP 3A so that inhibitors of this enzyme, such as ketoconazole, diltiazem, verapamil, macrolid Antibiotics, HIV protease inhibitors, and grapefruit juice, increase RAN levels. Inhibitors of g-glycoprotein increase plasma levels two- to threefold. RAN increases digoxin concentrations 1.4- to 1.6-fold, and simvastatin Cmax is doubled.
The patient population hersein reported seems reasonably typical of adults who would be referred to a cardiology practice primarily for ventricular arrhythmia evaluation and therapy. Patients were essentially Medicare-age with multiple Comorbidities, but well-preserved LVEF and highly symptomatic with palpitations, dizziness, and fatigue. Syncope and cardiac arrest were not methods of presentation.
In summary, RAN was found to be highly effective in suppressing triggered VPC. Isolated PVCs were reduced from 13,329 to 3,837, ventricular bigeminy reduced from4,168 to 851, ventricular couplets reduced from 374 to 81, and VT was reduced from 56 to 5, representing reductions of 71%, 80%, 78%, and 91%, respectively. One of the initial three non-responders demonstrated a remarkable response 1.5 years later with 16,890 PVCs reduced to only 3 PVCs per 24 hours (99% reduction). The presenting symptoms were improved in proportion to PVC reduction (marked decrease in palpitations, fatigue, and dizziness).
Limitations (1)
This is a single-center study. Recently, it was proposed that diastolic CHF be defined as CHF with LVEF≥0.50 [10]. Had we used this definition, only one of our diastolic RANCHF patients would have remained, increasing the systolic RANCHF group to 50 patients. With a new definition of systolic CHF requiring an
LVEF<0.50 (instead of ≤0.40), RAN would have increased LVEF ≥+7 EFUs in 26/53 (49%) systolic CHF patients, an increase from the 14/41 (34%) herein reported (p<0.001), with RAN being the last add-on therapy. Using spectral analysis of HRV to estimate cardiac sympathetic activity in CHF has its limitations. The sinoatrial node becomes less responsive to norepinephrine and acetylcholine, so HRV decreases despite high norepinephrine levels. Therefore, absolute cardiac LFa is inversely related to sympathetic outflow to muscle. Spectral analysis measures the modulation of autonomic neural outflow to the heart. SB reflects this modulation and an SB>2.5 have a positive predictive value of 61% for MACE. In comparison to 123 Iodine, Metaiodobenzylguanidine (MIBG) imaging to assess cardiac sympathetic activity, only 29% of CHF patients with high MIBG washout suffered MACE within a mean follow-up of 31 months [56].
Limitations (2)
This is a single-center open-label study. A larger, randomized prospective study might be useful in confirming these results. Furthermore, RAN can suppress the more common reentrant PVCs [54]. Reentrant patients weren’t studied, but if RAN were a successful therapy because of its safety, then RAN could be the first drug choice to treat the majority of patients with symptomatic PVCs.
Conclusions (1)
RAN preserved or improved LVEF during a 24 month follow-up period when added to guideline-driven therapy in CHF. Since LVEF has long been considered one of the most important prognostic indicators in CHF, and since RAN seems free of the potentially harmful side effects of some of the agents that increase LVEF (such as catecholamines, phosphodiesterase inhibitors, and Entresto), RAN has the potential to improve CHF mortality and morbidity without significant adverse effects.
Reduced sympathetic tone (LFa) and SB were present in RANCHF patients; the lowest measures of both were in RAN treated patients without MACE. When SB was ≤2.5, only 19% of subjects experienced MACE. High SB with low RFa (<0.1bpm2, defined as CAN) is associated with increased mortality and morbidity risk. Therefore measuring P&S function should improve our ability to risk-stratify our patients and adjust their management accordingly. Periodic P&S measures have become just as a routine management tool in our CHF patients as assessment of LVEF or measurement of (pro-) brain natriuretic peptide.
Conclusions (2)
RAN offers a safe, effective pharmacologic therapy for symptomatic VP patients whose PVCs are due to triggered activity, with no known proarrhythmia. It may have a role to play in treating symptomatic PVCs in Patients with LVH, CHF, hypokalemia, acute hypoxia, oxidative stress, catecholaminergic polymorphic VT, cocaine-related PVCs, and drug-induced torsades de pointes [57]. It is the pharmacologic treatment of choice for VP.
Conflict of Interest
The author reports no conflicts of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
