
Research Article | DOI: https://doi.org/10.31579/2641-0419/094
1Director of Clinical Research, The Heart and Vascular Institute, Germantown, USA
2Parasympathetic & Sympathetic Nervous System Consultant, Franklin Cardiovascular Associates, Sewell, New Jersey – USA
3Physio PS, Inc., Atlanta, Georgia – USA
*Corresponding Author: Gary L Murray, The Heart and Vascular Institute, 7205 Wolf River Blvd, Germantown.
Citation: Gary L Murray and Joseph Colombo., (2020) Re-print: Maintenance (r) Alpha Lipoic Acid Reduces Sudden Cardiac Death in Geriatric Diabetes Mellitus II Patients. J, Clinical Cardiology and Cardiovascular Interventions, 3(9); Doi:10.31579/2641-0419/094
Copyright: © 2020 Gary L Murray, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 30 September 2020 | Accepted: 09 October 2020 | Published: 16 October 2020
Keywords: alpha lipoic acid; dabetic autonomic neuropathy; sudden death.
Background: Diabetes carries a two-fold risk of Sudden Cardiac Death (SCD). Diabetic Autonomic Neuropathy (DAN), often progressing to Cardiovascular Autonomic Neuropathy (CAN, critically low parasympathetic tone [P]), increases death 3.5-fold over 5 years, half sudden or non- renal. Oxidative stress is a major cause of DAN. Also, increased sympathetic tone (S), High Sympathovagal Balance [SB>2.5] increases SCD risk.
Objective: Dysautonomic diabetic II patients were treated with the antioxidant (r) Alpha Lipoic Acid (ALA), autonomic function followed, and Sudden Death (SD) compared to untreated patients. Methods: 133 patients (mean age 66y/o) with DAN or CAN, diagnosed using the ANX
3.0 Autonomic Monitor (Physio PS, Inc., Atlanta, GA) was offered (r)-ALA: 83 agreed (Group 1), and 50 refused (Group 2). P and S were re- measured up to 3 times/yr (mean f/u 6.31 yrs); SCDs were recorded.
Results: A 43% Relative Risk Reduction (RRR) in SCD occurred with (r)- ALA (25% SCD Group 1 vs. 44% SCD Group 2, p=0.0076). Initial to final patients with high SB or CAN were 21.7%-12% (p=0.010), 10.8%- 15.7% (p=0.045), Group 1 vs. 24%-22% (p=ns), 6%-12% (p=0.083), Group 2. Only Group 1 survivors increased mean resting P. The progressive increase in P’s decline, increasing CAN risk, in the other patients correlated with mortality (p<0.001) and (r) ALA dose. Initially, Group 1 had insignificantly less high SB (p=0.449) and significantly more CAN (p=0.013) vs. Group 2. Finally, Group 1 had significantly less high SB (p=0.0967) vs. Group 2, also improving to insignificantly more CAN (p=0.261).
Conclusion: (r)-ALA was associated with a 43% RRR of SCD and favorable P and S changes.
SCD-Sudden Cardiac Death,
DAN-Diabetic Autonomic Neuropathy,
CAN-Cardiovascular Autonomic Neuropathy,
P-Parasympathetic tone,
Diabetics have a two-fold increased risk of Sudden Cardiac Death (SCD), the most common cause of death in adult diabetics. Subgroup analyses have not explained this adequately [1]. Diabetic Autonomic Neuropathy (DAN) [2], carries a 53% 5yr. mortality, half of the deaths sudden [3]. DAN can progress to Cardiovascular Autonomic Neuropathy (CAN) in approximately 65% of patients with aging and diabetes duration [4]; CAN, critically low Parasympathetic tone (P), increased SCD in the Framingham Study [5]. Hyperglycemic- oxidative stress causes dysautonomia [6-8]. We hypothesized (r)-ALA, a natural, potent anti-oxidant, might reduce SCD in Type 2 Diabetics (DMII) with dysautonomias. We have shown previously (r)-ALA improves autonomics in Hypertension (HTN) [9] as well as Neurogenic Orthostatic Hypotension (NOH) [10].
In 2006, 133 consecutive DMII referrals for cardiovascular evaluation underwent P and S testing via ANX 3.0 Autonomic Monitoring (P&S Monitoring, Physio PS, Inc., Atlanta, GA). P&S were computed simultaneously and independently by concurrent, continuous time- frequency analysis of Respiratory Activity (RA) and Heart Rate Variability (HRV), as we detailed previously [11-17]. P&S srenormally; sitting LFa and RFa=0.5 to 10.0 bpm2; SB is age dependent=0.4 to 1.0 for geriatrics; stand LFa is ≥ 10% increase with respect to (wrt) sit; stand RFa is a decrease wrt sit. High SB is defined as>2.5, as established in our 483 patient study [18]. High SB and CAN define a high risk of mortality, Acute Coronary Syndromes (ACS), CHF, and Ventricular Tachycardia/Fibrillation (VT/VF) alone or as a composite endpoint [18].
In the 83 (r)-ALA patients (Group 1), P&S were recorded 2-3 mo. afterwards until maintenance dosage, then yearly. Non-(r)ALA patients (Group 2, refused (r)-ALA) were tested yearly. Exclusion criteria were (1) arrhythmia precluding HRV measurement, and (2) cancer within 5 yrs. The inclusion criterion was DM II with any abnormality of P or S. Informed consent was obtained for this open-label, un-blinded study. The cause of SD was determined from hospital records or death certificates. Out of hospital SCD was defined as pulse less SD of cardiac origin.
Group 1 patients were subcategorized: survivors, Group AA; non- survivors Group AD. Group 2 (Controls): survivors, Group NA; non- survivors, Group ND. All patients took aspirin. All patients had Cardiovascular Autonomic Reflex Test (CART) w/o isometric grip (grip has only 25% sensitivity for CAN) [19]. DAN was defined as any abnormality of S or P, or high SB. CAN was defined as P<0.10bpm2, or 2 abnormalities of CARTs. Median follow-up was 5 yrs. Mean age was 66 y/o. There were 83 males, 50 females. Upon referral, rhythm assessment (Holters ± event monitors) were performed if clinically indicated: Groups AA 60%, AD 57.1%, NA 60.7%, ND 31.8%.
The abbreviations are: Δ, change from initial to final; A1C, glucose form hemoglobin; (r) ALA ((r)Alpha-Lipoic Acid) (the r-isomer functional in humans); BMI (Body Mass Index); Bx (Baseline); CAN; DAN; dBP (Diastolic Blood Pressure); HL (Hyperlipidemia); HR (Heart Rate); Init (Initial); LFa ((Low Frequency area)=S)); LVEF (Left Ventricular Ejection Fraction); mg (milligrams); N (number); Nml (normal); ns (not significant); P (Parasympathetic tone); PE (Parasympathetic Excess); QTc (corrected QT); RFa ((Respiratory Frequency area)=P)); S (Sympathetic tone); SB (Sympathovagal Balance); sBP (systolic BP); SW (Sympathetic Withdrawal). Given the size of the cohort, statistical significance is p<0.100. Statistical significance was determined with either a two-tailed, student T-test or a Pearson correlation.
25% of (r)-ALA patients experienced SCD vs. 44% non-(r)-ALA patients, a 43% Relative Risk Reduction (RRR, p=0.0076 [Figure 1]), altering the natural history of DAN [3].
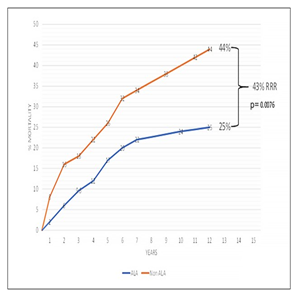
Figure 1: Sudden Death Mortality risk of a Diabetic type 2 cohort from a south-central USA cardiology practice. (r)ALA (blue curve) reduced this cohort’s relative risk ratio (RRR) by 43% (p=0.0076) as compared to controls (brown curve).
Demographics
Table 1 Survivor demographics Group AA had significantly more males and higher final A1C; their initial LVEF was insignificantly lower, factors not favoring survival [20-24]; tending to favor survival were insignificantly fewer with CAD (although all AA and NA patients were vascularized with normal stress tests), less Chronic Kidney Disease (CKD); and significantly more Angiotensin blocker therapy (ACEI or ARB, p<0.100) [20,25]. 11% more (r)-ALA patents required insulin. Control Group NA had significantly more females and lower final A1C; there were insignificantly higher initial LVEFs and insignificantly more patients on Empagliflozin, Liraglutid, and Metformin, tending to favor survival [26-29].
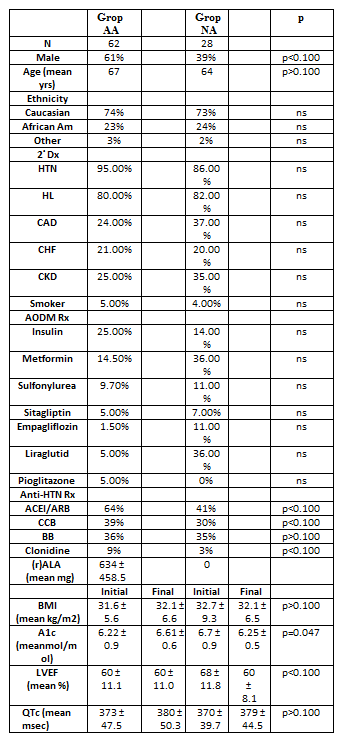
Note: 2° Dx=Secondary Diagnosis; ACEI=Angiotensin Converting Enzyme Inhibitor; ARB=Angiotensin Renin Blocker; BB=Beta-Blocker; CCB=Calcium Channel Blocker; HL=Hyperlipidemia; Rx=therapy.
Table 1: Survivor Patient Demographics.
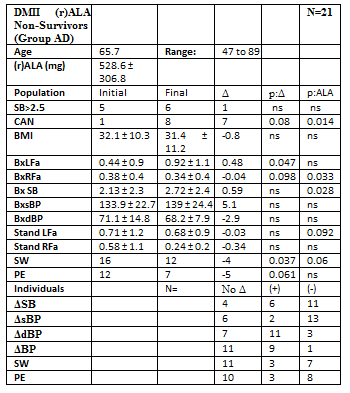
Table 2 Non-Survivors. Group AD had significantly more males and higher A1C; there were insignificantly higher final BMI [24], lower LVEFs, more CHF, and less Metformin use, all tending unfavorably regarding survival. But 9% more took ACEI/ARBs (p<0.100). Control Group ND was 4 years older (p>0.100); QTc had no significance on SD, as SD increases when QTc is >450ms in males or >470ms in females [30]. Insignificantly more Group ND African Americans tends to favor SD [31]. CAD causes most adult SDs [24]. Although more SD patients had CAD vs. survivors, CAD prevalence was insignificantly different in Groups AD, ND.
Group AA vs. Group ND: Improved Group AA survival occurred despite Group ND having a normal final BMI (p=0.067), less HTN (p=0.021), greater use of Empagliflozin (p<0.100), Metformin (p<0.100), lower final A1C (p=0.034), and fewer males (p<0.100), all favoring less SCD in Group ND. DMII attenuates gender differences in SD [22]. Group ND was 3 yrs. Older (p=0.067) with more CAD (p<0.100); all were revascularized (normal myocardial perfusion stress tests). Fewer in Group AA took insulin (p<0.100). Initially, Group AA had 18.4% VT (1sustained) vs. 14.3% non-sustained in Group ND, p=0.3559.
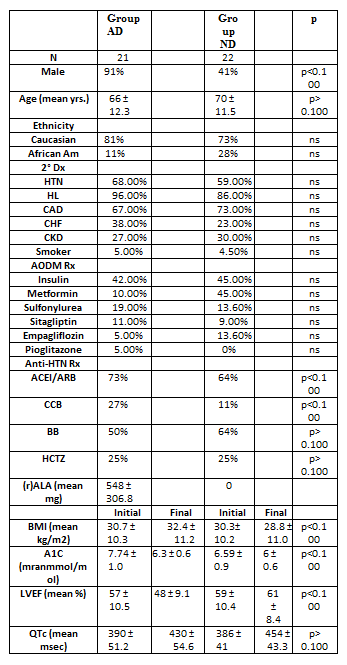
Note: HCTZ, hydrochlorothiazide. See Table 1 or Methods for other abbreviations.
Table 2: Non-Survivor Patient Demographics (Sudden Death Patients).
Autonomic Measures: Table 3: Survivors and SCD patients initial to final autonomic Measures. Mean Bx LFa, decreased in survivors (p=0.045), increasing in SCD (p=0.039). Bx RFa, increased in 55/90 patients (60%), by a mean 12.5% in survivors and severely decreased in 29/43 (67%) non-survivors, mean -59.5%, (p<0.0001). SB increased 17.6% in survivors, but had a greater increase in SCD to >2.5: +29.5% (p=0.064).
Non-Survivors demonstrated a more abnormal final alpha-S-response standing, SW (-24.4% vs. -13.8% [p=0.066]), indicating greater Bar receptor Reflex dysfunction, which increases SCD risk. PE upon standing developed more significantly in survivors (+65%) vs. SCD (+29%) because initial to final standing RFa increased in survivors vs. decreasing in SCD (p=0.022). In parallel, SCD patients experienced a dramatic 59.5% decrease in resting P in addition to SW. All P- and S- final values were lower in SCD, the lowest being resting P. Since HRV=S+P, HRV was lower in SCD (p<0.0001) mainly due to lower P.
Survivors
Group-AA, Survivors with (r)-ALA: (Table 4) A1C increased (increasing oxidative stress, p=0.047), inversely proportional to (r)- ALA dosage (p=0.071); but resting RFa increased proportionally (p=0.014). Average resting Bx LFa increased (p=0.095) as did resting Bx RFa (p=0.070). HRV increased. The mean initial standing response was SW. At final testing, 4 patients’ SW were relieved (p=0.097);
Consequently, BRS improved. One more patient demonstrated PE (p=0.098) (standing RFa increased) proportional to (r)-ALA dosage.

Note: HCTZ, hydrochlorothiazide; Standing represents positive head-up posture, equivalent to head-up tilt. See Table 1 or Methods for other abbreviations.
Table 3: Comparison between Survivors and Sudden Cardiac Death patients, Mean P&S Measures. See Methods for parameters’ normal ranges.

Note: (+), improved; (-), declined; Δ, change? Demonstrated; ns, not significant (p>0.100); See Table 1 or Methods for other abbreviations.
Table 4: Mean P&S measures for DM II Survivors on (r)ALA (GroupAA).
Group-NA, Survivors without (r)-ALA: (Table 5) Similar to Group- AA, the average initial P&S levels are normal, and given their age, SB is high (but lower than Group AA and not >2.5). Contrary to Group AA, final BxLFa decreased (p=0.075), as did BxRFa (and HRV). SB increased (p=0.088). Standing, Group-NA initially demonstrated normal P- and slightly low S-responses. Individually, 57.1% demonstrated SW. Of these, 81.3% demonstrated PE. At final testing, 2 patients’ SW were relieved; 5 relieved PE, different from the Group AA patients (p<0.027).
Group-NA, Survivors without (r)-ALA: (Table 5) Similar to Group- AA, the average initial P&S levels are normal, and given their age, SB is high (but lower than Group AA and not >2.5). Contrary to Group AA, final BxLFa decreased (p=0.075), as did BxRFa (and HRV). SB increased (p=0.088). Standing, Group-NA initially demonstrated normal P- and slightly low S-responses. Individually, 57.1% demonstrated SW. Of these, 81.3% demonstrated PE. At final testing, 2 patients’ SW were relieved; 5 relieved PE, different from the Group AA patients (p<0.027).
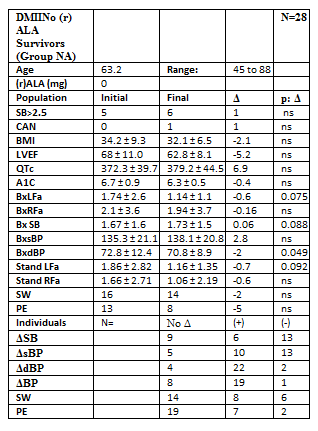
Note: (+), improved; (-), declined; Δ, change demonstrated; ns, not significant (p>0.100); See Table 1 or Methods for other abbreviations.
Table 5: Mean P&S measures for DM II Survivors not on (r)ALA (Group NA), the control group.
Survivors’ Mortality Risk: 13% Group AA patients demonstrated CAN initially, improving to 8.1%, proportional to (r)-ALA dose (p=0.004). Group AA was the only Group that increased resting BxRFa, (Table 4). Group-AA’s final RFa increased 36.2%, correlating with the dose of (r)-ALA (p=0.014). Group AA’s increase in resting BxLFa (Table 4) was mitigated by the increase in resting BxRFa, so the SB change was insignificant. Group NA had no CAN initially; increasing to 3.6%. This group’s average resting BxLFa decreased (34.5%); BxRFa fell 7.6%. SB (the average of 4 sec. ratios, not the ratio of these reported averages) significantly increased 3.6% (p=0.088), increasing MACE risk. In Tables 4 and 5, Group AA’s BxLFa and BxRFa were initially lower than Group NA’s (p<0.100), indicating lower HRV. Group AA increased both, decreasing mortality risk (Table 4). Group NA decreased both BxLFa (Table 5) (p=0.075) and BxRFa (p=ns), indicating an accelerated progression towards increased mortality risk (decreased HRV).
Non-Survivors
Group AD, Non-Survivors with (r)-ALA: (Table 6) Initial P&S levels are below normal and lowest of all Groups (lowest HRV). Given their age, SB is high (but not >2.5). Final LFa increased (p=0.047); RFa decreased (p=0.098); and SB increased to 2.72. Resting P protects against VT/VF and silent ischemia [21,32-36]; seven progressed to CAN (p=0.080), not surprising since initial BxRFa was so severely depressed. Group AD was beyond help. Standing, 57% of Group AD initially demonstrated PE; 33% ended with PE (p=0.061) and 57% ended with SW (p=0.037) indicative of BRS dysfunction (increases SCD). Finally, Group AD’s, average stand LFa was SW. These Sympathetic results are significantly similar to Group AA (p=0.061). However, the P-responses, are different (p=0.185).
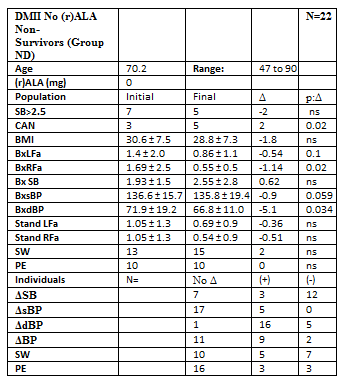
Group ND, Non-Survivors without (r)-ALA: (Table 7) Initial resting BxLFa, resting BxRFa, were normal; SB high for age (but not >2.5 Final BxLFa decreased, p=0.100; BxRFa severely decreased, p=0.020. Two more patients (67%) developed CAN (p=0.020) in spite of initially good BxRFa. Group ND’s initial standing P was normal, but S showed SW. Final average S-stand remained SW; P barely normalized. The P-responses as compared with the Group-AA are different (p=0.106).
Note: (+), improved; (-), declined; Δ, change? Demonstrated; ns, not significant (p>0.100); See Table 1or Methods for other abbreviations.
Table 6: Mean P&S measures for DM II Non-Survivors on (r)ALA (Group AD).
Note: (+), improved; (-), declined; Δ, change demonstrated; ns, not significant (p > 0.100); See Table 1or Methods for other abbreviations.
Table 7: Mean P&S measures for DM II Non-Survivors not on (r)ALA (Group ND).
Mortality Risk: Resting BxRFa decreased in both Groups (Tables 6&7): 10.5%, Group AD and 67.5%, Group ND (p=0.033); a higher risk of developing CAN. Final SB was >2.5 in both, which we have shown increases MACE 700% [18]. SB greater than 2.5 with CAN is particularly deadly in both Groups, and final average standing response was SW (impaired BRS), increasing SCD as well. BxLFa increased in Group AD (Table 6) by 109.1% vs. decreasing 38.6% in Group ND (Table 7, p=0.100), causing increased SB in Group AD.
In Group ND, despite the decrease in S, the severe decrease in resting BxRFa increased SB anyway. Two more patients had CAN. Non- survivors’ (r)ALA preserved their severely lowest P and S (LOWEST HRV) even in death. Group ND’s final BxLFa and BxRFa fell severely to the 2nd lowest among all Groups. CAN and high SB were most frequent in Groups AD and ND.
Traditional Standards Comparison: Comparing the gold standard of CARTs, without isometric hand-grip, to any abnormality of P&S Monitoring for diagnosing DAN or CAN, CARTs’ sensitivity was 48.2% of Group 1 and 30.0% of Group 2 patients; an overall unsatisfactory sensitivity of 41.4%.
Administration of (r)ALA resulted in a 43% RRR of SCD, rather than the demographics that may have favored survival in Controls. Rapid separation of the SCD curves (Figure 1) strongly implies treatment effect. Lower initial HRV, Group 1 vs. Group 2, p<0.0001, predicted SCD: AA 1.83 vs. AD 0.82, p=0.0171; NA 4.14 vs. ND 3.09,
p=0.0051. More initial CAN ((rALA 10.8% vs. Controls 6%, p=0.0013) and initial BRS dysfunction ((r)ALA 63.9% vs. Controls 58%, p=0.0044) predicted SCD better than recorded VT. (r)ALA preserved P and S vs. Controls. Those with the lowest P&S (HRV) died. Reduced HRV is a common thread in SCD Only Group AA demonstrated an increase in final, resting P (and HRV); P reduces VT/VF and silent ischemia [21,32-36], increasing 36.2% vs. a 7.6% decrease for Group NA, a 10.5% decrease for Group AD, and a 67.5% decrease for Group ND.
The progressive increase in the decline of resting P indicated mortality, from the lowest decline in resting P in Group NA, to the next greater decline in Group AD, to those with the greatest decline, Group ND (p<0.001). Changes in P were proportional to (r)ALA dose. These trends are not found in the other physiologic measures: BMI, LVEF, and QTc; and only different between the survivors’ A1Cs (Group AA vs. Group NA, p=0.034). Since SW and PE can cause both NOH and systemic HTN [9,10]. DMII patients not on (r)ALA might experience orthostasis, or labile HTN. HTN could be secondary (neurogenic), and is over twice as well controlled treating the primary SW ± PE [9] than treating the BP per se. (r)ALA preserved P and S, especially P, in survivors and non-survivors. (r)ALA is a natural, powerful thiol antioxidant. (r)ALA restores and recycles vitamins A,C,E and glutathione [9,10,34].
It improves hyperglycemia, endothelial dysfunction, nitric oxide levels (protective against VT/VF, silent ischemia [37-40]), reduces nuclear kappa B, and is essential for certain mitochondrial oxidative enzymes. (r)ALA prevents diabetic-induced reduction of the afferent limb function of the baroreceptor reflex (BR) [41], reducing MACE. SW, found in 50% to 74% of patients, failed to correct in 88% of Group NA and all SCD patients. SW disappeared substantially only in Group AA, 59.7% reduced to 53.2%, p=0.097, decreasing SCD risk. The other most common, and most important, P&S finding was low resting P in 56% to 81% of patients, improving only in Group AA (initial 56%, final 9%; p=0.070), vs. Group NA (initial 29%, final 43%; p=0.098), and worsening most severely in Group ND patients, a 67% reduction in RFa vs. 10.5% reduction in Group AD (p=0.020).
CAN decreased 37.5% in Group AA vs. an increase of 67% in Group ND. 29% of Group AD had high SB vs. 50% in Group ND (p=0.037). More CAN in Group 2 increased mortality; high SB increased mortality risk in Group 1. Group 1’s autonomic profiles generally stabilized or improved (HRV); Group 2’s deteriorated, especially a 59.5% decrease in resting P, reducing Group 2’s ability to combat VT/VF, silent ischemia, and life stresses. Standard deviations decreased over time, with the most decreases correlating with the (r)ALA dosage. The pleotropic effects of (r)ALA likely contributed to
SCD reduction. Increased nitric oxide improves P&S, endothelial dysfunction, protects against VT/VF and silent ischemia [37-40]. Decreased nitric oxide levels prolong QTc [37]. Improved mitochondrial function should reduce SCD also [42]. Asymptomatic SW (BR dysfunction) was the most common presentation of DAN. Approximately 90% of patients had HTN, presumed to be essential (primary), not possibly secondary to DAN. Ultimately, CAN with, or without, dangerously high SB can develop while under our care. How simple it is to diagnose and treat dysautonomia early; how tragic it may be not to.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
