
Research Article | DOI: https://doi.org/10.31579/jsrbi.2021/007
1Medical University Innsbruck, Innsbruck, Austria
2Private Practice, Innsbruck, Austria
3Professor and chairman, Clinical Department of Orthodontics, Innsbruck Medical University, Austria
4Division of Genetic Epidemiology, Department of Medical Genetics, Clinical and Molecular Pharmacology, Innsbruck Medical University, Austria
*Corresponding Author: Kulmer S, Medical University Innsbruck, Innsbruck, Austria
Citation: Kulmer S, Hattmannstorfer R, Niedermoser A2, Richter M and Brandstatter A, (2021) Re-Print Cephalometric Changes after Orthodontic Treatment and Fixed Oral Rehablitation in Adult Patients: 23 Years of Follow-Up. J. Scientific Research and Biomedical Informatics, 2(1); Doi:10.31579/jsrbi.2021/007
Copyright: © 2021 Kulmer S, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 February 2021 | Accepted: 15 February 2021 | Published: 22 February 2021
Keywords: occlusion; long-term changes in craniofacial structures
The aim of the present study was to investigate the long-term changes of craniofacial structures, teeth and soft-tissues after extended fixed oral rehabilitation over a period of 23 years.
Materials and Methods: A total of 15 selected patients (13 women, 2 men; mean age 42.04±10.05 years) obtained extended fixed dental restorations by utilization of the principles of the occlusal concept of sequential guidance with front-canine-dominance. The measurements were based on lateral cephalometric roentgenograms which were taken shortly, 10, 15 and 23 years after dental rehabilitation of each participant of the study. The lateral roentgenograms were traced and distances were measured with a digital calliper.
Results: The data showed an increase of 2.67 mm of the lower face height (PP-Me), the distance between the palatal plane and the incisal edge of the upper central incisor (PP-ls) increases by 1.49 mm, implying a downward movement of the upper incisors. Corresponding to these changes in the upper jaw, the distance from palatal plane to the incisal edge of the lower central incisor increases by 1.10 mm, vertical overbite increases by 0.39 mm, and the distance between Sella and Gnathion increases by 4.99 mm. The lip seal slides downward by 3.31 mm on average over 23 years after rehabilitation.
Conclusion: Significant changes in the lower face can be estimated which are in harmonious accord with the natural changes in the adult aging craniofacial complex.
Oral rehabilitation has to fulfill high claims to aesthetics and function but also should provide long-term stability. lf an extended fixed dental rehabilitation is planned a detailed diagnosis including cast and clinical functional analysis, axiography, muscle and temporo-mandibular joint (TMJ) evaluation, cephalometric analysis, and a careful treatment planning is essential [1-5]. Fixed dental rehabilitation includes the adjustment of centric occlusion in accordance with centric relation of the temporo-mandibular joint and individual calculation of cusp inclines and condylar path inclination. Based on these information an optimized construction of the guiding elements of the restoration can be created, which is best possible carried out by the occlusal concept of sequential guidance with front-canine-dominance [1-3,6]. This anterior posterior sequence of the occlusal guiding elements ensures the least muscular activity [3,7-10] and provides atraumatic and safe function of the stomatognatic system and should guarantee stability. Looked at from this point of view the patients for the present study were selected and rehabilitated with consideration for the above mentioned factors to create the best possible occlusion and function for each individual patient. The purpose of our study was to investigate the cephalometric changes in the dentofacial complex 10, 15 and 23 years after dental rehabilitation [11].
While an intensive growth, concerning the craniofacial complex, is characterizing the early childhood and adolescence until the age of 18-20 years, very small but significant changes in this complex are taking place during adulthood [12-31]. The purpose of this study is to investigate these changes of the craniofacial complex in a longterm follow-up over 23 years - the mean age of the patients is 42 to 65 years. After finishing the preprosthetic orthodontic treatment, an exactly examination of the occlusion was performed and necessary grinding of the teeth was done, so long, until a perfect occlusion was obtained. Then the patients became a fixed dental restoration (gold and/or ceramics).
Materials and Methods
This study was based on lateral cephalometric roentgenograms of individuals who obtained extended dental restorations at the department of preventive and restorative dentistry, Innsbruck Medical University, Austria. Fifteen Austrian patients (13 females and 2 males, mean age 42.04 years, SD 10.05 years) were included in this longitudinal study. The measured craniofacial variables were based on cephalometric reference points and lines shown in Figures 1-3. The measurements were evaluated from cephalograms taken immediately, 10, 15 and 23 years after fixed oral rehabilitation. All cephalometric roentgenograms were traced and distances were manually measured with a digital calliper (Mitutoyo, Tokyo, Japan).
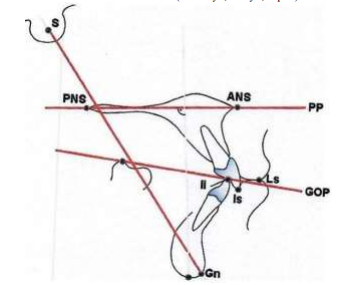
S: Sella; PNS: Spina nasalis posterior; ANS: Spina nasalis anterior; PP: Palatal plane; lP: Individual point; ls: Incisal edge of the upper central incisor; Ii: Incisal edge of the lower central incisor; LS: Lip seal; GOP: Gnathological occlusal plane; Me: Menton; Gn: Gnathion
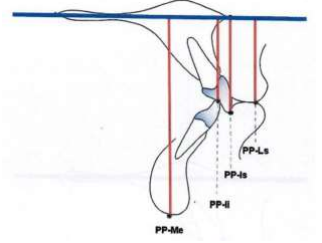
PP-Me: Distance from palatal plane to menton; PP-li: Distance from palatal plane to lower central incisor; PP-ls: Distance from palatal plane to upper central incisor; PP-LS: Distance from palatal plane to lip seal; Blue line: Palatal plane
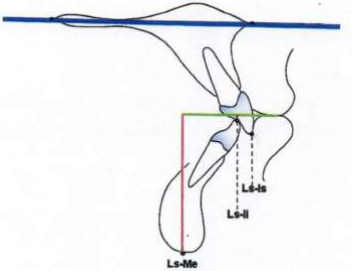
LS-Me: Distance from lip seal to menton; LS-Is: Distance from lip seal to upper central incisor; LS-Ii:
Distance from lip seal to lower central incisor; Green line: Parallel line to the Palatal plane through the lip seal
All patients attended the oral hygiene program, were diagnosed and initially treated following the guidelines for an updated diagnosis regimen of the masticatory system issued by the ARGE Prothetik und Gnathologie der Österreichischen Gesellschaft für Zahn, Mund- und Kieferheilkunde/Baden 1979 [26]. Several patients needed endodontic, periodontic or orthodontic pre-treatment. After finishing of the preprosthetic treatment and by grinding of the teeth a perfect occlusion of the patients was obtained, a fixed dental restoration (gold and/or ceramic) followed.
Statistics
Mean values and standard deviations were computed for all variables. As a non-parametric statistical test for the comparison of values obtained from the measurements of radiograms taken immediate, 10, 15 and 23 years after rehabilitation, the Friedman test was applied. Wilcoxon-tests for significant differences between single time-points were performed after a Bonferroni correction for multiple testing. All statistical analyses were performed with SPSS (version 16.0; SPSS lnc).
Results
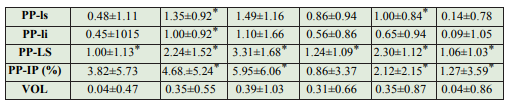
Referred to the palatal plane all measured distances showed significant increases except vertical overlap (VOL). The distance from palatal plane to menton (PP-Me) continuously increased from 67.90 mm after cementation to 68.94 mm 10 years, to 69.83 mm 15 years and to 70.57 mm 23 years after fixed rehabilitation (Table 1a). PP-Me showed a total increase of 2.67 mm at the end of the investigated time, which is statistically highly significant (Table 2a).
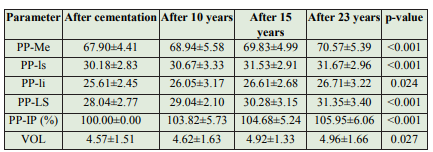

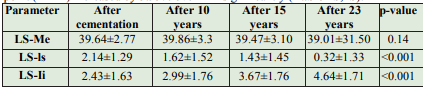
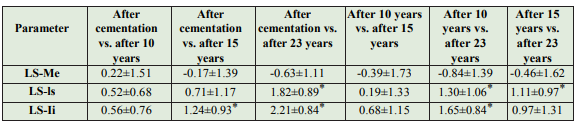
The distance from the lip seal to the incisal edge of the upper central incisors (LS-ls) decreased 1.82 mm (Table 1b,2b) and the distance to the incisal edge of the lower central incisors (LS-li) increased by 2.21 mm 23 years after cementation (Table1b,2b). The length from sella to gnathion (S-G) increased continuously by 2.29 mm after 10 years, 3.64 mm after 15 years and by 4.99 mm after 23 years post cementation. All differences in measurements were statistically significant (Table 1c,2c).

Table 1: Distances measured from various reference points

Parameters are given as mean values ± standard deviation; na: not available; *Significant after Bonferroni-correction for multiple testing (p<0.05/6 =0.008)
Table 2: Pairwise differences between time points
In this study we focused on changes of the vertical craniofacial structures in the lower face and front-teeth and their relationship to their corresponding soft-tissues to evaluate the long term-changes over 23 years after fixed oral rehabilitation with optimized occlusal conditions after the principles of the occlusal concept of sequential guidance with front-canine dominance. Harry Sicher wrote in his paper “The biology of attrition’’ in 1953: “We must not forget that even in such teeth as the growth, though limited in rate, never stops. The continued and growth of the cementum, and its accentuated increment around the root ends, is a well-known fact [32]’’. The palatal plane, as a very stable plane, was used as the main reference line for measurements in the present study. Our paper again shows this fact. Our investigation showed that the distance from the palatal plane to the incisal edge of the upper central incisors (PP-ls) increased up to 1.49 mm 23 years after cementation. These findings imply that the upper incisors are undergoing a downward movement perhaps including an enlargement of the vertical dimension of the maxilla. According to these changes the distance from the palatal plane to the incisal edge of the lower central incisors (PP-li) increases 1,10 mm over 23 years after cementation which might be a consequence of the dimensional changes of the maxilla, consequently leading to a slight increase of the vertical overbite (VOL) which was not statistically significant. Several studies showed in their investigations also an increase in overbite [16,27]. Other longitudinal studies demonstrated in their investigations that no increase of the vertical overbite could be found [22,25,30]. A possible explanation for the stability of the vertical overbite described by other authors may be natural attrition of the teeth of untreated individuals during aging. Our selection of patients obtained the individually best optimal occlusal rehabilitation in order to provide atraumatic function of the stomatognatic system without interference which is supposed to prevent attrition.
The distance from the palatal plane to menton (PP-Me) continuously increased 2,67 mm. The increasing distance from the palatal plane to menton (PP-Me) 23 years after rehabilitation is indicating a continuous downward movement of the upper jaw and lower jaw (meaning a vertical enlargement/”growing” process of the maxilla and mandible and/or eruption of the teeth) is resulting in an increase of the lower facial height. The increase of the lower face height seems to be a natural phenomenon in the adult aging craniofacial complex demonstrated also in several longitudinal studies [23,25,30]. As this observation is in accordance with other studies some authors postulate that the downward movement of the chin and a relative increase of the lower facial height is associated with a posterior rotation of the mandible because of the stability of the gonion-angle [25,30]. Responsible for the posterior rotation of the mandible might be the extrusion of teeth throughout life as a causal factor. Ainamo and Talari showed in their studies that eruption of teeth still occurs in adulthood [33]. Because of the form of nutrition of our forefathers attrition had an essential role to maintain the face height in former times [34]. Nowadays nutritional attrition is less pronounced because of today’s nourishment that continuous eruption of teeth may lead to an increase of the lower facial height.
Compared to other studies the present data showed a higher increase of the lower facial height this might be put down to the fact that our occlusal concept is thought to minimize attrition. Another explanation for the increasing lower face height could be a good chewing function. While a toothless jaw leads to bone atrophy a good masticatory function of teeth may stimulate jawbone growth by activating osteoblasts that contributes to the increase of the lower face height. The distance from sella to gnathion (S-G) also continuously increased statistically significant. At the end of the investigated period of 23 years we found an increase of nearly 5mm confirming the downward movement of chin shown in other studies [21-23,25].
Concerning the soft-tissues we found a steady increase of the distance from palatal plane to lip seal (PP-LS) of at least 3,31 mm over the investigated period of time whereas the distance from lip seal to menton (LS-Me) showed no significant change 23 years after cementation. Relating to the soft-tissues the increased lower face height is compensated by an increase of the upper lip-length. These findings coincide with other studies [22,23,25]. Because the age related downward movement of the lip seal happens to a larger amount than those of the upper central incisors the upper front teeth become more and more covered by the upper lip whereas the lower central incisors become more and more uncovered [35-37]. While the soft-tissues are undergoing a continuous change throughout the investigated period the skeletal and dentoalveolar structures are showing rather steadily increasing distances during the first 15 years after fixed dental rehabilitation followed by a tendency of slowing down of the dimensional changes. lt seems that the “growth-process” or enlargement of the aging craniofacial complex [19,20]. Continues up to a certain age and then comes to a period of stagnation or even decrease of the craniofacial dimensions [18].
Conclusion
Significant cephalometric changes in vertical dimensions in the lower face can be measured 23 years after fixed dental rehabilitation without disturbing the stability of the dental restorations [11,5]. These significant changes in the adult lower face should be taken into consideration in prosthetic treatment planning especially when single implants are included in the dental rehabilitation, because of the different behaviour of the implanted jawbone over the years compared to jawbone with natural teeth [32,38].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
